Mapping Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

(Northern Ireland) 2014
STATUTORY RULES OF NORTHERN IRELAND 2014 No. 36 ROADS The M1/Trunk Road T3 and M1-M2 Link (Amendment) Order (Northern Ireland) 2014 Made - - - - 12th February 2014 Coming into operation - 1st April 2014 The Department for Regional Development(a) in accordance with Article 15(1) of the Roads (Northern Ireland) Order 1993(b) having constructed the lengths of road described in Part I of Schedule 1 considers it expedient to designate them as special roads. The Department in accordance with Article 14(1) of that Order considers it expedient for the purpose of improving the trunk system that the lengths of road described in Parts I and II and the road and lengths of road described in Part III of Schedule 1 should be designated as trunk roads and that the roads and lengths of trunk road described in Part IV of that Schedule should cease to be trunk road. The Department has published and served a notice in compliance with paragraphs 1 and 2 of Schedule 8 to that Order. No objection has been received. The Department, in exercise of the powers conferred by Articles 14(1), 15(1), 16(1) and (2) and 68(6) of the Roads (Northern Ireland) Order 1993 and now vested in it(c) orders and directs as follows: Citation, commencement and interpretation 1.—(1) This Order may be cited as The M1/Trunk Road T3 and M1-M2 Link (Amendment) Order (Northern Ireland) 2014 and shall come into operation on 1st April 2014. (2) In this Order— “map T3/1” to “map T3/11”, means the sequence of drawings numbered from T3/1 to T3/11, marked “The M1/Trunk Road T3 and M1-M2 Link (Amendment) Order (Northern Ireland) 2014” copies of which have been deposited at the Department’s Roads Service offices, Headquarters, Clarence Court, 10-18 Adelaide Street, Belfast BT2 8GB, Northern Division, County Hall, Castlerock Road, Coleraine BT51 3HS, Western Division, County Hall, (a) S.I. -

Register of Employers
REGISTER OF EMPLOYERS A Register of Concerns in which people are employed in accordance with Article 47 of the Fair Employment and Treatment (Northern Ireland) Order 1998 The Equality Commission for Northern Ireland Equality House 7-9 Shaftesbury Square Belfast BT2 7DP Tel: (02890) 500 600 Fax: (02890) 328 970 Textphone: (02890) 500 589 E-mail [email protected] SEPTEMBER 2003 ________________________________________________REGISTRATION The Register Under Article 47 of the Fair Employment and Treatment (Northern Ireland) Order 1998 the Commission has a duty to keep a Register of those concerns employing more than 10 people in Northern Ireland and to make the information contained in the Register available for inspection by members of the public. The Register is available for use by the public in the Commission’s office. Under the legislation, public authorities as specified by the Office of the First Minister and the Deputy First Minister are automatically treated as registered with the Commission. All other employers have a duty to register if they have more than 10 employees working 16 hours or more per week. Employers who meet the conditions for registration are given one month in which to apply for registration. This month begins from the end of the week in which the concern employed more than 10 employees in Northern Ireland. It is a criminal offence for such an employer not to apply for registration within this period. Persons who become employers in relation to a registered concern are also under a legal duty to apply to have their name and address entered on the Register within one month of becoming such an employer. -

Smythe-Wood Series B
Mainly Ulster families – “B” series – Smythe-Wood Newspaper Index Irish Genealogical Research Society Dr P Smythe-Wood’s Irish Newspaper Index Selected families, mainly from Ulster ‘SERIES B’ The late Dr Patrick Smythe-Wood presented a large collection of card indexes to the IGRS Library, reflecting his various interests, - the Irish in Canada, Ulster families, various professions etc. These include abstracts from various Irish Newspapers, including the Belfast Newsletter, which are printed below. Abstracts are included for all papers up to 1864, but excluding any entries in the Belfast Newsletter prior to 1801, as they are fully available online. Dr Smythe-Wood often found entries in several newspapers for the one event, & these will be shown as one entry below. Entries dealing with RIC Officers, Customs & Excise Officers, Coastguards, Prison Officers, & Irish families in Canada will be dealt with in separate files. In most cases, Dr Smythe-Wood has recorded the exact entry, but in some, marked thus *, the entries were adjusted into a database, so should be treated with more caution. There are further large card indexes of Miscellaneous notes on families which are not at present being digitised, but which often deal with the same families treated below. ACR: Acadian Recorder LON The London Magazine ANC: Anglo-Celt LSL Londonderry Sentinel ARG Armagh Guardian LST Londonderry Standard BAA Ballina Advertiser LUR Lurgan Times BAI Ballina Impartial MAC Mayo Constitution BAU Banner of Ulster NAT The Nation BCC Belfast Commercial Chronicle NCT -

Quality Craftsmanship
Quality Craftsmanship Coolestone established by Alan Herron is a highly experienced stone masonry and stone supplier based in Dungannon, County Tyrone. As a leading stone company, Coolestone has an envied reputation as house builders, creating distinctive homes which utilise both the aesthetic and functional qualities of stone to develop homes with real character. With extensive knowledge of the stonemasonry industry Coolestone combines traditional materials with modern design to create stunning masterpieces. Coolestone prides itself on the quality craftsmanship from each of its stone masons offering a full in house service of design, manufacture, supply, delivery and building of stone providing you with the complete package for all your stone requirements. Coolestone is a reputable company with vast experience in its field and knows what is required on site and aims to provide customers with a comprehensive service supplying among other items, guillotined and bagged sandstone, limestone, basalt, granite, quartzite, cills and heads, hand carved arches and quoins. Coolestone also supplies high quality stone sourced locally and to offer the most extensive range around, imports from across the globe, selling into the commercial and domestic markets. Coolestone has a stone centre at the Dungannon site with built panels of stone that will help you to select the stone for your project. Why not go along and view the comprehensive portfolio to help create your dream project. Mix of reclaimed Sandstone, Pink Sandstone & Donegal Sandstone, Limestone window cills & heads Brown Quartzite Liscannor Sandstone dry build Donegal Sandstone with Sandstone window and door surrounds SANDSTONE Sandstone is a sedimentary rock composed of grains of sand compressed together. -

TRPSI Consultation Responses
ID No. Organisation 1 Lisburn and Castlereagh City Council 2 NI Farm Groups 3 Committee for Social Development 4 Disability Action 5 CLOUGH AND DISTRICT COMMUNITY ASSOCIATION 6 South West Age Partnership 7 Community Transport Network NI 8 Commissioner for Older People for Northern Ireland 9 North Antrim Community Network 10 Kilcoo GAC 11 Annsborough Community Forum 12 Killean & Edentubber Regeneration Group 13 TADA Rural support Network 14 CDM Community Transport 15 Hilltown Community Association 16 Annalong Community Association 17 Fivemiletown Community Development Association (COSTA) 18 Parkanaur College (COSTA) 19 Galbally Community Centre (COSTA) 20 Dungannon Area Churches Forum (COSTA) 21 Tamnamore Community Development Association (COSTA) 22 Aughnacloy Development Association (COSTA) 23 Killeeshill & Clonaneese Historical Society (COSTA) 24 Soroptomist International (COSTA) 25 Richmond Parents Support Group (COSTA) 26 Bawn Development Association (COSTA) 27 COSTA 28 ARMAGH RURAL TRANSPORT 29 Libraries NI 30 Drumquin Development Association 31 Robert Hamilton 32 Fermanagh and Omagh District Council 33 County Armagh Community Development 34 Ballywalter Community Action Group 35 Portaferry Regeneration Limited 36 Advantage 37 NILGA 38 Drummond Centre Project Ltd 39 Dennett Interchange 40 Omagh Forum for Rural Associations 41 Aughlisnafin Community Association 42 County Down Rural Community Network 43 Castlerock Community Association 44 Creggan Community Association 45 Butterlope Social Farm CIC 46 Claudy Parish Community Group 47 Gortilea -

Minutes of Cookstown Town Centre Forum Meeting Held on Wednesday 30 August 2017 at 12.30Pm in the Chamber, Mudc Offices, Cookstown
MINUTES OF COOKSTOWN TOWN CENTRE FORUM MEETING HELD ON WEDNESDAY 30 AUGUST 2017 AT 12.30PM IN THE CHAMBER, MUDC OFFICES, COOKSTOWN Present: Councillor J McNamee Mid Ulster District Council Councillor M Glasgow Mid Ulster District Council Councillor C Mallaghan Mid Ulster District Council Councillor T Quinn Mid Ulster District Council Patrick Anderson Department for Communities Neil Bratton Department for Infrastructure Ursula Marshall Cookstown Disability Forum TP Sheehy Small Independent Retailer Raymond McGarvey Cookstown Chamber of Commerce Seamus Doone Police Service of Northern Ireland Fiona McKeown ) Andrew Cassells ) Mid Ulster District Council Mary McCullagh ) In attendance: Colleen Bell ) Mid Ulster District Council The Chairman, Councillor McNamee welcomed all members to the Cookstown Town Centre Forum Meeting. 1) APOLOGIES Apologies were received on behalf of Councillor Wilson, Mid Ulster District Council; Eugene Teague, ASDA; Tom Jebb, Vinters Association; Inspector Danny Walsh, PSNI; Brain McCallion and John Hynes, Tesco; Bernie Sonners, Tenants Association; Jim Eastwood, Cookstown Enterprise Centre; Elaine Mullin, Adrian McCreesh and Colin McKenna, Mid Ulster District Council. 2) MINUTES OF PREVIOUS MEETING It was AGREED to ADOPT the minutes of the Town Centre Forum Meeting held on 3 May 2017. - 1 - 3) MATTERS ARISING FROM MINUTES a) Cookstown Public Realm Scheme M McCullagh informed members that FP McCann has commenced installation of parking restriction poles, required for parking enforcement throughout Cookstown Town Centre. N Bratton reminded members that legislation, approved by NI Assembly will follow. M McCullagh advised that most areas will be fully enforceable after parking restriction poles and plates are in place. The Chair enquired about the timescale for the said legislation being approved. -

Blackwater River Catchment
BLACKWATER DATA COLLATION FOR INTERREG V October 2015 CONTENTS Page number Introduction 3 WFD Status and Objectives 3 Managing freshwater resources in an integrated catchment 4 Groundwater in Integrated Catchment Management 5 Narrative summary 6 Results 6 Groundwater 10 River Blackwater Feeder GBNI1NB030307180 12 River Blackwater, Augher GBNI1NB030308223 15 Fury River GBNI1NB030307238 18 River Blackwater 5 GBNI1NB030308201 21 Cor River GBNI1NB030308245 24 River Blackwater 4 GBNI1NB030308204 27 River Blackwater 3 GBNI1NB030307043 30 River Blackwater 2 GBNI1NB030308203 33 River Rhone Lower GBNI1NB030307036 37 River Rhone Upper GBNI1NB030307025 40 Appendix 44 2 of 46 INTRODUCTION INTERREG Europe, financed by the European Regional Development Fund (ERDF), is scheduled to run from 2014 to 2020 http://www.interreg4c.eu/interreg-europe/. The ERDF budget for the overall INTERREG project is EUR 359 million. The Environment theme will receive a proportion of this funding. The purpose of this document is to demonstrate what information is currently available within NI Environment Agency (NIEA) and ROI Environmental Protection Agency (EPA) to assist with project proposals for river restoration schemes and integrated catchment management actions (including groundwater). This will save applicants duplicating studies already completed, while proposing additional types of information that can be collected. The report will provide information on the failing Water Framework Directive (WFD) quality elements for parts of the system. In addition there are impact assessments to guide how improvements may be progressed to meet WFD 2023 result indicator targets for INTERREG V. Any works to be carried out should be in line with current licensing and regulations1. The example given below is for the Blackwater Catchment. -

Dfi ROADS WESTERN DIVISION
DDffII RROOAADDSS WWEESSTTEERRNN DDIIVVIISSIIOONN RReeppoorrttt tttoo MMIIDD UULLSSTTEERR DDIISSTTRRIICCTT CCOOUUNNCCIILL SSpprriiinngg 22001199 1 Resurfacing works on the U711 Slaght Road, Cookstown CONTENTS PAGE Foreword by Divisional Roads Manager 3 – 4 Western Division 5 Senior Management Structure 6 1.0 Strategic Road Improvements 7 1.1 A5 Western Transport Corridor (A5WTC) 8 – 9 1.2 A29 Cookstown By-Pass 10 – 11 1.3 A6 Randalstown to Castledawson Dualling 11 – 12 2.0 Network Maintenance 13 – 15 2.1 Structural Maintenance Completed Works 2018-2019 16 – 25 2.2 Routine Maintenance Completed 2018 - 2019 26 – 27 2.3 Winter Service 28 2.4 Streetworks 29 2.5 Structural Maintenance Planned Works 2019-2020 30 – 38 3.0 Network Development 39 3.1 Local Transport and Safety Measures 40 3.1.1 Completed Works 2018-2019 40 – 45 3.1.2 Planned Works 2019-2020 46 – 49 3.2 Structures 50 3.2.1 Completed Works 2018-2019 51 – 52 3.2.2 Planned Works 2019-2020 52 – 54 3.3 Street Lighting 55 3.3.1 Completed Works 2018-2019 56 – 60 3.3.2 Planned Works 2019-2020 61 4.0 Network Planning 62 4.1 Planning Consultations 63 4.2 Private Streets 64 – 65 Useful Numbers 66 2 Foreword I have pleasure in submitting the 2019/2020 Annual Report on the work of DfI Roads across the Mid Ulster District Council Area. This report deals with works completed across the Council area during the year 2018/2019 and sets out our initial proposals for schemes to be undertaken in the year 2019/2020. -

Register of Employers 2021
REGISTER OF EMPLOYERS A Register of Concerns in which people are employed In accordance with Article 47 of the Fair Employment and Treatment (Northern Ireland) Order 1998 The Equality Commission for Northern Ireland Equality House 7-9 Shaftesbury Square Belfast BT2 7DP Tel: (02890) 500 600 E-mail: [email protected] August 2021 _______________________________________REGISTRATION The Register Under Article 47 of the Fair Employment and Treatment (Northern Ireland) Order 1998 the Commission has a duty to keep a Register of those concerns employing more than 10 people in Northern Ireland and to make the information contained in the Register available for inspection by members of the public. The Register is available for use by the public in the Commission’s office. Under the legislation, public authorities as specified by the Office of the First Minister and the Deputy First Minister are automatically treated as registered with the Commission. All other employers have a duty to register if they have more than 10 employees working 16 hours or more per week. Employers who meet the conditions for registration are given one month in which to apply for registration. This month begins from the end of the week in which the concern employed more than 10 employees in Northern Ireland. It is a criminal offence for such an employer not to apply for registration within this period. Persons who become employers in relation to a registered concern are also under a legal duty to apply to have their name and address entered on the Register within one month of becoming such an employer. -

Chief Executive
STRABANE IN WORLD WAR 1 As reported in The Strabane Chronicle & The Strabane Weekly News July 1914 – November 1919 Thanks are due to all those who contributed to the compilation of material for this research project. The group painstakingly combed the microfilm copies of the Strabane Chronicle and Strabane Weekly news and selected material and these included John Rogan, James Johnston, Joseph O’Kane, Hugh McGarrigle, Kathleen Patton, Chris McDermott, Pat McGuigan, William Allen, Ronnie Johnston, Michael Kennedy and John Dooher. Thanks are also due to Ms Geraldine Casey for her assistance. The group is grateful to the staff of Strabane Library for their unfailing help and to Libraries N.I. for making the resources available. Photo on front cover shows a military parade at The Diamond, Lifford, in 1914. CONTENTS 1914 page 4 1915 page 34 1916 page 146 1917 page 240 1918 page 318 1919 page 416 1914 Strabane Chronicle 4th July 1914 RURAL LABOUR PROBLEM There has been for many years the report states a marked scarcity of agricultural labourers, which was becoming more and more acute. The increase in the cost of living and the increased prices which the farmers was getting for his produce had been mainly instrumental in bringing about increased wages. The wages however are still very low. The usual daily wage current in 1913 were for men 2s to 3s 6d, for women 1s 6d to 3s. RESERVES CALLED UP IMMEDIATELY At the start of WW1 58,000 Irishmen were already enlisted in the British Regular Army or Navy – 21,000 serving regular soldiers, 18,000 reservists, 12,000 in the Special Reserve, 5,000 Naval ratings and 2,000 officers. -

Page 1 of 184
04 April 2019 Dear Councillor You are invited to attend a meeting of the Development Committee to be held in The Chamber, Cookstown at Mid Ulster District Council, Council Offices, COOKSTOWN, BT80 8DT on Wednesday, 03 April 2019 at 19:00 to transact the business noted below. Yours faithfully Anthony Tohill Chief Executive AGENDA OPEN BUSINESS 1. Apologies 2. Declarations of Interest 3. Chair's Business Matters for Decision 4. Community Development Report 3 - 104 5. Economic Development Report 105 - 130 6. Walk NI Consortium 2019-20 131 - 144 7. Recommendations on allocation of Schools’ Sports 145 - 148 Facilities Access Grants (Re-advertised) Matters for Information 8 Minutes of Development Committee held on 14 March 149 - 164 2019 9 Corporate Events 2019 165 - 170 10 Mid Ulster District Tourism Development Group 171 - 180 11 International Women’s Day 2019 181 - 184 Items restricted in accordance with Section 42, Part 1 of Schedule 6 of the Local Government Act (NI) 2014. The public will be asked to withdraw from the meeting at this point. Matters for Decision 12. Redevelopment of the former Maghera High School Site 13. Local Full Fibre Networks (LFFN) Challenge Fund Page 1 of 184 Matters for Information 14. Confidential Minutes of Development Committee held on 14 March 2019 Page 2 of 184 Report on Community Development Date of Meeting 11th April 2019 Reporting Officer Claire Linney, Head of Community Development Contact Officer Philip Clarke Community Support, Oliver Morgan Good Relations & Peace, Michael McCrory PCSP Is this report restricted for confidential business? Yes If ‘Yes’, confirm below the exempt information category relied upon No X 1.0 Purpose of Report 1.1 To agree the Community Grant awards. -
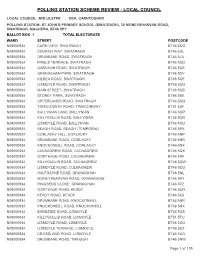
Polling Station Scheme Review - Local Council
POLLING STATION SCHEME REVIEW - LOCAL COUNCIL LOCAL COUNCIL: MID ULSTER DEA: CARNTOGHER POLLING STATION: ST JOHN'S PRIMARY SCHOOL (SWATRAGH), 30 MONEYSHARVAN ROAD, SWATRAGH, MAGHERA, BT46 5PY BALLOT BOX 1 TOTAL ELECTORATE WARD STREET POSTCODE N08000934CARN VIEW, SWATRAGH BT46 5QG N08000934CHURCH WAY, SWATRAGH BT46 5UL N08000934DRUMBANE ROAD, SWATRAGH BT46 5JA N08000934FRIELS TERRACE, SWATRAGH BT46 5QD N08000934GARVAGH ROAD, SWATRAGH BT46 5QE N08000934GRANAGHAN PARK, SWATRAGH BT46 5DY N08000934KILREA ROAD, SWATRAGH BT46 5QF N08000934LISMOYLE ROAD, SWATRAGH BT46 5QU N08000934MAIN STREET, SWATRAGH BT46 5QB N08000934STONEY PARK, SWATRAGH BT46 5BE N08000934UPPERLANDS ROAD, SWATRAGH BT46 5QQ N08000934TIMACONWAY ROAD, TIMACONWAY BT51 5UF N08000934BALLYNIAN LANE, BALLYNIAN BT46 5QP N08000934KILLYGULLIB ROAD, BALLYNIAN BT46 5QR N08000934LISMOYLE ROAD, BALLYNIAN BT46 5QU N08000934BEAGH ROAD, BEAGH (TEMPORAL) BT46 5PX N08000934CORLACKY HILL, CORLACKY BT46 5NP N08000934DRUMBANE ROAD, CORLACKY BT46 5NR N08000934KNOCKONEILL ROAD, CORLACKY BT46 5NX N08000934CULNAGREW ROAD, CULNAGREW BT46 5QX N08000934GORTEADE ROAD, CULNAGREW BT46 5RF N08000934KILLYGULLIB ROAD, CULNAGREW BT46 5QW N08000934LISMOYLE ROAD, CULNAGREW BT46 5QU N08000934HALFGAYNE ROAD, GRANAGHAN BT46 5NL N08000934MONEYSHARVAN ROAD, GRANAGHAN BT46 5PY N08000934RINGSEND CLOSE, GRANAGHAN BT46 5PZ N08000934GORTEADE ROAD, KEADY BT46 5QH N08000934KEADY ROAD, KEADY BT46 5QJ N08000934DRUMBANE ROAD, KNOCKONEILL BT46 5NR N08000934KNOCKONEILL ROAD, KNOCKONEILL BT46 5NX N08000934BARNSIDE ROAD, LISMOYLE