Sexual Assault Laws in South Carolina
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Chain of Custody
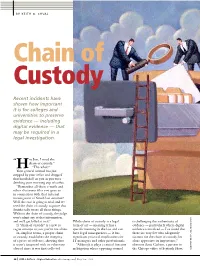
BY KEITH G. CHVAL Chain of Custody Recent incidents have shown how important it is for colleges and universities to preserve evidence — including digital evidence — that may be required in a legal investigation. ey Jon, I need the “ chain of custody.” H “The what?” Your general counsel has just stopped by your office and dropped that bombshell on you as you were drinking your morning cup of coffee. “Remember all those e-mails and other electronic files you gave us in connection with that internal investigation of Smith last summer? Well, the case is going to trial, and we need the chain of custody to prove that Smith really wrote all those things. Without the chain of custody, the judge won’t admit any of that information, and we’ll get killed at trial.” While chain of custody is a legal is challenging the authenticity of If “chain of custody” is a new or term of art — meaning it has a evidence — particularly where digital vague concept to you, you’re not alone. specific meaning in the law and can evidence is involved — I’ve found that AEL HENDERSON AEL In simplest terms, a proper chain have legal consequences — it has there are very few who adequately L of custody establishes the integrity significant practical implications for account for the chain of custody, let of a piece of evidence, showing that IT managers and other professionals. alone appreciate its importance,” it wasn’t tampered with or otherwise “Although it plays a critical function observes Scott Carlson, a partner in altered since it was first collected. -
19-Cr-00008-NR Document 2581 Filed 12/21/20 Page 1 of 3
Case 2:19-cr-00008-NR Document 2581 Filed 12/21/20 Page 1 of 3 IN THE UNITED STATES DISTRICT COURT FOR THE WESTERN DISTRICT OF PENNSYLVANIA UNITED STATES OF AMERICA ) ) v. ) 2:19-cr-8-NR ) OMARI PATTON, ) ) ) Defendant. ) MEMORANDUM ORDER Omari Patton and 47 co-defendants are charged with engaging in a large-scale conspiracy to traffic a variety of Schedule I, II, and III controlled substances, including heroin, cocaine, fentanyl, and synthetic cannabinoids. Mr. Patton has requested leave to file a motion to suppress certain laboratory test results and other items that the Federal Bureau of Prisons seized, including card stock and other paper that was believed to have been soaked in controlled substances. ECF 1774; ECF 1810. After carefully considering the parties’ submissions, the Court will grant Mr. Patton leave to file his motion to suppress, but will deny the motion without prejudice to Mr. Patton reasserting his objections at or around the time of trial. Mr. Patton’s primary argument is that “the Government failed to properly preserve” the cards and paper seized and later lab tested because of “numerous and serious errors in the chain of custody.” ECF 1810, ¶¶ 4-6. Mr. Patton claims that “[p]hysical evidence must be authenticated before being admitted into evidence.” Id. at ¶ 7. He also claims that the substantial “break” in the chain of custody here makes this authentication impossible. Id. at ¶ 31. The government, however, correctly points out that “[a]uthentication objections, like other trial objections, are assessed according to the applicable Federal Rules of Evidence, including Rules 104(a) and 901(a),” and there is “no requirement that the proponent [of evidence] do so before the evidence is presented at trial[.]” ECF 1879, at ¶ 22. -

Chain of Custody Specimen Collection Instructions
DEPARTMENT OF PATHOLOGY AND LABORATORY MEDICINE CHAIN OF CUSTODY SPECIMEN COLLECTION INSTRUCTIONS Chain of custody specimens can be used as evidence in court as the specimen is collected in the presence of a witness, sealed to prevent tampering and all handling/possession of specimen is recorded on the form from collection to testing. Testing Available Drugs of Abuse Microbiology Drugs of Abuse Screen 5, CoC, Meconium, LAB7379 Chlamydia trachomatis and Neisseria gonorrhea PCR (CTNG PCR), Urine, LAB7166 Confirmed Drug Abuse Panel 9, CoC, Urine, LAB8020 Rapid Plasma Reagin w/ Reflex Titer (RPR), Blood, LAB7452 All Specimen Types 1. Place appropriate Chain of Custody test order in Epic 2. Microbiology samples can be ordered with or without Chain of Custody. Compete the following items in Epic when ordering testing for Chain of Custody: • Chain of Custody? Mark box “Yes” 3. Obtain Chain of Custody kit from the Laboratory: Anschutz Campus – 720-777-6711 North Campus – 720-478-5250 South Campus – 720-478-6711; 303-201-0155 (after-hours pager) Receive Chain of Custody Kit. Ensure all required items are included. Meconium Kit: Urine Kit: Blood Kit: • Chain of custody bag • Chain of custody bag • Chain of custody bag • Stool specimen container • Plastic cup • Red top vacutainer tube • Security label • 60-mL bottle • Security label • Chain of custody form • Security tape • Chain of custody form • Temperature slip • Chain of custody form 4. Complete Chain of Custody Form 5. Identify witness and obtain witness signature 6. Collect specimen: Meconium: Urine: Blood: • Place 1.0 to 5.0 • Collect specimen in provided cup or pediatric bag • Venipuncture or grams meconium in • Pour specimen into 60-mL transport bottle. -

Case: 4:11-Cv-00454-DCN Doc #: 40 Filed: 03/28/14 1 of 46. Pageid
Case: 4:11-cv-00454-DCN Doc #: 40 Filed: 03/28/14 1 of 46. PageID #: <pageID> UNITED STATES DISTRICT COURT NORTHERN DISTRICT OF OHIO EASTERN DIVISION JOHN E. WOLFF, JR., ) CASE NO. 4:11-cv-0454 ) Petitioner, ) JUDGE NUGENT ) v. ) MAGISTRATE JUDGE VECCHIARELLI ) TERRY TIBBALS, ) ) REPORT AND RECOMMENDATION Respondent. ) This matter is before the magistrate judge pursuant to Local Rule 72.2(b)(2). Before the court is the petition of John E. Wolff, Jr., (“Petitioner”) for a writ of habeas corpus filed pursuant to 28 U.S.C. § 2254. Petitioner is in the custody of the Ohio Department of Rehabilitation and Correction pursuant to journal entry of sentence in the case of State of Ohio vs. Wolff, Case No. 06-CR-978 (Mahoning County Aug. 29, 2007). (Doc. No. 23-10.) For the reasons set forth below, it is recommended that the petition be dismissed with prejudice. I. Relevant Factual Background The state appellate court that reviewed Petitioner’s conviction and sentence recited the following facts: On September 14, 2006, Wolff was indicted on ten counts of rape, in violation of R.C. 2907.02(A)(1)(b)(B), special felony (Counts 1-10); three counts of rape, in violation of R.C. 2907.02(A)(2)(B), 1st degree felony (Counts 11-13); five counts of gross sexual imposition, in violation of R.C. 2907.05(A)(4)(B), 3rd degree felony (Counts 14-18); and two counts of gross sexual imposition, in violation of R.C. Case: 4:11-cv-00454-DCN Doc #: 40 Filed: 03/28/14 2 of 46. -

GUIDE to NEW YORK EVIDENCE ARTICLE 11 REAL and DEMONSTRATIVE EVIDENCE TABLE of CONTENTS 11.01 Real Evidence 11.03 Demonstrative
GUIDE TO NEW YORK EVIDENCE ARTICLE 11 REAL AND DEMONSTRATIVE EVIDENCE TABLE OF CONTENTS 11.01 Real Evidence 11.03 Demonstrative Evidence 11.05 Anatomically Correct Dolls 11.07 Childs Age 11.09 Demonstrations and Experiments 11.11 Personal Appearance & Capability 11.13 Photographs 11.15 Viewing of Premises 11.17 Exhibits to the Jury 11.01. Real Evidence (1) Definition. Real Evidence refers to any tangible object or sound recording of a conversation that is offered in evidence. (2) Admissibility. Real evidence is admissible upon a showing that it is relevant to an issue in the proceeding, is what it purports to be, and has not been tampered with. Proof that an object has not been tampered with and is what it purports to be depends on the nature of the object and, in particular, whether the object is patently identifiable, or fungible. (a) Patently identifiable evidence. When real evidence possesses unique or distinctive characteristics or markings and is not subject to material alteration that is not readily apparent, evidence identifying the object normally will constitute the requisite proof. (b) Fungible evidence. When real evidence is fungible, capable of being altered, contaminated, or replaced, or is a sound recording, in addition to testimony identifying the object, proof that the proffered evidence has not been tampered with is required and may be satisfied by: (i) a chain of custody (i.e. testimony of those persons who handled the object or recording from the time it was obtained or recorded to the time it is presented in court to identify the object or recording and attest to its unchanged condition); or (ii) proof of circumstances that provide reasonable assurances of the identity and unchanged condition of the object or recording. -

WHO Background Paper Obstacles to Women Accessing Forensic Medical Exams in Cases of Sexual Violence by A. Widney Brown, Advocac
WHO Background Paper Obstacles to Women Accessing Forensic Medical Exams in Cases of Sexual Violence By A. Widney Brown, Advocacy Director, Women’s Rights Division, Human Rights Watch Final Version Introduction The international community awoke to the realization that “women’s rights are human rights” when women’s rights activists from all over the world took center stage at the World Conference on Human Rights held in Vienna in 1993. They seized the initiative at the conference by focusing on violence against women and the failure of states to provide redress for the violence suffered. At a tribunal held at the NGO parallel conference, women from numerous countries stepped forward to describe their experiences as victims of sexual and gender based violence. They also described the failure of the state to condemn the violence, to protect women from further violence and to provide redress through the criminal justice system. The pervasiveness of violence against women is breathtaking in developing and developed countries alike.1 The litany of harms inflicted is long: female genital mutilation, forced marriages, trafficking into forced labor, domestic violence, so-called honor killings, acid burning, dowry deaths, and finally, in every culture, rape and other crimes of sexual violence. The U.N. Convention on the Elimination of all forms of Discrimination against Women adopted in 1979, called on States to “take in all fields appropriate measures, including legislation, to ensure the full development and advancement of women, for the purpose -
Chain-Of-Custody Considerations By: SSA William A
Chain-of-Custody Considerations By: SSA William A. Zinnikas, FBI/NYO/JTTF Chain-of-custody is the ability to give an accurate accounting in a court of law as to the manner in which evidence was acquired, maintained, transported, examined, etc., by whom, when, where, and for what purpose. Chain-of-custody describes a process as testified to by an individual who offers real evidence in a court of law and can account for the evidence from the moment it reached his/her custody until it is offered as evidence in court. Chain-of-custody bears on the weight of the evidence, not its admissibility. Just because you don’t have a chain-of-custody process doesn’t mean that the evidence is inadmissible. Admissibility is determined by the manner in which the evidence was acquired. (It must be legally obtained! “Fruit of the poisoned tree,” etc.) The emphasis is on the individual, not the process. A process alone does not create chain-of-custody. Any documentation merely supports the person’s testimony with respect to the handling of the evidence. Chain-of-custody can be perfect, or imperfect. Even if the process is faulty, a chain-of-custody could still be established. Chain-of-custody is more of a concept than a precise formula. (“It’s all about believability!”) waz 02/26/2003 Technically, chain-of-custody only applies to sworn law enforcement officers. However, if a laboratory is assisting law enforcement in an investigation, the laboratory could be construed by the court as an “agent” of law enforcement. -

What Should Be Documented As a Part of the SANE/SAFE Evidentiary Examination?
Linsa E. Ledray, RN, SANE-A, PhD, FAAN Documentation: What should be documented as a part of the SANE/SAFE Evidentiary Examination? Prior to the development of SANE programs in the mid 1970’s the paperwork in the evidentiary exam kits was developed by crime laboratories with the intent of obtaining the information the criminal laboratory needed to analyze the evidence collected in the kit. Most kits also included a release of information for the patient to sign giving the hospital permission to release the evidence collected to law enforcement, who then transported the evidence to the crime laboratory for analysis. Hospital emergency staff would often complete this paperwork and provide little additional information to law enforcement, unless there were injuries requiring treatment, which only occurred in fewer than 7% of the cases across studies (Ledray, 1999; Littel, 2001). As SANE programs developed it became clear to these nurses that valuable information was being missed and that additional information should to be documented and included as a part of the evidence collection. In some states an attempt was made to include this additional information in crime laboratory paperwork provided in the evidentiary exam kit and in other areas SANE programs developed additional sexual assault exam forms that they completed and provided to law enforcement with the evidentiary exam kits. As a result there is no standard documentation and information gathered varies considerably both in content and format. This paper will address what to needs to be documented and how it should be documented. It will also discuss address the question, is it possible to document too much information? 1 Linsa E. -

SEXUAL ASSAULT: an Acute Care Protocol for Medical/Forensic Evaluation
STATE OF NEW HAMPSHIRE OFFICE OF THE ATTORNEY GENERAL SEXUAL ASSAULT: An Acute Care Protocol for Medical/Forensic Evaluation Ninth Edition, 2018 http://doj.nh.gov/criminal/victim-assistance/documents/acute-care- protocol.pdf HISTORY OF THE NEW HAMPSHIRE SEXUAL ASSAULT PROTOCOL PROJECT On April 26, l988, the New Hampshire Legislature passed RSA 21-M:8-c, which made the State responsible for the payment of forensic medical examinations of sexual assault victims when there is no insurance (See Appendix A). Under RSA 21-M:8-c the New Hampshire Department of Justice (Attorney General’s Office) is authorized to “implement rules establishing a standardized sexual assault protocol and kit to be used by all physicians or hospitals in this state when providing physical examinations of victims of alleged sexual offenses.” This Protocol is a statutory mandate for all hospitals and physicians in the state. In 1989, the New Hampshire Attorney General's Office formed the Sexual Assault Protocol Committee representing the medical, legal, law enforcement, victim advocacy and forensic science communities, to establish a New Hampshire protocol and kit. The Committee took great care to make recommendations based upon the physical and emotional needs of the sexual assault victim, reasonably balanced with the basic requirements of the legal system. The result was the publication of Sexual Assault: A Protocol for Medical and Forensic Examination, and a standardized evidence collection kit to be used in all of the hospitals in the state. This project was completed in June 1989. Recognizing that forensic science is a field in continual evolution, the Protocol is continually being revised in an effort to improve evidence collection outcomes for patients who have experienced sexual assault. -

1 Cheryl Howell School of Government Evidence Issues in Domestic Court Special Topic Seminar for District Court Judges April
1 Cheryl Howell School of Government Evidence Issues in Domestic Court Special Topic Seminar for District Court Judges April 2010 Discussion Questions and Suggested Answers 1(a). Child custody case where child has lived primarily with mother: During the direct examination of mother, her lawyer asks if the 10 year-old child has told the mother where the child prefers to live. Father’s attorney objects. Sustained or overruled? Answer: Probably overruled. Mother can testify as to what child told her about where the child prefers to live, unless you find it should be excluded pursuant to Rule 403 as unduly prejudicial. Relevance? Statement of child‟s preference is relevant if the child is of an age and capacity to form an intelligent and rational view on the matter. Hinkle v. Hinkle, 266 N.C. 189 (1966); In re Pearl, 305 N.C. 640 (1982)(nine year child old enough to form opinion). But compare Daniels v. Hatcher, 46 N.C . App. 481 (1980)(judge did not abuse his discretion in refusing to hear testimony from children ages 7, 8 and 12) with Kearnes v. Kearnes, 6 N.C. App. 319 (1969)(judge erred in refusing to hear testimony of children ages 7, 9, 11 and 12). Hearsay? If child testifies, the statement of the child to the mother will be offered to corroborate the in-court statement of the child. The statement will not be hearsay because it is offered for a non-hearsay purpose. See Rule 801(c). See State v. Aycock, 310 N.C. 1 (1984); State v. -

Military Rules of Evidence
PART III MILITARY RULES OF EVIDENCE SECTION I GENERAL PROVISIONS Rule 101. Scope the error materially prejudices a substantial right of (a) Scope. These rules apply to courts-martial the party and: proceedings to the extent and with the exceptions (1) if the ruling admits evidence, a party, on the stated in Mil. R. Evid. 1101. record: (b) Sources of Law. In the absence of guidance in (A) timely objects or moves to strike; and this Manual or these rules, courts-martial will apply: (B) states the specific ground, unless it was (1) First, the Federal Rules of Evidence and the apparent from the context; or case law interpreting them; and (2) if the ruling excludes evidence, a party in- (2) Second, when not inconsistent with subdivi- forms the military judge of its substance by an offer of proof, unless the substance was apparent from the sion (b)(1), the rules of evidence at common law. context. (c) Rule of Construction. Except as otherwise pro- (b) Not Needing to Renew an Objection or Offer of vided in these rules, the term “military judge” in- Proof. Once the military judge rules definitively on cludes the president of a special court-martial the record admitting or excluding evidence, either without a military judge and a summary court-mar- before or at trial, a party need not renew an objec- tial officer. tion or offer of proof to preserve a claim of error for appeal. Discussion (c) Review of Constitutional Error. The standard Discussion was added to these Rules in 2013. The Discussion provided in subdivision (a)(2) does not apply to er- itself does not have the force of law, even though it may describe rors implicating the United States Constitution as it legal requirements derived from other sources. -
Daubert Standard
TheWildlife Forensic Expert: A Prosecutor’s Perspective Environmental Crimes Section Environment and Natural Resources Division, U.S. Department of Justice We use forensic experts in wildlife cases for: Class characterization/species i.d. Individualization Necropsy/cause of death Toolmarks/bullet-gun matching Graphic display/trial exhibits Serology Wildlife cases are different from other criminal cases -No victim to testify or “represent” in court -Wildlife law is usually outside comfort zone of judges and general prosecutors - “Harm” issues are different from human cases: Why care about a smuggled snake? Or an electrocuted hawk? Or an oiled duck? Or a shot wolf? -How do I retain credibility in court as a prosecutor of wildlife cases? Purpose of this discussion Provide some insight into how wildlife crime prosecutors view these cases; Charging decisions How the process works The specific evidence rules concerning expert testimony How you can make your forensic witness an effective witness First, a few questions: Is the witness an advocate or a conduit for accurate findings/science? Is your forensic witness’s analysis affected by any bias? What type of witness are you dealing with? e.g., Research scientist vs. Law Enforcement vs. Forensic Scientist? • Best practices? • Error rates? • Accreditation? Chain of Custody Issues are Paramount in Forensics… “Crime scene to courtroom:” unbroken, provable chain of possession for fungible items. Objective is to prove the thing in the courtroom is the same thing that was collected at the crime scene and same thing that was tested. Weak or broken chain of custody may prevent admission of evidence and your analysis, or create doubt.