Calf-Head Sign in Miyoshi Myopathy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Table of Contents - Current Issue
Open access journal indexed with Index Medicus Users online: 3815 Home | Login Current Ahead of Online About Archive Search Instructions Subscribe Videos Etcetera Contact Issue print Submission Navigate here » Table of Contents - Current issue » Search November-December 2018 View issue as eBook » Current Issue Volume 66 | Issue 6 Issue statistics » Submit Article Page Nos. 1539-1876 RSS » My Preferences Online since Wednesday, November 28, 2018 Accessed 1,250 times. PDF access policy Full text access is free in HTML pages; however the journal allows PDF access only to users from INDIA and paid subscribers. EPub access policy Full text in EPub is free except for the current issue. Access to the latest issue is reserved only for the paid subscribers. Show all abstracts Show selected abstracts Export selected to Add to my list NI FEATURE: THE FIRST IMPRESSION - COMMENTARY The cover page p. 1539 DOI:10.4103/0028-3886.246290 [HTML Full text] [PDF] [Mobile Full text] [EPub] [Sword Plugin for Repository]Beta NI FEATURE: TIMELESS REVERBERATIONS - COMMENTARY My journey in the field of neurosurgery and its changing trends p. Sushil Kumar 1540 DOI:10.4103/0028-3886.246232 [HTML Full text] [PDF] [Mobile Full text] [EPub] [Sword Plugin for Repository]Beta NI FEATURE: JOURNEY THROUGH THE EONS - COMMENTARY Professor B. Ramamurthi (1922-2003): Personal reminiscences p. Prakash N Tandon 1543 DOI:10.4103/0028-3886.246297 [HTML Full text] [PDF] [Mobile Full text] [EPub] [Sword Plugin for Repository]Beta Tuberculous meningitis: Challenges in diagnosis and p. management: Lessons learnt from Prof. Dastur's article 1550 published in 1970 Manish Modi, Manoj Kumar Goyal, Anumiti Jain, Suhalika Singhal Sawhney, Kusum Sharma, Sameer Vyas, Chirag Kamal Ahuja DOI:10.4103/0028-3886.246224 [ABSTRACT] [HTML Full text] [PDF] [Mobile Full text] [EPub] [Sword Plugin for Repository]Beta GUEST COMMENTARY Generational tensions are a distraction from addressing the p. -

Dormant Account 10 Years and Above As on Ashadh 2076
Everest Bank Limited Head Office, Lazimpat 14th Aug 2019 DORMANT ACCOUNT 10 YEARS AND ABOVE AS ON ASHADH 2076 SN A/C NAME CURRENCY 1 BIRENDRA & PUNAMAYA EUR 2 ROBERT PRAETZEL EUR 3 NABARAJ KOIRALA EUR 4 SHREE NAV KANTIPUR BAHUUD NPR 5 INTERCONTINENTAL KTM HOTE NPR 6 KANHIYALAL & RAJESH OSWAL NPR 7 LAXMI HARDWARE NPR 8 NAVA KSHITIZ ENTERPRISES NPR 9 SWADESHI VASTRA BIKRI BHA NPR 10 UNNAT INDUSTRIES LTD. NPR 11 RAJ PHOTO STUDIO NPR 12 RND ENTERPRISES NPR 13 LUMBINI RESORT AND HILL D NPR 14 ARUNODAY POLYPACK IND. NPR 15 UNNAT INDUSTRIES PVT.LTD. NPR 16 KRISHNA MODERN DAL UDYOG NPR 17 TIRUPATI DISTRIB. CONCERN NPR 18 LAXMI GALLA KATTA KHARID NPR 19 URGN HARDWARE CONCERN. NPR 20 AASHMA COOPERATIVE FINANC NPR 21 VERITY PRINTERS(P)LT NPR 22 PUZA TRADERS NPR 23 NEPAL MATCH MANUFACTURER NPR 24 G.B TEXTILE MILLS PVT. LT NPR 25 VISION 9PRODUCT. (P) L.-R NPR 26 PHOOLPATI ENTERPRISES NPR 27 ROSHI SAVING & CREDIT CO. NPR 28 SHRESTHA TRD.GROUP P.LTD. NPR 29 P.D.CONSULT (PARTNERS FOR NPR 30 N.Y.S.M.S RELIEF FUND NPR 31 ASHOK WIRE PVT. LTD NPR 32 PAWAN KRISHNA HARDWARE ST NPR 33 OCEAN COMPUTER PVT. LTD. NPR 34 CHHIGU MULTIPURPOSE CO-OP NPR 35 GAJENDRA TRADERS NPR 36 SURENDRA KARKI NPR 37 GATE WAY INT'L TRADERS NPR 38 VYAHUT COMMERCIAL TRADERS NPR 39 SAPTA KOSHI SAV.&CR. CO.L NPR 40 MHAIPI HOSIERY NPR 41 STYLE FOOTWEARS P LTD NPR 42 MINA IMPEX NPR 43 CUSTOM CLEARANCE SERVICE NPR 44 HOTEL LA DYNASY PVT. -

HOMELESSNESS ABOUT BUTTERFLIES Children in News Homelessness
HOMELESSNESS ABOUT BUTTERFLIES Children in News Homelessness VOL. XXIV, 2015 HIS NAME IS TODAY Years V 1989 -2014 OL. XXIV , 2015 U-4, Green Park Extension, New Delhi-110016 CHILDREN IN NEWS VOL XXIV, 2015 1 Tel.: 26163935, 26191063 E-mail: [email protected] Delhi Child Rights Club The Delhi Child Rights Club (DCRC) was launched by BUTTERFLIES in 1998. There was a need to have a children's forum in Delhi where children could articulate their issues and collectively take action to get their entitlements which is rightfully theirs. BUTTERFLIES invited children of NGOs working with children based in Delhi to be part of this forum. The response to this invitation was encouraging. Today there are children from 15 NGOs who are members In the little world in which and in recent times children from various neighbourhoods have attended DCRC meetings. The primary objective of DCRC is to have children's voices heard by civil society and policy makers, their views on issues children have their existence pertaining to their lives be taken seriously, and to consult them on all issues related to their welfare, development and protection. DCRC is open to all children of Delhi under 18 years of age whether from working whosoever brings them up,there is class, middle class or upper class background or a child living in an institution. A city-wide Child Rights Club is one mechanism where by children can work together towards the creation of a child safe and nothing so finely perceived and so friendly city. The children envisage a city where children's rights to respect, dignity, opportunities, growth, development and protection are ensured. -

Indian Council of Medical Research New Delhi © 2005 Indian Council of Medical Research
Annual Report 2003-2004 Indian Council of Medical Research New Delhi © 2005 Indian Council of Medical Research Prof. N.K. Ganguly: Director-General Dr. K. Satyanarayana: Chief (Publication & Information) Complied and Edited by Dr. Sudha Chauhan, DDG (SG) Published by the Division of Publication, Information and Communication on behalf of the Director-General, Indian Council of Medical Research New Delhi 110029 Layout Design & Production Control by ICMR Press Unit Printed at: S. Narayan & Sons, B-88, Okhla Indl. Area, Phase-II, New Delhi Tel: 26385873 he Indian Council of Medical Research has made significant strides in its mandate of ‘Research for TBetter Health’. The Council has lived up to country’s expectations on all major fronts of its activity: research and development of vaccines and drugs for infectious diseases like tuberculosis, malaria, filariasis, HIV/AIDS, research in the areas of modern biology like molecular biology, genomics, bioinformatics, fertility regulation, cancer and other non-communicable diseases, consultancy and human resource development, national and international collaborations and biomedical informatics and communication. During the period under report, the Memorandum for the Expenditure Finance Committee (EFC) of ICMR has been approved by the Government of India and Rs.870 Crores have been allocated for the 10th Plan. The research activities will now be pursued with greater vigour as more funding would be available. To optimize resource utilization, the Council is using the Combined Approach Matrix being used by Global Health Forum for Health Research for setting research priorities in various disciplines. The Council continued to play an important role in detecting new and emerging infections in India like the Chandipura virus encephalitis in Andhra Pradesh and Gujarat and outbreak of mysterious fever in Siliguri. -
Pdf Web Notice for to Advt. No.-Cimfr 06-2020
lh,lvkbZvkj&dsUnzh; [kuu ,oa bZa/ku vuqla/kku laLFkku CSIR-CENTRAL INSTITUTE OF MINING & FUEL RESEARCH cjok jksM] /kuckn@ Barwa Road, Dhanbad fnukad% 08-06-2021 osc lwpuk foKkiu la[;k flEQj&06@2020 ds rgr rduhdh vf/kdkjh@xzqi& III(3) in (indksM& MIN/TO/20, CHML/TO/20, CSE/TO/20, ECE/TO/20, CVL/TO/20, ENVT/TO/20, MET/TO/20 ) gsrq izkIr vkosnuksa ds Nkuchu (Screening) ds i'pkr V~zsM VsLV gsrq 'kkWVZfyLVsM (Shortlisted) ,oa ukWV 'kkWVZfyLVsM (Not Shortlisted) mEehnokjksa dh lwpha rFkk 'kkWVZfyfLVax ekinaM (Criteria) iksLVdksM ds vuqlkj layXud&1 (Annexure-I) esa iznf'kZr dh xbZ gSA rFkkfi] fdlh mEehnokj dks iznf'kZr lwpuk ds laca/k esa fdlh Hkh rjg dh vkifRr gks rks nLrkosth lk{; (tgka ykxw gks) dk;kZy; dks jftLVMZ@LihM iksLV vFkok bZ&esy [email protected] ij izsf"kr djsa] tks fd bl dk;kZy; dks fnukad 30 -06 -2021 la/;k 05%30 rd vo'; izkIr gks tk,A mDr frfFk ,oa le; ds ckn izkIr ;k fcuk lk{; vkifRr ij fdlh Hkh rjg dk fopkj ugha fd;k tk,xkA nwjHkk"k ,oa vU; ek/;e ls ntZ vkifRr Lohdk;Z ugha gksaxsA bl in gsrq izkIr vkosnu i=ksa esa nh xbZ ik=rk laca/kh lHkh tkudkfj;ksa ,oa ?kks"k.kkvksa dh lR;rk lkfcr djus dh ftEesnkjh Lo;a mEehnokjksa dh gksxhA lwph iw.kZ lko/kkuh ds lkFk rS;kj dh xbZ gS] ;n~;fi dksbZ [email protected] xyfr;kWa jg xbZ gks rks] lh,lvkbZvkj&flEQj fdlh Hkh Lrj ij mls lq/kkjus dk vf/kdkj lqjf{kr j[krk gSA mi;qZDr in gsrq ijh{kk (V~zsM ,oa fyf[kr ) dk vk;kstu lh,lvkbZvkj ds i=kad 5-1(315)/2015-PD ] fnukad 01-03-2019 }kjk tkjh vn~;ru ikB~;dze ,oa ijh{kk izfdz;k ds vuqlkj dh tk,xhA V~zsM VsLV ,oa fyf[kr ijh{kk dk ikB~;dze lHkh lacaf/krksa dks lwpukFkZ layXud&AA (ANNEXURE-II) esa layXu gSA lHkh vH;kosnu ds lkFk vkosnu i= Hksts tkus ls lacaf/kr Mkd foHkkx dh jlhn (Receipt) vo'; layXu fd;k tkuk pkfg,A foKkiu la[;k flEQj&06@2020 }kjk foKkfir mi;qZDr in ,oa vU; lHkh in gsrq vn~;ru lwpuk laLFkku dh osclkbZV www.cimfr.nic.in ij le;≤ ij iznf'kZr dh tk,xhA g@& iz'kklfud vf/kdkjh layXud% ;Fkksifj Page 1 of 97 ANNEXURE -1 LIST OF SHORTLISTED CANDI DATES FOR TRADE TEST, POST CODE : CHML/TO/20 ADVT. -

Valley Sign in Becker Muscular Dystrophy and Outliers of Duchenne and Becker Muscular Dystrophy
Original Article Valley sign in Becker muscular dystrophy and outliers of Duchenne and Becker muscular dystrophy Sunil Pradhan Department of Neurology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India. Valley sign has been described in patients with Duchenne volvement is an important characteristic of muscular 1 muscular dystrophy (DMD). As there are genetic and clini- dystrophies. In DMD and BMD, this selectivity is evident 2 cal similarities between DMD and Becker muscular dystro- for hypertrophy as well as wasting. In one study done on phy (BMD), this clinical sign is evaluated in this study in DMD patients, infraspinatus and deltoid muscles were found BMD and DMD/ BMD outliers. To evaluate the sign, 28 pa- to be the second and third most common hypertrophied mus- tients with Becker muscular dystrophy (BMD), 8 DMD/BMD cles after the most obvious calf muscles. On observing the outliers and 44 age-matched male controls with other neu- wasting, the muscles forming the anterior and posterior axil- romuscular diseases were studied. The sign was examined lary folds were found to be the ones most significantly wasted.3 after asking patients to abduct their arms to about 90ºwith Still finer observations revealed that in the deltoid muscle, hands directed upwards; the muscle bulk over the back of only the central fibers originating from the acromion process the shoulders was observed. The sign was considered posi- were enlarged while the anterior and posterior fibers originat- tive if the infraspinatus and deltoid muscles were enlarged ing from the clavicle and spinous process of the scapula re- and between these two muscles, the muscles forming the spectively, were wasted.3 Similarly, the inferomedial part of posterior axillary fold were wasted as if there were a valley the infraspinatus muscle was enlarged while the superolateral between the two mounts. -
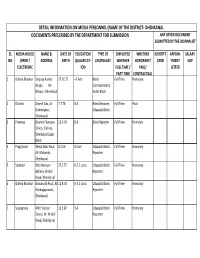
Journalists List Final
DETAIL INFORMATION ON MEDIA PERSONNEL (NAME OF THE DISTRICT- DHENKANAL) DOCUMENTS PRESCRIBED BY THE DEPARTMENT FOR SUBMISSION ANY OTHER DOCUMENT SUBMITTED BY THE JOURNALIST SL. MEDIA HOUSE NAME & DATE OF EDUCATION TYPE OF EMPLOYED WHETHER IDENTITY APPOIN- SALARY NO. (PRINT/ ADDRESS BIRTH QUALIFICAT- JOURNALIST WHETHER HONORARY/ CARD TMENT SLIP ELECTRONIC ION FULL TIME / PAID/ LETTER PART TIME CONTRACTUAL 1 Odisha Bhaskar Sanjaya Kumar 27.01.72 +3 Arts Block Full Time Honorary Nayak, At- Correspondent, Bhapur, Dhenkanal Sadar Block 2 Dharitri Dinesh Das, At- 7.7.76 B.A. Block Reporter, Full Time Paid Gobindapur, Odapada Block Dhenkanal 3 Prameya Biranchi Narayan 13.9.70 B.A. Block Reporter Full Time Honorary Sahoo, Siminai, Dhenkanal Sadar Block 4 Pragativadi Shesa Deva Rout, 8.2.56 B.Com Odapada Block Full Time Honorary At- Motanda, Reporter Dhenkanal 5 Sambad Rabi Narayan 27.2.57 H.S.C. pass Odapada Block Full Time Honorary Behera, Hindol Reporter Road, Dhenkanal 6 Odisha Bhaskar Biswanath Rout, At- 12.8.78 H.S.C. pass Odapada Block Full Time Honorary Khadagaprasad, Reporter Dhenkanal 7 Suryaprava Mihir Kumar 10.5.87 B.A. Odapada Block Full Time Honorary Sahoo, At- Hindol Reporter Road, Dhenkanal 8 Samaya Pratap Kumar 15.3.75 B.Sc Odapada Block Full Time Honorary Behera, At- Hindol Reporter Road, Dhenkanal 9 Samaya Akhila Kumar 19.4.60 B.A. Odapada Block Full Time Honorary MOhapatra, At- Reporter Kamalong, Dist- Dhenkanal 10 Odisha Bhaskar Jatti Nayak, At- 20.7.79 B.A. Reporter Full Time Honorary Haldibahal, Dhenkanal 11 Sambad Ananda Chandra 12.4.68 M.A. -

Alphabetical List of Recommendations Received for Padma Awards - 2014
Alphabetical List of recommendations received for Padma Awards - 2014 Sl. No. Name Recommending Authority 1. Shri Manoj Tibrewal Aakash Shri Sriprakash Jaiswal, Minister of Coal, Govt. of India. 2. Dr. (Smt.) Durga Pathak Aarti 1.Dr. Raman Singh, Chief Minister, Govt. of Chhattisgarh. 2.Shri Madhusudan Yadav, MP, Lok Sabha. 3.Shri Motilal Vora, MP, Rajya Sabha. 4.Shri Nand Kumar Saay, MP, Rajya Sabha. 5.Shri Nirmal Kumar Richhariya, Raipur, Chhattisgarh. 6.Shri N.K. Richarya, Chhattisgarh. 3. Dr. Naheed Abidi Dr. Karan Singh, MP, Rajya Sabha & Padma Vibhushan awardee. 4. Dr. Thomas Abraham Shri Inder Singh, Chairman, Global Organization of People Indian Origin, USA. 5. Dr. Yash Pal Abrol Prof. M.S. Swaminathan, Padma Vibhushan awardee. 6. Shri S.K. Acharigi Self 7. Dr. Subrat Kumar Acharya Padma Award Committee. 8. Shri Achintya Kumar Acharya Self 9. Dr. Hariram Acharya Government of Rajasthan. 10. Guru Shashadhar Acharya Ministry of Culture, Govt. of India. 11. Shri Somnath Adhikary Self 12. Dr. Sunkara Venkata Adinarayana Rao Shri Ganta Srinivasa Rao, Minister for Infrastructure & Investments, Ports, Airporst & Natural Gas, Govt. of Andhra Pradesh. 13. Prof. S.H. Advani Dr. S.K. Rana, Consultant Cardiologist & Physician, Kolkata. 14. Shri Vikas Agarwal Self 15. Prof. Amar Agarwal Shri M. Anandan, MP, Lok Sabha. 16. Shri Apoorv Agarwal 1.Shri Praveen Singh Aron, MP, Lok Sabha. 2.Dr. Arun Kumar Saxena, MLA, Uttar Pradesh. 17. Shri Uttam Prakash Agarwal Dr. Deepak K. Tempe, Dean, Maulana Azad Medical College. 18. Dr. Shekhar Agarwal 1.Dr. Ashok Kumar Walia, Minister of Health & Family Welfare, Higher Education & TTE, Skill Mission/Labour, Irrigation & Floods Control, Govt. -

Allahabad Dealers Of
Dealers of Allahabad Sl.No TIN NO. UPTTNO FIRM - NAME FIRM-ADDRESS 1 09112700012 AD0028383 ALLAHABAD SAINT PAL SOCIETY 28 CHAITHAM LINES ALLAHABAD 2 09112700026 AD0069203 RANG MAHAL 478 KATRA ALLAHABAD 3 09112700031 AD0070803 R.K.ELECTRONICES 32 MONARCO ALLAHABAD 4 09112700045 AD0076384 AMAR MUDRALAY 742 OLD KATRA ALLAHABAD 5 09112700050 AD0077576 UNIVERSAL FOOTWEAR COLONELGANJ ALLAHABAD 6 09112700059 AD0082441 MARWARI STORE 479 KATRA ALLAHABAD 7 09112700064 AD0089747 U.P.STATE BRIDGE CORP.LTD. 26,KASTURBA GANDHI MARG ALLAHABAD 8 09112700078 AD0093128 HIMANCHAL PRAKASHAN 42 BALRAMPUR HOUSE ALLAHABAD 9 09112700083 AD0096956 MILESTONE TYRES P.LTD. 8/63 MASTER ZAHRUL HASAN ROAD KATRA 10 09112700097 AD0102697 UMRAI DEVI A-40 ALNELGANJ ALLAHABAD 11 09112700106 AD0089177 KRISHNA CYCLE HOUSE 349 KATRA ALLAHABAD 12 09112700111 AD0110277 VINAY KUMAR VIJAY KUMAR MAUAIMA SORAON ALLAHABAD 13 09112700125 AD0117875 PRAKASH STORES 607 COLONELGANJ ALLAHABAD 14 09112700130 AD0118032 KRIPA SHANKER GAYATRI PRASAD LAL GOPALGANJ SORAON ALLAHABAD 15 09112700139 AD0126546 SINGH COAL TRADERS 170/3/4 COLONELGANJ ALLAHABAD 16 09112700144 AD0012926 SAHU CYCLE CO. PHAPHAMAU ALLAHANAD 17 09112700163 AD0134430 YADAU BRICK FIELD SORAV PHAPHAMAU ALLAHABAD 18 09112700177 AD0136875 MAUAIMA MACHINERY STORE MAUAIMA SORAON ALLAHABAD 19 09112700182 AD0130279 SHARDA GENERAL STORE SORAV PHAPHAMAU ALLAHABAD 20 09112700196 AD0145142 AJAY COLD STORAGE & ICE FACTORY 363\2 GADDHOPUR ALLAHABAD 21 09112700205 AD0144480 SATEESH KUMAR 263 KATRA ALLAHABAD 22 09112700210 AD0145595 SILVER VING ENTERPRISES 16 B.K. BANARJEE MARG ALLAHABAD 23 09112700219 AD0147563 FAROOQ ENTERPRISES SHIVGARH SORAON ALLAHABAD 24 09112700224 AD0162643 MANEESH ENTERPRISES 141-B/1 CHADPUR SALORI ALLAHABAD 25 09112700238 AD0165888 RAMA SHOE CO. 218 KATRA ALLAHABAD 26 09112700243 AD0171185 CHHEDI LAL 84-C RASOOLABAD ALLAHABAD 27 09112700257 AD0164418 CHANDRA ENTERPRISES 6 M.I.G. -

Padma Awards - One of the Highest Civilian Awards of the Country, Are Conferred in Three Categories, Namely, Padma Vibhushan, Padma Bhushan and Padma Shri
Padma Awards - one of the highest civilian Awards of the country, are conferred in three categories, namely, Padma Vibhushan, Padma Bhushan and Padma Shri. The Awards are given in various disciplines/ fields of activities, viz.- art, social work, public affairs, science and engineering, trade and industry, medicine, literature and education, sports, civil service, etc. ‘Padma Vibhushan’ is awarded for exceptional and distinguished service; ‘Padma Bhushan’ for distinguished service of high order and ‘Padma Shri’ for distinguished service in any field. The awards are announced on the occasion of Republic Day every year. 2. These awards are conferred by the President of India at ceremonial functions which are held at Rashtrapati Bhawan usually around March/ April every year. This year the President of India has approved conferment of 127 Padma Awards including one duo case (counted as one) as per the list below. The list comprises of 2 Padma Vibhushan, 24 Padma Bhushan and 101 Padma Shri Awardees. 27 of the Awardees are women and the list also includes 10 persons from the category of foreigners, NRIs, PIOs and Posthumous Awardees. Padma Vibhushan Sl No. Name Discipline State/ Domicile 1. Dr. Raghunath A. Mashelkar Science and Engineering Maharashtra 2. Shri B.K.S. Iyengar Others-Yoga Maharashtra Padma Bhushan Sl No. Name Discipline State/ Domicile 1. Prof. Gulam Mohammed Sheikh Art - Painting Gujarat 2. Begum Parveen Sultana Art - Classical Singing Maharashtra 3. Shri T.H. Vinayakram Art - Ghatam Artist Tamil Nadu 4. Shri Kamala Haasan Art-Cinema Tamil Nadu 5. Justice Dalveer Bhandari Public Affairs Delhi 6. Prof. Padmanabhan Balaram Science and Engineering Karnataka 7. -

Page 1 of 30
NATIONAL LOK ADALAT CAUSELIST For Saturday The 10th July 2021 COURT NO. 13 (THROUGH VC) SINGLE BENCH (BENCH ID-24812) (BENCH NO. 01) AT 11:00 AM HON'BLE MR.JUSTICE SUJIT NARAYAN PRASAD Lok Adalat 1 Cont.(Cvl)/688/2017 SARDAR DALJEET SINGH NIRAJ KISHORE NEELAM TIWARY VS AKSHAY KR MAHATO MD. SHAMIM AKHTAR THE STATE OF JHARKHAND AND ANR AJIT KUMAR RAHUL KR GUPTA CONTEMPT OF COURTS ACT 1971 2 Cont.(Cvl)/691/2018 MD MAHMUD HASAN MD. JALISUR RAHMAN HIMANSHU KR MEHTA VS VANDANA SINGH THE STATE OF JHARKHAND RICHA SANCHITA CONTEMPT OF COURTS ACT 1971 3 Cont.(Cvl)/701/2018 COURT ON ITS OWN MOTION VS SRI SHASHIDHAR MANDAL MANAGING DIRECTOR MINERAL AREA DEVELOPMENT AUTHORITY CONTEMPT OF COURTS ACT 1971 4 Cont.(Cvl)/702/2018 COURT ON ITS OWN MOTION VS SRI SHASHIDHAR MANDAL MANAGING DIRECTOR MINERAL AREA DEVELOPMENT AUTHORITY CONTEMPT OF COURTS ACT 1971 5 Cont.(Cvl)/703/2018 COURT ON ITS OWN MOTION VS SRI SHASHIDHAR MANDAL MANAGING DIRECTOR MINERAL AREA DEVELOPMENT AUTHORITY CONTEMPT OF COURTS ACT 1971 6 Cont.(Cvl)/704/2018 COURT ON ITS OWN MOTION VS SRI SHREEDHAR MANDAL MANAGING DIRECTOR MINERAL AREA DEVELOPMENT AUTHORITY CONTEMPT OF COURTS ACT 1971 7 Cont.(Cvl)/705/2018 COURT ON ITS OWN MOTION VS SRI SHASHIDHAR MANDAL MANAGING DIRECTOR MINERAL AREA DEVELOPMENT AUTHORITY CONTEMPT OF COURTS ACT 1971 8 Cont.(Cvl)/706/2018 COURT ON ITS OWN MOTION VS MR SHREEDHAR MANDAL MANAGING DIRECTOR MINERAL AREA DEVELOPMENT AUTHORITY CONTEMPT OF COURTS ACT 1971 9 Cont.(Cvl)/707/2018 COURT ON ITS OWN MOTION VS MR SHREEDHAR MANDAL MANAGING DIRECTOR MINERAL AREA DEVELOPMENT AUTHORITY CONTEMPT OF COURTS ACT 1971 10 Cont.(Cvl)/708/2018 COURT ON ITS OWN MOTION VS SRI SHASHIDHAR MANDAL MANAGING DIRECTOR MINERAL AREA DEVELOPMENT AUTHORITY CONTEMPT OF COURTS ACT 1971 Page 1 of 30. -

Sakthy Academy Coimbatore
Sakthy Academy Coimbatore Bharat Ratna Award: List of recipients Year Laureates Brief Description 1954 C. Rajagopalachari An Indian independence activist, statesman, and lawyer, Rajagopalachari was the only Indian and last Governor-General of independent India. He was Chief Minister of Madras Presidency (1937–39) and Madras State (1952–54); and founder of Indian political party Swatantra Party. Sarvepalli He served as India's first Vice- Radhakrishnan President (1952–62) and second President (1962–67). Since 1962, his birthday on 5 September is observed as "Teachers' Day" in India. C. V. Raman Widely known for his work on the scattering of light and the discovery of the effect, better known as "Raman scattering", Raman mainly worked in the field of atomic physics and electromagnetism and was presented Nobel Prize in Physics in 1930. 1955 Bhagwan Das Independence activist, philosopher, and educationist, and co-founder of Mahatma Gandhi Kashi Vidyapithand worked with Madan Mohan Malaviya for the foundation of Banaras Hindu University. M. Visvesvaraya Civil engineer, statesman, and Diwan of Mysore (1912–18), was a Knight Commander of the Order of the Indian Empire. His birthday, 15 September, is observed as "Engineer's Day" in India. Jawaharlal Nehru Independence activist and author, Nehru is the first and the longest-serving Prime Minister of India (1947–64). 1957 Govind Ballabh Pant Independence activist Pant was premier of United Provinces (1937–39, 1946–50) and first Chief Minister of Uttar Pradesh (1950– 54). He served as Union Home Minister from 1955–61. 1958 Dhondo Keshav Karve Social reformer and educator, Karve is widely known for his works related to woman education and remarriage of Hindu widows.