Evaluation of Work Efficiency and Medical Quality for a Hospital on the PPP Model in China with Benchmarking and GRA
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Distributed Scatterer Insar Reveals Surface Motion of the Ancient Chaoshan Residence Cluster in the Lianjiang Plain, China
Article Distributed Scatterer InSAR Reveals Surface Motion of the Ancient Chaoshan Residence Cluster in the Lianjiang Plain, China Yuzhou Liu 1, Peifeng Ma 1,2,3,*, Hui Lin 1,4,5, Weixi Wang 2,6 and Guoqiang Shi 1 1 Institute of Space and Earth Information Science, The Chinese University of Hong Kong, Shatin, N.T., Hong Kong; [email protected](Y.L.); [email protected] (H.L.); [email protected] (G.S.) 2 Key Laboratory of Urban Land Resources Monitoring and Simulation, Ministry of Land and Resources, Shenzhen 518034, China; [email protected] 3 Faculty of Geosciences and Environmental Engineering, Southwest Jiaotong University, Chengdu 611756, China 4 Shenzhen Research Institute, The Chinese University of Hong Kong, Shenzhen 518063, China 5 Department of Geography and Resource Management, The Chinese University of Hong Kong, Shatin, N.T., Hong Kong 6 Research Institute for Smart Cities, School of Architecture and Urban Planning, Shenzhen University, Shenzhen 518060, China * Correspondence: [email protected]; Tel.: +852-3943-4407 Received: 14 December 2018; Accepted: 15 January 2019; Published: 16 January 2019 Abstract: The Lianjiang Plain in China and ancient villages distributed within the plain are under the potential threat of surface motion change, but no effective monitoring strategy currently exists. Distributed Scatterer InSAR (DSInSAR) provides a new high-resolution method for the precise detection of surface motion change. In contrast to the first-generation of time-series InSAR methodology, the distributed scatterer-based method focuses both on pointwise targets with high phase stability and distributed targets with moderate coherence, the latter of which is more suitable for the comprehensive environment of the Lianjiang Plain. -

Cotton on Group Supplier List 2018 Cotton on Group - Supplier List 2
Cotton On Group supplier list 2018 Cotton On Group - Supplier List _2 TOTAL % OF FEMALE % OF MIGRANT/ PARENT COUNTRY FACTORY NAME SUPPLIER ADDRESS STAGE WORKERS WORKERS TEMP COMPANY (IF APPLICABLE) UNIT 4/22 NARABANG WAY AUSTRALIA AXIS TOYS BELROSE CMT 3 67 0 NSW 2085 10 CHALDER STREET AUSTRALIA BODYTREATS AUSTRALIA MARRICKVILLE CMT 3 3 0 NSW 2204 32 CHESTERFIELD AVE BONDI CONSTELLATION PTY LTD MALVERN AUSTRALIA T/A ZEBRA HOMEWARES AND CMT 4 67 0 MELBOURNE SMILING ZEBRA SUITE 6, 60 LANGRIDGE ST AUSTRALIA I SCREAM NAILS COLLINGWOOD CMT VIC 3066 42 BARKLY ST INNOVATIVE BEVERAGE CO PTY AUSTRALIA ST KILDA CMT 7 29 0 LTD VIC 3182 UNIT 1, 57-59 BURCHILL STREET AUSTRALIA LIFESTYLE JEWELLERY PTY LTD LOGANHOLME CMT 20 56 0 QLD 4129 90 MARIBYRNONG CT AUSTRALIA LONELY PLANET FOOTSCRAY CMT VIC 3011 88 KYABRAM ST AUSTRALIA MERCATOR PTY LTD COOLAROO CMT VIC 3048 3/1490 FERNTREE GULLY ROAD AUSTRALIA WARRANBROOKE PTY LTD KNOXFIELD CMT VIC 3180 HARI BARITEK BANGLADESH A&A TROUSERS PUBAIL COLLEGE GATE CMT 1973 61 0 N/A GAZIPUR SINGAIR ROAD, DEKKO ACCESSORIES BANGLADESH AGAMI ACCESSORIES LTD HEMAYETPUR, RAW MATERIALS 324 25 0 LIMITED SAVAR, DHAKA GOLORA, CHORKHONDO, BANGLADESH AKIJ TEXTILE MILLS LTD MANIKGANJ SADAR, FABRIC/MILLS 1904 18 0 AKIJ GROUP MANIKGANJ Supplier List as at June 2018 Cotton On Group - Supplier List _3 BOIRAGIRCHALA BANGLADESH AMANTEX UNIT 2 LTD SREEPUR, INPUTS 74 0 0 N/A GAZIPUR 468-69, BSCIC I/A, SHASHONGAON BANGLADESH AMS KNITWEAR LTD ENAYETNAGAR, FATULLAH CMT 212 83 0 N/A NARAYANGONJ-1400 SATISH ROAD BANGLADESH ANAM CLOTHING LTD -

Table of Codes for Each Court of Each Level
Table of Codes for Each Court of Each Level Corresponding Type Chinese Court Region Court Name Administrative Name Code Code Area Supreme People’s Court 最高人民法院 最高法 Higher People's Court of 北京市高级人民 Beijing 京 110000 1 Beijing Municipality 法院 Municipality No. 1 Intermediate People's 北京市第一中级 京 01 2 Court of Beijing Municipality 人民法院 Shijingshan Shijingshan District People’s 北京市石景山区 京 0107 110107 District of Beijing 1 Court of Beijing Municipality 人民法院 Municipality Haidian District of Haidian District People’s 北京市海淀区人 京 0108 110108 Beijing 1 Court of Beijing Municipality 民法院 Municipality Mentougou Mentougou District People’s 北京市门头沟区 京 0109 110109 District of Beijing 1 Court of Beijing Municipality 人民法院 Municipality Changping Changping District People’s 北京市昌平区人 京 0114 110114 District of Beijing 1 Court of Beijing Municipality 民法院 Municipality Yanqing County People’s 延庆县人民法院 京 0229 110229 Yanqing County 1 Court No. 2 Intermediate People's 北京市第二中级 京 02 2 Court of Beijing Municipality 人民法院 Dongcheng Dongcheng District People’s 北京市东城区人 京 0101 110101 District of Beijing 1 Court of Beijing Municipality 民法院 Municipality Xicheng District Xicheng District People’s 北京市西城区人 京 0102 110102 of Beijing 1 Court of Beijing Municipality 民法院 Municipality Fengtai District of Fengtai District People’s 北京市丰台区人 京 0106 110106 Beijing 1 Court of Beijing Municipality 民法院 Municipality 1 Fangshan District Fangshan District People’s 北京市房山区人 京 0111 110111 of Beijing 1 Court of Beijing Municipality 民法院 Municipality Daxing District of Daxing District People’s 北京市大兴区人 京 0115 -

Next Tier 3 Suppliers 2020
TIER 3 SUPPLIER SITES - Produced March 2021 SUPPLIER NAME ADDRESS SPINNING KNITTING WEAVING DYEING PRINTING Bangladesh A One Polar Ltd Vulta, Rupgonj, Nrayangonj ✓ ✓ ✓ AA Spinning Mill Ltd Nagar Howla, Sreepur, Gazipur District, Dhaka ✓ Aaron Denim Ltd Sukran, Mirzanagar, Nobinagar, Savar, Dhaka 1347 ✓ ✓ Abanti Colour Tex Ltd S A-646, Shashongaon, Enayetnagar, Fatullah, Narayanganj 1400 ✓ ✓ ✓ ACS Textiles Ltd Tetlabo, Rupgonj, Ward 3, Narayangonj, Dhaka 1400 ✓ ✓ ✓ Adury Knit Composite Ltd Karadi, Shibpur, Narsingdi Narshingdi Dhaka ✓ ✓ ✓ Akij Textile Mills Ltd Golora, Charkhanda, Manikgonj ✓ ✓ ✓ Al Haj Karim Textiles Ltd Kalampur, Dhamrai, Savar, Dhaka 1351 ✓ Alim Knit BD Ltd Nayapara, Kashimpur, Zitar Moor, Gazipur ✓ ✓ ✓ Alliance Knit Composite Ltd 8/118, Pukurpar, Zirabo, Ashulia, Savar, Dhaka-1341 ✓ ✓ ✓ Aman Spinning Mills Ltd Ashulia Highway, Zirabo, Ashulia, Savar, Dhaka ✓ Amantex Limited Boiragi Challa, Shreepur, Gazipur 1740, Dhaka ✓ ✓ ✓ Amber Cotton Mills Ltd Banglabazar, Bahadurpur, Razendrapur, Gazipur, Dhaka ✓ Amber Denim Mills Ltd (Unit 2) Unit 2, Banglabazar, Bahadurpur, Razendrapur, Gazipur, Dhaka ✓ ✓ Anjum Textile Mills Birampur, Madhobdi, Norshingd ✓ ✓ Anwar Silk Mills Ltd 186 Tongi Industrial Area, Tongi, Gazipur ✓ Apex Weaving and Finishing Mills Ltd East Chundora, Shafipur, Kaliakoar, Gazipur 1751 ✓ ✓ ✓ APS Group Kamar Gaon Pubail Road Gazipur ✓ ✓ Argon Denims Ltd Beraider Chala Po Gilaberaid Ps Sripur, Gazipur, 1742, Gazipur ✓ ✓ ✓ Arif Spinning Mill Ltd Mastarbari, Jamirdia, Valuka, Mymensingh ✓ Armada Spinning Mills -

Annual Report 2020 002 Prospect
ABOUT US Charmacy Pharmaceutical Co., Ltd. (stock code: 2289.HK) is principally engaged in the pharmaceutical distribution business. It mainly distributes western medicine, Chinese patent medicine and healthcare products to downstream distributors and retail terminals, as well as provides consultation service on pharmaceutical products. Founded in 2000, over the past 21 years of rapid development, it has become one of the leading pharmaceutical distributors in the Southern China region. The Company adheres to the development strategy of "Intensive Engagement in Guangdong Province and Extensive Coverage across Surrounding Areas", and has built logistics centers in Shantou, Foshan, Zhuhai, Guangzhou and Huizhou, all equipped with professional transportation teams, and has a highly efficient delivery mechanism of delivering pharmaceutical products three times per day for customers within a radius of 10 kilometers, twice per day for customers within a radius of 50 kilometers and once per day for those within a 250-kilometers' radius. In addition, the Company has a modern information system that covers the entire supply chain for pharmaceutical distribution, including procurement, sales, warehousing, transportation and delivery. Apart from that, the Company operates its own B2B e-commerce platform "Charmacy e-Medicine" ( 創美e 藥 ), a platform for customers to place orders online, make inquires and payment and many more. In 2019, the Company ranked top 50 among top 100 PRC wholesalers, in respect of revenue generated from the principal business. According to the Market Research Report of the Chinese Pharmaceutical Industry (2017) (《中國醫藥行業市場研究報告》(2017)), in respect of sales scale, the Company ranked 7th among the pharmaceutical distribution businesses in Guangdong Province and second among private enterprises. -
3114-PRC: Guangdong Chaonan Water Resources Development and and Title: Protection Demonstration Project Contract No
Invitation for Bids Date: 4 July 2017 Loan No. 3114-PRC: Guangdong Chaonan Water Resources Development and and Title: Protection Demonstration Project Contract No. C8: Civil works, installation, and commissioning of the Jinxi and Qiufeng and Title: water supply plants Deadline for Submission of 4 August 2017; 10:00 hours (Beijing Time) Bids: 1. The People’s Republic of China has received a loan from the Asian Development Bank (ADB) towards the cost of Guangdong Chaonan Water Resources Development and Protection Demonstration Project and it intends to apply part of the proceeds of this loan to payments under the Contract named above. Bidding is open to Bidders from eligible source countries of the ADB. 2. The Chaonan Water Supply Company (“the Employer”) invites sealed bids from all eligible Bidders for the civil works, installation, and commissioning of the Jinxi and Qiufeng water supply plants (WSP) (C8). The construction site of Qiufeng WSP Expansion and Jinxi WSP Upgrade Project is respectively located in Gucuo Village of Liangying Town and Shenxi Village of Xiancheng Town, whose water sources are respectively Qiufeng water system and Jinxi water system. The main construction content includes but is not limited to: water treatment buildings and structures with capacity of 72000m3/d, water intake pumping room within reservoir, water distribution pumping room in plant area, sludge treatment facilities, chlorine and chemical dosing room, raw water pipes and outlet pipes, access roads to WSP, counterpart facilities of plant area with capacity of 142000m3/d. The construction period of the above project is 18 months after contract signing. 3. -
Primark Does Not Own Any Factories and Is Selective About the Suppliers with Whom We Work
Information last updated November 2020 Global Sourcing Map Factory List - Bangladesh Factory Name Address Country Total Men Women Number of Workers A&A Trousers Ltd Haribaritek Pubail College Gate Gazipur Dhaka 1721 Bangladesh 2250 996 (44.3)% 1254 (55.7)% Afiya Knitwear Ltd 10/ 2 Durgapur Ashulia Savar Dhaka 1341 Bangladesh 496 232 (46.8)% 264 (53.2)% AKH Apparels Ltd 128 Hemayetpur Savar Dhaka 1340 Bangladesh 2136 855 (40.0)% 1281 (60.0)% Alpha Clothing Ltd Tenguri, BKSP Ashulia Savar Dhaka Bangladesh 1971 968 (49.1)% 1003 (50.9)% Ananta Huaxiang Ltd 222, 223, H2-H4, Adamjee EPZ Shiddirgonj Narayanganj Dhaka Bangladesh 2038 982 (48.2)% 1056 (51.8)% Anowara Knit Composite Ltd Mulaid Mawna Sreepur Gazipur Bangladesh 2276 1329 (58.4)% 947 (41.6)% Aspire Garments Ltd 491 Dhalla Singair Manikganj 1822 Bangladesh 2992 1389 (46.4)% 1603 (53.6)% ASR Sweater Limited Mulaied Maona Sreepur Gazipur Bangladesh 1458 927 (63.6)% 531 (36.4)% Primark does not own any factories and is selective about the suppliers with whom we work. Every factory which manufactures product for Primark has to commit to meeting internationally recognised standards, before the first order is placed and throughout the time they work with us. The factories featured on Primark’s Global Sourcing Map are Primark’s suppliers’ production sites which represent over 95% of Primark products for sale in Primark stores. A factory is detailed on the Map only after it has produced products for Primark for a year and has become an established supplier. During the first year a factory has to demonstrate that it can consistently work to Primark’s ethical standards, as well as meet our commercial requirements in areas such as quality and timely delivery. -

Official-Gazette-Vol.-89.Pdf
ສາທາລະນະລດັ ປະຊາທິປະໄຕ ປະຊາຊນົ ລາວ LAO PEOPLE’S DEMOCRATIC REPUBLIC ກະຊວງ ວທິ ະຍາສາດ ແລະ ເຕັກໂນໂລຊ ີ ກມົ ຊບັ ສນິ ທາງປນັ ຍາ MINISTRY OF SCIENCE AND TECHNOLOGY DEPARTMENT OF INTELLECTUAL PROPERTY ຈດົ ໝາຍເຫດທາງລດັ ຖະການ ກຽ່ ວກບັ ການເຜີຍແຜຜ່ ນົ ຂອງການຈດົ ທະບຽນ ຊບັ ສນິ ອດຸ ສາຫະກາ ຢ່ ສປປ ລາວ OFFICIAL GAZETTE OF INDUSTRIAL PROPERTY ສະບບັ ທີ (Vol.) 89 Official Gazette of Industrial Property Vol. 89, 20/03/2020 ສາລະບານ ພາກທີ I: ຜນົ ຂອງການຂໍຈດົ ທະບຽນເຄື່ ອ ງໝາຍການຄາ້ ພາກທີ II: ຜນົ ຂອງການຈດົ ທະບຽນເຄື່ ອ ງໝາຍການຄາ້ ພາກທີ III: ຜນົ ຂອງການຂໍຈດົ ທະບຽນເຄື່ ອ ງໝາຍການຄາ້ ສາກນົ ພາກທີ IV: ຜນົ ຂອງການຈດົ ທະບຽນເຄື່ ອ ງໝາຍການຄາ້ ສາກນົ ພາກທີ V: ຜນົ ຂອງການຕື່ ອາຍກຸ ານຈດົ ທະບຽນເຄື່ ອ ງໝາຍການຄາ້ CONTENT Part I: New Application of Trademark Part II: Registration of Trademark Part III: Madrid New Application of Trademark Part IV: Madrid Registration of Trademark Part V: Renewal of Trademark I Official Gazette of Industrial Property Vol. 89, 20/03/2020 ພາກທີ I ຜນົ ຂອງການຂໍຈດົ ທະບຽນເຄື່ ອ ງໝາຍການຄາ້ ຄາ ແນະນາ ກຽື່ ວກບັ ລະຫດັ ຫຍ ້ (540) ເຄື່ ອ ງໝາຍການຄາ້ (511) ໝວດຂອງສນິ ຄາ້ ແລະ ການບ ລິການ (210) ເລກທີຄາ ຮອ້ ງ (220) ວນັ ທີທື່ ີຍື່ ນ ຄາ ຮອ້ ງ (732) ຊື່ ແລະ ທື່ ີຢື່ ຂອງຜຍ້ ື່ ນຄາ ຮອ້ ງ Part I New Application of Trademark Introduction of Codes (540) Trademark (511) Classification of goods and services (Nice Classification) (210) Number of the application (220) Date of filing of the application (732) Name and Address of applicant II Official Gazette of Industrial Property Vol. 89, 20/03/2020 ພາກທີ II ຜນົ ຂອງການຈດົ ທະບຽນເຄື່ ອ ງໝາຍການຄາ້ ຄາ ແນະນາ ກຽື່ ວກບັ ລະຫດັ ຫຍ ້ (540) ເຄື່ -

Global Factory List As of August 3Rd, 2020
Global Factory List as of August 3rd, 2020 Target is committed to providing increased supply chain transparency. To meet this objective, Target publishes a list of all tier one factories that produce our owned-brand products, national brand products where Target is the importer of record, as well as tier two apparel textile mills and wet processing facilities. Target partners with its vendors and suppliers to maintain an accurate factory list. The list below represents factories as of August 3rd, 2020. This list is subject to change and updates will be provided on a quarterly basis. Factory Name State/Province City Address AMERICAN SAMOA American Samoa Plant Pago Pago 368 Route 1,Tutuila Island ARGENTINA Angel Estrada Cla. S.A, Buenos Aires Ciudad de Buenos Aires Ruta Nacional N 38 Km. 1,155,Provincia de La Rioja AUSTRIA Tiroler Glashuette GmbH Werk: Schneegattern Oberosterreich Lengau Kobernauserwaldstrase 25, BAHRAIN WestPoint Home Bahrain W.L.L. Al Manamah (Al Asimah) Riffa Building #1912, Road # 5146, Block 951,South Alba Industrial Area, Askar BANGLADESH Campex (BD) Limited Chittagong zila Chattogram Building-FS SFB#06, Sector#01, Road#02, Chittagong Export Processing Zone,, Canvas Garments (Pvt.) Ltd Chittagong zila Chattogram 301, North Baizid Bostami Road,,Nasirabad I/A, Canvas Building Chittagong Asian Apparels Chittagong zila Chattogram 132 Nasirabad Indstrial Area,Chattogram Clifton Cotton Mills Ltd Chittagong zila Chattogram CDA plot no-D28,28-d/2 Char Ragmatia Kalurghat, Clifton Textile Chittagong zila Chattogram 180 Nasirabad Industrial Area,Baizid Bostami Road Fashion Watch Limited Chittagong zila Chattogram 1363/A 1364 Askarabad, D.T. Road,Doublemoring, Chattogram, Bangladesh Fortune Apparels Ltd Chittagong zila Chattogram 135/142 Nasirabad Industrial Area,Chattogram KDS Garment Industries Ltd. -

ACCASETTE GARMENT CO LTD Cambodia National Road No 3, Phnom Penh City Apparel 1000-3000 CO
Strategic Contractors Parent HBI Factory Name Country Address Product Type Employees HAND SEVEN INTERNATIONAL ENT. ACCASETTE GARMENT CO LTD Cambodia National Road No 3, Phnom Penh City Apparel 1000-3000 CO. LTD. | HAND SEVEN INTERNATIONAL ENT. ACCASETTE GARMENT VIETNAM CO LTD Vietnam One Part CN18 N2 Street & 6 Street Song Than 3 Industrial Zone, Phu Tan Ward, Thu Apparel 1000-3000 CO. LTD. | Dau Mot City Best Corporation Private Limited | ALPHA APPARELS India 106/1 Avinashi Road Lpt Opp Arasurpo, Coimbatore Apparel <1000 DAIWABO NEU CO. LTD. | ANHUI NEWJIALE GARMENT CO China 318 National Road Wenchang ToWn, Xuancheng City, Anhui Province Apparel <1000 ZXY INTERNATIONAL FZCO | Anlima Textile Limited Bangladesh Karnapara Savar, Dhaka 12090 Bangladesh Apparel 1000-3000 APEX LINGERIE LIMITED APEX LINGERIE LIMITED Bangladesh MOUZA-CHANDURA GAZIPUR, Bangladesh Apparel >3000 APEX TEXTILE PRINTING MILLS APEX TEXTILE PRINTING MILLS LIMITED Bangladesh Biman Bhaban 5th Floor Chandora Kailakoir, Gazipur Apparel >3000 LIMITED SHK CO.LTD. | APPARELTECH VINH LOC GARMENT EXPORT CO Vietnam Vinh Long Commune Vinh Loc District Thanh Hoa Province, Vinh Loc, Thua Thien- Apparel >3000 LTD Hue MARQUIS IMPEX PTE. LTD. |Best BEST INTERNATIONAL GAREMENTS PLC Ethiopia Shed No 38, HaWassa Industrial Park HaWassa SNPPR Region Apparel <1000 Corporation Private Limited | BOGART LINGERIE LTD BOGART LINGERIE SHENZHEN LTD China No28-29 Building No3 Shenzhen, China Apparel 1000-3000 HANSAE CO. LTD. | Branch of Hanoi Textile and Garment Joint Stock CorporationVietnam Nam Giang Inderstrial Zone Nam Dan, 25110 Vietnam Apparel 1000-3000 DAMOST CORP LTD | Chaohu Galaxy Vegas Textile China No 8, Jinchao Avenue, Heifei City, Anhui Apparel <1000 MIDAS GARMENT ENTERPRISE LTD TaiWan NO 36 SHINGUNG FIRST RD TAINJUNG, TaiWan Apparel <1000 (HQ) |MIDAS GARMENT ENTERPRISE LTD. -

Resettlement Plan
Resettlement Plan Project Number: 46079 January 2014 PRC: Guangdong Chaonan Water Resources Development and Protection Demonstration Project Prepared by the Chaonan Water Supply Company under the Chaonan Water Affairs Bureau of the Chaonan District Government, Guangdong Province, People’s Republic of China for the Asian Development Bank. CURRENCY EQUIVALENTS (as of 24 January 2014) Currency unit – yuan (CNY) CNY1.00 = $0.1652 $1.00 = CNY6.0527 ABBREVIATIONS ADB – Asian Development Bank AAOV – average annual output value AH – affected household CNY – Chinese yuan CFB – Chaonan Finance Bureau CLRB – Chaonan Land Resources Bureau CWAB – Chaonan Water Affairs Bureau CWSC – Chaonan Water Supply Company DI – design institute EA – executing agency GDP – gross domestic product FSR – feasibility study report HH – household IA – implementing agency LAR – land acquisition and resettlement LARD – Land Acquisition and Resettlement Division M&E – monitoring and evaluation MLSSP – Minimum Living Standard Security Program PMO – project management office PPTA – project preparatory technical assistance PRC – People’s Republic of China RP – resettlement plan TOR – term of reference NOTES (i) The fiscal year (FY) of the Government of the People’s Republic of China and its agencies ends on 31 December. FY before a calendar year denotes the year in which the fiscal year ends, e.g., FY2010 ends on 31 December 2013. (ii) In this report, "$" refers to US dollars. This resettlement plan is a document of the borrower. The views expressed herein do not necessarily represent those of ADB's Board of Directors, Management, or staff, and may be preliminary in nature. Your attention is directed to the “terms of use” section of this website. -
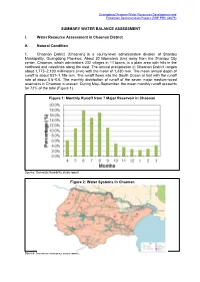
46079-002: Guangdong Chaonan Water Resources Development And
Guangdong Chaonan Water Resources Development and Protection Demonstration Project (RRP PRC 46079) SUMMARY WATER BALANCE ASSESSMENT I. Water Resource Assessment in Chaonan District A. Natural Condition 1. Chaonan District (Chaonan) is a county-level administrative division of Shantou Municipality, Guangdong Province. About 30 kilometers (km) away from the Shantou City center, Chaonan, which administers 232 villages in 11 towns, is a plain area with hills in the northeast and coastlines along the east. The annual precipitation in Chaonan District ranges about 1,773–2,100 millimeters (mm) with the mean of 1,830 mm. The mean annual depth of runoff is about 831–1,186 mm. The runoff flows into the South Ocean at last with the runoff rate of about 0.5–0.6. The monthly distribution of runoff of the seven major medium-sized reservoirs in Chaonan is uneven. During May–September, the mean monthly runoff accounts for 72% of the total (Figure 1). Figure 1: Monthly Runoff from 7 Major Reservoir in Chaonan Source: Domestic feasibility study report. Figure 2: Water Systems in Chaonan Source: Domestic feasibility study report. 2 B. Available Water Resources1 1. Rivers 2. Leiling River. Leiling river originates from Leiling Mountain and has three branch streams joining together at Shuangxi Village in Leiling Town. It runs across Shenquan Port in Huilai County and enters into the South China Sea. The length of Leiling River is 26 km with a catchment area of 444 square kilometers (km2), of which 61 km2 or 13.7% of the total catchment area is in Chaonan. The total average annual flow of the river is 11 million cubic meters (m3).