Nutritional Status and Morbidity Among School Going
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Solid Waste Management Exposure Workshop for Urban Local Bodies Of
Title of the report Final Report 2018TR15 Solid waste management exposure workshop for urban local bodies of Uttar Pradesh under Swachh Bharat Mission of the Government of India Proceeding of workshop at Agra, 27-29 November, 2018 Supported by / Prepared for National Institute of Urban Affairs (NIUA) i © The Energy and Resources Institute 2018 Suggested format for citation T E R I. 2018 Solid waste management exposure workshops for ULBs of Uttar Pradesh New Delhi: The Energy and Resources Institute. 353 pp. [Project Report No. 2018RT15] For more information Project Monitoring Cell T E R I Tel. 2468 2100 or 2468 2111 Darbari Seth Block E-mail [email protected] IHC Complex, Lodhi Road Fax 2468 2144 or 2468 2145 New Delhi – 110 003 Web www.teriin.org India India +91 • Delhi (0)11 ii Table of contents 1. INTRODUCTION ....................................................................................................................... 1 1.1 Workshop at Agra ............................................................................................................ 2 2. PROCEEDINGS ............................................................................................................................ 4 2.1 Number of Participants ................................................................................................... 4 2.2 Profile of Participants ....................................................................................................... 5 2.3 Consolidated Feedback ................................................................................................... -

O.I.H. Government of India Ministry of Housing & Urban Affairs Lok Sabha Unstarred Question No. 3376 to Be Answered On
O.I.H. GOVERNMENT OF INDIA MINISTRY OF HOUSING & URBAN AFFAIRS LOK SABHA UNSTARRED QUESTION NO. 3376 TO BE ANSWERED ON JANUARY 01, 2019 SLUMS IN U.P. No. 3376. SHRI BHOLA SINGH: Will the Minister of HOUSING AND URBAN AFFAIRS be pleased to state: (a) whether slums have been identified in the State of Uttar Pradesh, as per 2011 census; (b) if so, the details thereof, location-wise; and (c) the number of people living in the said slums? ANSWER THE MINISTER OF STATE (INDEPENDENT CHARGE) OF THE MINISTRY OF HOUSING & URBAN AFFAIRS [SHRI HARDEEP SINGH PURI] **** (a) to (c): As per the Census-2011, number of slum households was 10,66,363 and slum population was 62,39,965 in the State of Uttar Pradesh. City-wise number of slum households and slum population in the State of Uttar Pradesh are at Annexure. ****** Annexure referred in reply to LSUQ No. 3376 due for 1.1.2018 City -wise number of Slum Households and Slum Population in the State of Uttar Pradesh as per Census 2011 Sl. Town No. of Slum Total Slum Area Name No. Code Households Population 1 120227 Noida (CT) 11510 49407 2 800630 Saharanpur (M Corp.) 12308 67303 3 800633 Nakur (NPP) 1579 9670 4 800634 Ambehta (NP) 806 5153 5 800635 Gangoh (NPP) 1277 7957 6 800637 Deoband (NPP) 4759 30737 7 800638 Nanauta (NP) 1917 10914 8 800639 Rampur Maniharan (NP) 3519 21000 9 800642 Kairana (NPP) 1731 11134 10 800643 Kandhla (NPP) 633 4128 11 800670 Afzalgarh (NPP) 75 498 12 800672 Dhampur (NPP) 748 3509 13 800678 Thakurdwara (NPP) 2857 18905 14 800680 Umri Kalan (NP) 549 3148 15 800681 Bhojpur Dharampur -

Bareilly Dealers Of
Dealers of Bareilly Sl.No TIN NO. UPTTNO FIRM - NAME FIRM-ADDRESS 1 09107300009 BE0001281 RAJ CROCKERY CENTER HOSPITAL ROAD BAREILLY 2 09107300014 BE0008385 SUPER PROVISION STORE PANJABI MARKET, BAREILLY. 3 09107300028 BE0006987 BHATIA AGEMCIES 89 CIVIL LINES, BAREILLY. 4 09107300033 BE0010659 VIJAY KIRANA STORE SUBHAS NAGAR BY 5 09107300047 BE0001030 MUKUT MURARI LAL WOOD VIKRATA CHOUPLA ROAD BY 6 09107300052 BE0008979 GARG BROTHERS TOWN HALL BAREILLY. 7 09107300066 BE0001244 RAJ BOOK DEPOT SUBHAS MKT BY 8 09107300071 BE0000318 MONICA MEDICAL STORE 179, CIVIL LINES, BAREILLY. 9 09107300085 BE0001762 RAM KUMAR SUBASH CHAND AONLA ,BAREILLY. 10 09107300090 BE0009124 GARU NANA FILLING STN KARGANA BAREILLY. 11 09107300099 BE0005657 KHANDUJA ENTERPRISES GANJ AONLA,BAREILLY. 12 09107300108 BE0004857 ADARSH RTRADING CO. CHOPUPLA ROAD BY 13 09107300113 BE0007245 SWETI ENTERPRISES CHOUPLA ROAD BY 14 09107300127 BE0011496 GREEN MEDICAL STORE GHER ANNU KHAN AONLA BAREILLY 15 09107300132 BE0002007 RAMESHER DAYAL SURENDRA BHAV AONLA BAREILLY 16 09107300146 BE0062544 INDIAN FARMERS FERTILISERS CORP AONLA, BAREILLY. LTD 17 09107300151 BE0007079 BHARAT MECH STORE BALIA AONLA, BAREILLY. 18 09107300165 BE0011395 SUCHETA PRAKASHAN MANDIR BAZAR GANJ AONLA BAREILLY 19 09107300170 BE0003628 KICHEN CENTER & RAPAIRS JILA PARISAD BY 20 09107300179 BE0006421 BAREILLY GUN SERVICE 179/10 CIVIL LINES,BAREILLY 21 09107300184 BE0004554 AHUJA GAS & FAMILY APPLIANCES 179 CIVIL LINES, BAREILLY. 22 09107300198 BE0002360 IJAAT KHA CONTRACTOR SIROLY AONLA BAREILLY. 23 09107300207 BE0003604 KRISHAN AUTAUR CONTRACTOR BAMANPURI BAREILLY. 24 09107300212 BE0009945 PUSTAK MANDIR SUBASH MKT BY 25 09107300226 BE0005758 NITIN FANCY JEWELERS CANAAT PLACE MKT BY 26 09107300231 BE0005520 DEHLI AUTO CENTER CAROLAAN CHOUPLA ROAD BY 27 09107300245 BE0003248 KHANN A PLYWOOD EMPORIUM CIVIL LINES, BAREILLY. -

List of Class Wise Ulbs of Uttar Pradesh
List of Class wise ULBs of Uttar Pradesh Classification Nos. Name of Town I Class 50 Moradabad, Meerut, Ghazia bad, Aligarh, Agra, Bareilly , Lucknow , Kanpur , Jhansi, Allahabad , (100,000 & above Population) Gorakhpur & Varanasi (all Nagar Nigam) Saharanpur, Muzaffarnagar, Sambhal, Chandausi, Rampur, Amroha, Hapur, Modinagar, Loni, Bulandshahr , Hathras, Mathura, Firozabad, Etah, Badaun, Pilibhit, Shahjahanpur, Lakhimpur, Sitapur, Hardoi , Unnao, Raebareli, Farrukkhabad, Etawah, Orai, Lalitpur, Banda, Fatehpur, Faizabad, Sultanpur, Bahraich, Gonda, Basti , Deoria, Maunath Bhanjan, Ballia, Jaunpur & Mirzapur (all Nagar Palika Parishad) II Class 56 Deoband, Gangoh, Shamli, Kairana, Khatauli, Kiratpur, Chandpur, Najibabad, Bijnor, Nagina, Sherkot, (50,000 - 99,999 Population) Hasanpur, Mawana, Baraut, Muradnagar, Pilkhuwa, Dadri, Sikandrabad, Jahangirabad, Khurja, Vrindavan, Sikohabad,Tundla, Kasganj, Mainpuri, Sahaswan, Ujhani, Beheri, Faridpur, Bisalpur, Tilhar, Gola Gokarannath, Laharpur, Shahabad, Gangaghat, Kannauj, Chhibramau, Auraiya, Konch, Jalaun, Mauranipur, Rath, Mahoba, Pratapgarh, Nawabganj, Tanda, Nanpara, Balrampur, Mubarakpur, Azamgarh, Ghazipur, Mughalsarai & Bhadohi (all Nagar Palika Parishad) Obra, Renukoot & Pipri (all Nagar Panchayat) III Class 167 Nakur, Kandhla, Afzalgarh, Seohara, Dhampur, Nehtaur, Noorpur, Thakurdwara, Bilari, Bahjoi, Tanda, Bilaspur, (20,000 - 49,999 Population) Suar, Milak, Bachhraon, Dhanaura, Sardhana, Bagpat, Garmukteshwer, Anupshahar, Gulathi, Siana, Dibai, Shikarpur, Atrauli, Khair, Sikandra -
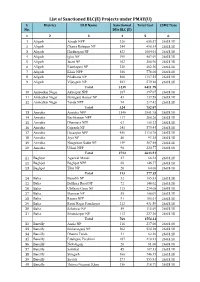
List of Sanctioned BLC(E) Projects Under PMAY(U) S
List of Sanctioned BLC(E) Projects under PMAY(U) S. District ULB Name Sanctioned Total Cost CSMC Date No. DUs BLC (E) 1 2 3 4 5 6 1 Aligarh Atrauli NPP 320 655.57 26.03.18 2 Aligarh Charra Rafatpur NP 244 498.54 26.03.18 3 Aligarh Harduaganj NP 822 1684.01 26.03.18 4 Aligarh Iglas NP 199 407.69 26.03.18 5 Aligarh Jatari NP 102 208.96 26.03.18 6 Aligarh Kauriaganj NP 228 462.36 26.03.18 7 Aligarh Khair NPP 380 778.00 26.03.18 8 Aligarh Pilakhana NP 560 1137.55 26.03.18 9 Aligarh Vijaygarh NP 283 579.10 26.03.18 Total 3138 6411.78 10 Ambedkar Nagar Akbarpur NPP 187 397.07 26.03.18 11 Ambedkar Nagar Iltifatganj Bazaar NP 43 137.58 26.03.18 12 Ambedkar Nagar Tanda NPP 94 217.42 26.03.18 Total 324 752.07 13 Amroha Amroha NPP 1546 3801.98 26.03.18 14 Amroha Bachharaon NPP 117 288.26 26.03.18 15 Amroha Dhanaura NPP 63 155.22 26.03.18 16 Amroha Gajraula NP 241 575.45 26.03.18 17 Amroha Hasanpur NPP 456 1110.70 26.03.18 18 Amroha Joya NP 40 93.25 26.03.18 19 Amroha Naugawan Sadat NP 159 387.88 26.03.18 20 Amroha Ujhari NPP 90 220.77 26.03.18 Total 2712 6633.51 21 Baghpat Agarwal Mandi 27 66.52 26.03.18 22 Baghpat Baghpat NPP 60 146.77 26.03.18 23 Baghpat Tikri NP 26 64.06 26.03.18 Total 113 277.35 24 Balia Bansdih NP 52 105.83 26.03.18 25 Balia Belthara Road NP 72 146.02 26.03.18 26 Balia Chitbara Gaon NP 115 234.08 26.03.18 27 Balia Maniyar NP 55 108.09 26.03.18 28 Balia Rasara NPP 91 185.61 26.03.18 29 Balia Reoti Nagar Panchayat 212 431.59 26.03.18 30 Balia Sahatwar NP 59 115.69 26.03.18 31 Balia Sikanderpur NP 112 227.30 26.03.18 Total 768 1554.21 32 Bareilly Anola NP 116 237.00 26.03.18 33 Bareilly Bisharatganj NP 262 534.10 26.03.18 34 Bareilly Dhaura Tanda 31 62.36 26.03.18 35 Bareilly Fatehganj Pacshimi 107 218.23 26.03.18 36 Bareilly Nawabganj 26 61.06 26.03.18 37 Bareilly Sainthal 45 107.13 26.03.18 38 Bareilly Shisgarh 366 746.55 26.03.18 39 Bareilly Sirauli 273 555.81 26.03.18 40 Bareilly Thiriya Nizamat Khan 156 318.79 26.03.18 S. -
Ramganga Basin Plan Volume - Ii
STATE WATER RESOURCES AGENCY (SWaRA) Government of Uttar Pradesh DEVELOPMENT OF RIVER BASIN ASSESSMENT AND PLANS FOR ALL MAJOR RIVER BASINS IN UTTAR PRADESH RAMGANGA BASIN PLAN VOLUME - II March 2020 Prepared & Submitted By : TAHAL Consulting Engineers Ltd. in Joint Venture with INRM Consultants Pvt. Ltd. Government of Uttar Pradesh SWaRA State Water Resources Agency Development of River Basin Assessment and Plans for all Major River Basins in Uttar Pradesh Ramganga Basin Plan (Volume-II) March 2020 Development of BAPS for UP Major River Basins Ramganga Basin Plan Development of River Basin Assessment and Plans for all Major River Basins in Uttar Pradesh Ramganga Basin Plan (Volume-II) List of Appendices Page Appendix 1 : Districts and Blocks Falling within Ramganga Basin and its Sub Basins ...... 1 Appendix 2 : Population Distribution in Ramganga Basin by Administrative Units (Census 2011) ..................................................................................................... 10 Appendix 3 : SC, ST and BPL Population Distribution in Ramganga Basin by Administrative Units (Census 2011) ................................................................ 15 Appendix 4 : Land Holdings in Ramganga Basin by Administrative Units ........................ 20 Appendix 5 : Towns in Ramganga Basin ................................................................................ 25 Appendix 6 : Workers Population in Ramganga Basin by Administrative Units (Census 2011) .................................................................................................... -

State Urban Development Agency (Suda)
REQUEST FOR PROPOSAL (RFP) FOR SELECTION OF CONSULTANT FOR ADDITIONAL WORK OF PREPARING DETAILED PROJECT REPORT (DPR) AND PROVIDING PMC SERVICES UNDER BENEFICIARY LED CONSTRUCTION IN 653 ULB’S UNDER PRADHAN MANTRI AWAS YOJANA - HOUSING FOR ALL (URBAN) IN UTTAR PRADESH RFP No. : 81/03/29/HFA/2018-19 Date: 06/04/2018 Particulars Date Time Date of Publication of RFP 08/04/2018 - Date and Time of Pre - Bid Meeting 20/04/2018 11:00 a.m. Last date & time for uploading of RFP by bidder 01/05/2018 02:00 p.m. Last date & time of submission of RFP cost & EMD 01/05/2018 02:00 p.m. Date & time for opening of Technical Bids 01/05/2018 03:00 p.m. Note: Draft for Cost of RFP and EMD to be kept in a single envelope to be dropped in the tender box kept at State Urban Development Authority, SUDA office at Lucknow STATE URBAN DEVELOPMENT AGENCY (SUDA) Sector – 7, Gomti Nagar Extension, Near UP Dial 100 Office, Lucknow REQUEST FOR PROPOSAL (RFP) FOR SELECTION OF CONSULTANT FOR ADDITIONAL WORK OF PREPARING DETAILED PROJECT REPORT (DPR) AND PROVIDING PMC SERVICES UNDER BENEFICIARY LED CONSTRUCTION IN 653 ULB’S UNDER PRADHAN MANTRI AWAS YOJANA - HOUSING FOR ALL (URBAN) IN UP STATE URBAN DEVELOPMENT AGENCY (SUDA) Sector – 7, Gomti Nagar Extension, Near UP Dial 100 Office, Lucknow Phone: 0522-2286709 Fax – 0522-2286711 Website: http://www.sudaup.org RFP No. : 81/03/29/HFA/2018-19 Date: 06/04/2018 1. Director, State Urban Development Agency invites technical and financial proposals from eligible Consultancy Firms/agencies/companies for additional work of Preparation of Detailed Project Report (DPR) and providing PMC services for Projects under Beneficiary Led Construction in 653 ULB’s in Uttar Pradesh. -

Religion, Part IV-B (Ii), Series-25, Uttar Pradesh
CENSUS OF INDIA 1991 SERIES - 25 UTTAR PRADESH PART IV - B(ii} RELIGION (TABLE C-9) DIRECTORATE OF CENSUS OPERATIONS UTTAR PRADESH CONTENTS Pages PREFACE v ACKNOWLEDGEMENT vII INTRODUCTORY NOTE 2 Note on Religion Table 27 C-9-Rellglon Table 28-243 APPENDICES AppendIx A -Details of religions shown under 'Other rellafons and 247-254 persuasions' having population of 100 or more at State level In main rellafon table. Appendix 8 - Details of religions shown under 'Other rellafons and 255-257 persuasIons' having population less than 100 at State level In main rellafon table. An nexu re - Details of Sects/Belief/Religions dubbed with another religion 261-274 which Is shown at the head of the table In block letters. (III) PREFACE The present volume gives the religious composition of the population of Uttar Pradesh with sexwlse break up separately for the State, Districts, Tahsils and Urban Agglomerations/Towns as revealed by 1991 Census. This report presents Information In respect of six major religious communities namely Hindus, Sikhs, Muslims, Jalns, Christians, Buddhists, "Other Religions and Persuasions" and" Religion not Stated". The CensUs Operations of 1991 were carried out In UP under the direction of Sri Vijender aut;lAS. The compilation of religion data was done under the supervision of Deputy Dlr n the Regional Tabulation Offices. The tlnallsatlon of Religion Table, Appendices and An~e etc. were done In Census Division of the Directorate under the supervision and . guidance of S/Sri K.C. Upadhyaya and Ram Sa hal, Asstt. Directors. The names of members of staff of this Directorate, who were closely associated with the work are given separately. -

RO MO/EC Office Name Address 1 220000 LUCKNOW RO LUCKNOW
S.N Office FI Addres RO MO/EC Office Name Address O Code TOWNS s 2 43, 1 220000 LUCKNOW RO LUCKNOW 3RD FLOOR, JEEVAN BHAVAN HAZRA TGANJ 8, Balmiki Marg, Lal Bagh, Luckno 2 220014 LUCKNOW SVC LUCKNOW Lucknow w 17/03 MEGHDOOT BUILDING, 3 220012 LUCKNOW SVC KANPUR THE MALL, KANPUR, ALLHA 4 220013 LUCKNOW SVC ALLAHABAD 16-A, MG MARG, CIVIL LINES BAD 43, 5 220022 LUCKNOW TP HB LUCKNOW 3RD FLOOR, JEEVAN BHAVAN HAZRA TGANJ 17/03, MEGHDOOT BUILDING, 6 220023 LUCKNOW TP HUB KANPUR MALL, KANPUR 16 A, MG MARG, CIVIL LINES , Allahab 7 220024 LUCKNOW TP HUB ALLAHABAD ALLAHABAD ad 22- VIKASDEEP, 9TH FLOOR, 8 221100 LUCKNOW DO 2 LUCKNOW STATIO STATION ROAD, LUCKNOW NROAD 8, BALMIKI MARG, LALBAGH, LUCKN 9 221112 LUCKNOW CBO 2 LUCKNOW LUCKNOW. OW sahu 10 221113 LUCKNOW CBO-4, LUCKNOW 184/135,3rd floor plaza Bldg. YUSUF MAHAL, SABJI MANDI, 11 221191 LUCKNOW FI MO MO, MALIHABAD MIRZA GANJ,MALIHABAD DurgaGanj Crossing, Hardoi 12 221192 LUCKNOW FI MO MO KAKORI road Near Matiyari Crossing, Beside 13 221300 LUCKNOW DO-3, LUCKNOW Union Bank of India, Faizabad Road, Lucknow Above Basant Cinema, Mayfair 14 221301 LUCKNOW CBO-1, LUCKNOW Extension Bldg. , Lucknow Indira Market, Station Road, 15 221302 LUCKNOW BO BARABANKI Barabanki 8, Balmiki Marg, Lal Bagh, 16 221306 LUCKNOW CBO5, LUCKNOW Lucknow MAMAPUR, NEXT TO JANTA 17 221395 LUCKNOW FI MO MO DEVA DHARAM KANTA, BARABANKI ROAD, DEVA, PIN: 225301 18 221397 LUCKNOW FI MO MO DARIYABAD Makdum Zadgan,Quasba 19 221399 LUCKNOW FI MO MO SIDDHAUR Shideshwar Crossing, S iddaur Opp. -

Pradhan Mantri Awas Yojana (PMAY-U)
Pradhan Mantri Awas Yojana (PMAY-U) Proposal for 20 projects with 18598 EWS Houses under Vertical-3 AHP Proposal for 282 projects with 102047 validated Beneficiaries under Vertical 4 – BLC (N) Presented to 29th CSMC Dated 27-12-2017 State Urban Development Agency (SUDA), Government of Uttar Pradesh PROGRESS OF PMAY (U) Indicators Current Status (No.) . Cities Approved 653 Nos . Total Application Received after De duplication 27,34,293 . Total Physical Validation completed in ULB’s 539 ULBs . Total no of Applications physically Validated 17,70,594 . Demand Survey Completed . 465 ULBs . SECC 2011 data linkage 28% average . Cases accepted/rejected (including deduplication) 5,89,736/4,09,497 (7,71,361 entry is in process) . Whether HFAPoA Submitted 69 cities . Whether AIP Submitted No . Whether HFAPoA & AIP entered in MIS Under Progress . SLTC/CLTC staffs approved vs. placed SLTC/CLTC staff will be placed by next month. Target of DUs in 2017-18 5,00,000 Dus . State Budgetary Provision for PMAY (U) in 2017-18 3000 Cr. STATUS OF MANDATORY CONDITIONS Mandatory conditions Current Status .Dispensing the need for separate Non Agricultural (NA) Permission Complied .Prepare/amend their Master Plans earmarking land for Under Progress Affordable Housing .Single-window, time bound clearance for layout approval and Complied building permissions .Adopt the approach of deemed building permission and layout Complied approval on the basis of pre-approved lay outs and building plans. .Amend or legislate existing rent laws on the lines of the Model Under Progress Tenancy Act. .Additional Floor Area Ratio (FAR)/Floor Space Index (FSI)/ Provision for Transferable Development Rights (TDR) and relaxed density norms. -
State Urban Development Agency Government of Uttar Pradesh
State Urban Development Agency Government of Uttar Pradesh Letter No.- /tl ]6 /01/29lHF A/2020:21 Date*- i4 /12/2020 Minutes of Meeting of 8lnstate Level Appraisal Committee (SLAC) for Housing for A hetd on 14.12.2020. Housing for All Plan of Action under "Pradhan Mantri Awas Yojaoa (Urban)" has been appraised by the State Level Appraisal Comrnittee (SLAC). After discussion, SLAC has appraised the I{FAPoA put up by the State Level Noclal Agency and recommends the approval of following for SLSMC: N0 Agra Achhnera NPP 0 173 50 65 50 338 7.09 1.65 1.58 2 Agra Dayalbagh NP 0 164 267 57 0 488 9.24 3.24 5.83 3 Agra Etmadpur NPP 0 49 179 68 46 342 5.70 2.93 4.18 4 Agra '158 Fatehabad NP 0 74 47 0 279 6.03 1.21 1.88 5 Agra Fatehpursikri NPP 0 116 131 381 0 628 10.78 5.12 5.90 6 Agra Jagner NP 0 248 241 101 30 620 12.20 3.72 5.70 '7 Agra Kheragarh NP 0 370 26 96 44 536 12.37 1.66 I.JO 8 Agra Kkawali NP 0 1'13 47 132 0 292 5.70 1.79 2.08 9 Agra Pinahat NP 0 308 72 273 58 711 14.27 4.03 3.81 10 Agra Samshabad NPP t.t 0 155 71 27 274 5.92 1 .'19 1.04 It Agra Swamibagh NP 0 3 6 0 0 9 0.17 0.06 0.12 12 Agra Wah NPP 0 155 21 71 27 274 5.92 1 .19 1.04 1J Aligarh Aligarh NN 4459 73196 22498 15734 765 116652 2539.29 416.02 654.50 t4 Barabanki Subeha NP 0 38 81 102 10 231 3.91 1.88 2.49 I) Bareilly Anwala NPP 0 129 16 180 116 441 8.12 3.12 2.80 l6 Bareilly BaheriNPP 0 478 62 205 46 791 17.46 3.13 3.96 l'7 Bareilly Dhaura Tanda NP 0 144 20 356 JI 551 9.95 4.07 5.06 Bareilly Faridpur NP 0 25 4 51 6 86 1.58 0.6'1 0.75 l9 Bareilly Fatehganj Purvi NP 0 19 1 -

Pradhan Mantri Awas Yojna (Urban) Projects Sanctioned Till 43Rd CSMC of BLC (N) S
Pradhan Mantri Awas Yojna (Urban) Projects Sanctioned till 43rd CSMC of BLC (N) S. Sanctioned CSMC District ULB Name No DUs 1 26th CSMC Dt. 27.09.2017 Agra Achhnera 65 2 36th CSMC Dt. 23-07-2018 Agra Achhnera 136 3 38th CSMC Dt. 26-09-2018 Agra Achhnera 35 4 43rd CSMC Dt. 25-02-2019 Agra Achnera 368 5 26th CSMC Dt. 27.09.2017 Agra Agra 2237 6 29th CSMC Dt. 27-12-2017 Agra Agra 2153 7 31st CSMC Dt. 27-02-2018 Agra Agra 869 8 36th CSMC Dt. 23-07-2018 Agra Agra 3742 9 38th CSMC Dt. 26-09-2018 Agra Agra 4693 10 43rd CSMC Dt. 25-02-2019 Agra Agra 1084 11 25th CSMC Dt. 23.08.2017 Agra Bah 71 12 31st CSMC Dt. 27-02-2018 Agra Bah 45 13 36th CSMC Dt. 23-07-2018 Agra Bah 83 14 38th CSMC Dt. 26-09-2018 Agra Bah 187 15 43rd CSMC Dt. 25-02-2019 Agra Bah 277 16 25th CSMC Dt. 23.08.2017 Agra Dayalbagh 57 17 25th CSMC Dt. 23.08.2017 Agra Etmadpur 68 18 31st CSMC Dt. 27-02-2018 Agra Etmadpur 87 19 36th CSMC Dt. 23-07-2018 Agra Etmadpur 369 20 38th CSMC Dt. 26-09-2018 Agra Etmadpur 611 21 42nd CSMC Dt. 30-01-2019 Agra Etmadpur 1365 22 24th CSMC Dt. 24.07.2017 Agra Fatehabad 47 23 29th CSMC Dt. 27-12-2017 Agra Fatehabad 102 24 38th CSMC Dt. 26-09-2018 Agra Fatehabad 187 25 25th CSMC Dt.