Cranial Nerves
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Imaging of Nontraumatic Temporal Bone Emergencies Nitesh Shekhrajka, MD and Gul Moonis, MD
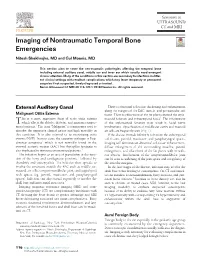
Imaging of Nontraumatic Temporal Bone Emergencies Nitesh Shekhrajka, MD and Gul Moonis, MD This section aims to cover the non-traumatic pathologies affecting the temporal bone including external auditory canal, middle ear and inner ear which usually need emergent clinical attention. Many of the conditions in this section are secondary to infections in differ- ent clinical settings with resultant complications which may leave temporary or permanent sequelae if not suspected, timely diagnosed or treated. Semin Ultrasound CT MRI 40:116-124 © 2018 Elsevier Inc. All rights reserved. External Auditory Canal There is abnormal soft tissue thickening and enhancement along the margins of the EAC, auricle, and periauricular soft Malignant Otitis Externa tissue. There is effacement of the fat planes around the stylo- his is a more aggressive form of acute otitis externa mastoid foramen and infratemporal fossa5. The involvement T which affects the elderly, diabetic, and immunocompro- of the stylomastoid foramen may result in facial nerve mised patients.1 The term “Malignant” is a misnomer used to involvement. Opacification of middle ear cavity and mastoid describe the aggressive clinical nature and high mortality in air cells are frequently seen (Fig. 1). this condition. It is also referred to as necrotizing otitis If the disease extends inferiorly to involve the subtemporal externa (NOE). In most cases, the causative pathogen is Pseu- soft tissues, parotid, masticator, and parapharyngeal spaces, domonas aeruginosa2 which is not normally found in the imaging will demonstrate abnormal soft tissue enhancement, external acoustic meatus (EAC) but Aspergillus fumigatus is diffuse enlargement of the surrounding muscles, parotid also implicated in immunocompromised patients.3 enlargement, and effacement of the fat planes with or with- The infection begins as an area of granulation at the junc- out abscess. -

Entrapment Neuropathy of the Central Nervous System. Part II. Cranial
Entrapment neuropathy of the Cranial nerves central nervous system. Part II. Cranial nerves 1-IV, VI-VIII, XII HAROLD I. MAGOUN, D.O., F.A.A.O. Denver, Colorado This article, the second in a series, significance because of possible embarrassment considers specific examples of by adjacent structures in that area. The same entrapment neuropathy. It discusses entrapment can occur en route to their desti- nation. sources of malfunction of the olfactory nerves ranging from the The first cranial nerve relatively rare anosmia to the common The olfactory nerves (I) arise from the nasal chronic nasal drip. The frequency of mucosa and send about twenty central proces- ocular defects in the population today ses through the cribriform plate of the ethmoid bone to the inferior surface of the olfactory attests to the vulnerability of the optic bulb. They are concerned only with the sense nerves. Certain areas traversed by of smell. Many normal people have difficulty in each oculomotor nerve are pointed out identifying definite odors although they can as potential trouble spots. It is seen perceive them. This is not of real concern. The how the trochlear nerves are subject total loss of smell, or anosmia, is the significant to tension, pressure, or stress from abnormality. It may be due to a considerable variety of causes from arteriosclerosis to tu- trauma to various bony components morous growths but there is another cause of the skull. Finally, structural which is not usually considered. influences on the abducens, facial, The cribriform plate fits within the ethmoid acoustic, and hypoglossal nerves notch between the orbital plates of the frontal are explored. -

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -

MBB: Head & Neck Anatomy
MBB: Head & Neck Anatomy Skull Osteology • This is a comprehensive guide of all the skull features you must know by the practical exam. • Many of these structures will be presented multiple times during upcoming labs. • This PowerPoint Handout is the resource you will use during lab when you have access to skulls. Mind, Brain & Behavior 2021 Osteology of the Skull Slide Title Slide Number Slide Title Slide Number Ethmoid Slide 3 Paranasal Sinuses Slide 19 Vomer, Nasal Bone, and Inferior Turbinate (Concha) Slide4 Paranasal Sinus Imaging Slide 20 Lacrimal and Palatine Bones Slide 5 Paranasal Sinus Imaging (Sagittal Section) Slide 21 Zygomatic Bone Slide 6 Skull Sutures Slide 22 Frontal Bone Slide 7 Foramen RevieW Slide 23 Mandible Slide 8 Skull Subdivisions Slide 24 Maxilla Slide 9 Sphenoid Bone Slide 10 Skull Subdivisions: Viscerocranium Slide 25 Temporal Bone Slide 11 Skull Subdivisions: Neurocranium Slide 26 Temporal Bone (Continued) Slide 12 Cranial Base: Cranial Fossae Slide 27 Temporal Bone (Middle Ear Cavity and Facial Canal) Slide 13 Skull Development: Intramembranous vs Endochondral Slide 28 Occipital Bone Slide 14 Ossification Structures/Spaces Formed by More Than One Bone Slide 15 Intramembranous Ossification: Fontanelles Slide 29 Structures/Apertures Formed by More Than One Bone Slide 16 Intramembranous Ossification: Craniosynostosis Slide 30 Nasal Septum Slide 17 Endochondral Ossification Slide 31 Infratemporal Fossa & Pterygopalatine Fossa Slide 18 Achondroplasia and Skull Growth Slide 32 Ethmoid • Cribriform plate/foramina -

Morphometric Analysis of Stylomastoid Foramen Location and Its Clinical Importance
Dental Communication Biosc.Biotech.Res.Comm. Special Issue Vol 13 No 8 2020 Pp-108-111 Morphometric Analysis of Stylomastoid Foramen Location and its Clinical Importance Hemanth Ragav N V1 and Yuvaraj Babu K2* 1Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai- 600077, India 2Assistant Professor, Department of Anatomy, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Science, Saveetha University, Chennai- 600077, India ABSTRACT The stylomastoid foramen is located between the styloid process and mastoid process of the temporal bone. Facial nerve and Stylomastoid branch of posterior auricular artery passes through this stylomastoid foramen. The facial nerve can be blocked at this stylomastoid foramen but it has high risk of nerve damage. For Nadbath facial nerve block, stylomastoid foramen is the most important site. Facial canal ends at this foramen and it is the important motor portion of this stylomastoid foramen. A total of 50 dry skulls from the Anatomy Department of Saveetha Dental College were studied to locate the position of the centre of the stylomastoid foramen with respect to the tip of mastoid process and the articular tubercle of the zygomatic arch by a digital vernier caliper. All measurements were tabulated and statistically analysed. In our study, we found the mean distance of stylomastoid foramen from mastoid processes 16.31+2.37 mm and 16.01+2.08 mm on right and left. Their range is 10.48-23.34 mm and 11.5-21.7 mm. The mean distance of stylomastoid foramen from articular tubercle is 29.48+1.91 mm and 29.90+1.62 mm on right and left. -

Atlas of the Facial Nerve and Related Structures
Rhoton Yoshioka Atlas of the Facial Nerve Unique Atlas Opens Window and Related Structures Into Facial Nerve Anatomy… Atlas of the Facial Nerve and Related Structures and Related Nerve Facial of the Atlas “His meticulous methods of anatomical dissection and microsurgical techniques helped transform the primitive specialty of neurosurgery into the magnificent surgical discipline that it is today.”— Nobutaka Yoshioka American Association of Neurological Surgeons. Albert L. Rhoton, Jr. Nobutaka Yoshioka, MD, PhD and Albert L. Rhoton, Jr., MD have created an anatomical atlas of astounding precision. An unparalleled teaching tool, this atlas opens a unique window into the anatomical intricacies of complex facial nerves and related structures. An internationally renowned author, educator, brain anatomist, and neurosurgeon, Dr. Rhoton is regarded by colleagues as one of the fathers of modern microscopic neurosurgery. Dr. Yoshioka, an esteemed craniofacial reconstructive surgeon in Japan, mastered this precise dissection technique while undertaking a fellowship at Dr. Rhoton’s microanatomy lab, writing in the preface that within such precision images lies potential for surgical innovation. Special Features • Exquisite color photographs, prepared from carefully dissected latex injected cadavers, reveal anatomy layer by layer with remarkable detail and clarity • An added highlight, 3-D versions of these extraordinary images, are available online in the Thieme MediaCenter • Major sections include intracranial region and skull, upper facial and midfacial region, and lower facial and posterolateral neck region Organized by region, each layered dissection elucidates specific nerves and structures with pinpoint accuracy, providing the clinician with in-depth anatomical insights. Precise clinical explanations accompany each photograph. In tandem, the images and text provide an excellent foundation for understanding the nerves and structures impacted by neurosurgical-related pathologies as well as other conditions and injuries. -

Topographical Anatomy and Morphometry of the Temporal Bone of the Macaque
Folia Morphol. Vol. 68, No. 1, pp. 13–22 Copyright © 2009 Via Medica O R I G I N A L A R T I C L E ISSN 0015–5659 www.fm.viamedica.pl Topographical anatomy and morphometry of the temporal bone of the macaque J. Wysocki 1Clinic of Otolaryngology and Rehabilitation, II Medical Faculty, Warsaw Medical University, Poland, Kajetany, Nadarzyn, Poland 2Laboratory of Clinical Anatomy of the Head and Neck, Institute of Physiology and Pathology of Hearing, Poland, Kajetany, Nadarzyn, Poland [Received 7 July 2008; Accepted 10 October 2008] Based on the dissections of 24 bones of 12 macaques (Macaca mulatta), a systematic anatomical description was made and measurements of the cho- sen size parameters of the temporal bone as well as the skull were taken. Although there is a small mastoid process, the general arrangement of the macaque’s temporal bone structures is very close to that which is observed in humans. The main differences are a different model of pneumatisation and the presence of subarcuate fossa, which possesses considerable dimensions. The main air space in the middle ear is the mesotympanum, but there are also additional air cells: the epitympanic recess containing the head of malleus and body of incus, the mastoid cavity, and several air spaces on the floor of the tympanic cavity. The vicinity of the carotid canal is also very well pneuma- tised and the walls of the canal are very thin. The semicircular canals are relatively small, very regular in shape, and characterized by almost the same dimensions. The bony walls of the labyrinth are relatively thin. -

Detection of Perineural Spread: Fat Is a Friend
AJNR: 19, September 1998 EDITORIALS 1385 head and neck coil has considerable appeal, and such viding the “payoff” of very rapid coronal slab se- “combo coils” will soon be widely used. At the very quences obtained sequentially, while maintaining sig- least, the current “conventional” cervical-cranial nificantly high intravascular signal to limit flow- MRA techniques can be supplemented with the tech- related artifacts. Thus, LeClerc et al take another step nique described by LeClerc et al for evaluation of the up the stairway, the top of which is the complete aortic arch and proximal cervical vasculature. Second, replacement of conventional angiography with MRA with further technical development, it is likely that for evaluation of cerebrovascular disease. coverage can be extended to allow visualization of the ostia and the carotid siphons in one acquisition. Newer contrast agents that do not exit the intravas- MICHAEL BRANT-ZAWADZKI,MD cular space will optimize the ability to do repeated Hoag Memorial Hospital Presbyterian MR sequences after only a single injection, thus pro- Newport Beach, California Detection of Perineural Spread: Fat Is a Friend One could easily argue that the search for perineu- affected foramen, enhancement of the nerve, mass ral tumor spread is the most important task of the effect in the Meckel’s cave region, and obliteration of radiologist examining a patient with head and neck the fat in the pterygopalatine fossa. I would like to carcinoma. emphasize the importance of this last finding: oblit- Certainly the description of a primary tumor site is eration of normal fat just external to the neural fora- important. -

Level I to III Craniofacial Approaches Based on Barrow Classification For
Neurosurg Focus 30 (5):E5, 2011 Level I to III craniofacial approaches based on Barrow classification for treatment of skull base meningiomas: surgical technique, microsurgical anatomy, and case illustrations EMEL AVCı, M.D.,1 ERINÇ AKTÜRE, M.D.,1 HAKAN SEÇKIN, M.D., PH.D.,1 KUTLUAY ULUÇ, M.D.,1 ANDREW M. BAUER, M.D.,1 YUSUF IZCI, M.D.,1 JACQUes J. MORCOS, M.D.,2 AND MUSTAFA K. BAşKAYA, M.D.1 1Department of Neurological Surgery, University of Wisconsin–Madison, Wisconsin; and 2Department of Neurological Surgery, University of Miami, Florida Object. Although craniofacial approaches to the midline skull base have been defined and surgical results have been published, clear descriptions of these complex approaches in a step-wise manner are lacking. The objective of this study is to demonstrate the surgical technique of craniofacial approaches based on Barrow classification (Levels I–III) and to study the microsurgical anatomy pertinent to these complex craniofacial approaches. Methods. Ten adult cadaveric heads perfused with colored silicone and 24 dry human skulls were used to study the microsurgical anatomy and to demonstrate craniofacial approaches in a step-wise manner. In addition to cadaveric studies, case illustrations of anterior skull base meningiomas were presented to demonstrate the clinical application of the first 3 (Levels I–III) approaches. Results. Cadaveric head dissection was performed in 10 heads using craniofacial approaches. Ethmoid and sphe- noid sinuses, cribriform plate, orbit, planum sphenoidale, clivus, sellar, and parasellar regions were shown at Levels I, II, and III. In 24 human dry skulls (48 sides), a supraorbital notch (85.4%) was observed more frequently than the supraorbital foramen (14.6%). -

Variations in the Morphology of Stylomastoid Foramen: a Possible Solution to the Conundrum of Unexplained Cases of Bell’S Palsy S.K
Folia Morphol. Vol. 80, No. 1, pp. 97–105 DOI: 10.5603/FM.a2020.0019 O R I G I N A L A R T I C L E Copyright © 2021 Via Medica ISSN 0015–5659 eISSN 1644–3284 journals.viamedica.pl Variations in the morphology of stylomastoid foramen: a possible solution to the conundrum of unexplained cases of Bell’s palsy S.K. Ghosh , R.K. Narayan Department of Anatomy, All India Institute of Medical Sciences, Phulwarisharif, Patna, Bihar, India [Received: 12 January 2020; Accepted: 2 February 2020] Background: Stylomastoid foramen is the terminal part of facial canal and is the exit gateway for facial nerve from skull base. We hypothesized that anatomical variations of this foramen could be a risk factor for the injury of facial nerve re- sulting in unilateral facial nerve paralysis or Bell’s palsy. Hence the present study was conducted to study the variations in size and shape of stylomastoid foramen in dry adult human skulls. Materials and methods: The study was conducted on 37 dry adult human skulls of unknown age and sex. High resolution images of the skulls under study were processed by ImageJ software and observations were undertaken. Results: Total eight variations of stylomastoid foramen were observed in terms of shape. The common variants were round, oval and square (present in 83.79% skulls on right side and 81.07% skulls on left side), whereas the rare variants were triangular, rectangular, serrated, bean-shaped and irregular. It was noted that stylomastoid foramen were associated with extensions (45.95% skulls) and also adjacent foramen (18.92% skulls). -

Ch07a Axial Skeleton
CHAPTER 7 AXIAL SKELETON Skeletal System • Bones – axial skeleton • skull , vertebral column , ribs – appendicular skeleton • upper extremities , shoulder girdle • lower extremities , pelvic girdle • Cartilage • joints , discs • growth plates • Joints • Fibrous connective tissue ligaments periosteum bone markings – bumps • bumps for muscle attachments = process – tubercle – tuberosity – trochanter – epicondyle – spine • bumps forming joints – head – facet – condyle holes and dips in bones • indentations: – fissure – groove – sulcus – fossa • holes – foramen – foramina – canal – meatus Skull • = cranium + facial bones • cranium – protect the brain , ear – cranial vault = calvarium – cranial floor • facial bones – protect sensory organs : eye, nose, mouth – attach facial muscles cranial bones • frontal • parietal • temporal • occipital • sphenoid • ethmoid facial bones • mandible • maxilla • zygomatic • nasal • lacrimal • vomer • palatine • inferior nasal conchae temporal bone • squamous portion • zygomatic portion – zygomatic process – mandibular fossa • mastoid portion – mastoid process – styloid process – external acoustic meatus – stylomastoid foramen • petrous portion – inner ear ; internal acoustic meatus – carotid canal occipital bone • floor, posterior wall of cranial cavity • occipital condyles joint with vertebral column • foramen magnum passage for spinal cord • basilar portion (clivus) • hypoglossal canal • external occipital protuberance • superior , inferior nuchal lines sphenoid bone • greater wing • lesser wing • pterygoid -

Anatomy Lab: the Skeletal System Part I: Vertebrae and Thoracic Cage
ANA Lab: Bone 1 Anatomy Lab: The skeletal system Part I: Vertebrae and Thoracic cage Spine (Vertebrae) Body Vertebral arch Vertebral canal Pedicle Lamina Spinous process Transverse process Sup. articular facets Inf. articular facets Sup. vertebral notch Inf. vertebral notch Intervertebral foramen Cervical vertebrae: 7 Typical (C3-C6) Transverse foramen C1, Atlas C2, Axis: dens C7 Thoracic vertebrae: 12 Typical (T2-T10) T1 T11, 12 Lumbar vertebrae: 5 Typical (L1-4) Sacrum: 5 Ala Anterior sacral foramina Posterior sacral foramina Sacral canal ANA Lab: Bone 2 Sacral hiatus promontory median sacral crest intermediate crest lateral crest Coccyx Horns Transverse process Thoracic cages Ribs: 12 pairs Typical ribs (R3-R10): Head, 2 facets intermediate crest neck tubercle angle costal cartilage costal groove R1 R2 R11,12 Sternum Manubrium of sternum Clavicular notch for sternoclavicular joint body xiphoid process ANA Lab: Bone 3 Part II: Skull and Facial skeleton Skull Cranial skeleton, Calvaria (neurocranium) Facial skeleton (viscerocranium) Overview: identify the margin of each bone Cranial skeleton 1. Lateral view Frontal Temporal Parietal Occipital 2. Cranial base midline: Ethmoid, Sphenoid, Occipital bilateral: Temporal Viscerocranium 1. Anterior view Ethmoid, Vomer, Mandible Maxilla, Zygoma, Nasal, Lacrimal, Inferior nasal chonae, Palatine 2. Inferior view Palatine, Maxilla, Zygoma Sutures: external view vs. internal view Coronal suture Sagittal suture Lambdoid suture External appearance of skull Posterior view external occipital protuberance