New Genes and Mechanisms of Recurrent Hydatidiform Moles
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Análise Integrativa De Perfis Transcricionais De Pacientes Com
UNIVERSIDADE DE SÃO PAULO FACULDADE DE MEDICINA DE RIBEIRÃO PRETO PROGRAMA DE PÓS-GRADUAÇÃO EM GENÉTICA ADRIANE FEIJÓ EVANGELISTA Análise integrativa de perfis transcricionais de pacientes com diabetes mellitus tipo 1, tipo 2 e gestacional, comparando-os com manifestações demográficas, clínicas, laboratoriais, fisiopatológicas e terapêuticas Ribeirão Preto – 2012 ADRIANE FEIJÓ EVANGELISTA Análise integrativa de perfis transcricionais de pacientes com diabetes mellitus tipo 1, tipo 2 e gestacional, comparando-os com manifestações demográficas, clínicas, laboratoriais, fisiopatológicas e terapêuticas Tese apresentada à Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo para obtenção do título de Doutor em Ciências. Área de Concentração: Genética Orientador: Prof. Dr. Eduardo Antonio Donadi Co-orientador: Prof. Dr. Geraldo A. S. Passos Ribeirão Preto – 2012 AUTORIZO A REPRODUÇÃO E DIVULGAÇÃO TOTAL OU PARCIAL DESTE TRABALHO, POR QUALQUER MEIO CONVENCIONAL OU ELETRÔNICO, PARA FINS DE ESTUDO E PESQUISA, DESDE QUE CITADA A FONTE. FICHA CATALOGRÁFICA Evangelista, Adriane Feijó Análise integrativa de perfis transcricionais de pacientes com diabetes mellitus tipo 1, tipo 2 e gestacional, comparando-os com manifestações demográficas, clínicas, laboratoriais, fisiopatológicas e terapêuticas. Ribeirão Preto, 2012 192p. Tese de Doutorado apresentada à Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo. Área de Concentração: Genética. Orientador: Donadi, Eduardo Antonio Co-orientador: Passos, Geraldo A. 1. Expressão gênica – microarrays 2. Análise bioinformática por module maps 3. Diabetes mellitus tipo 1 4. Diabetes mellitus tipo 2 5. Diabetes mellitus gestacional FOLHA DE APROVAÇÃO ADRIANE FEIJÓ EVANGELISTA Análise integrativa de perfis transcricionais de pacientes com diabetes mellitus tipo 1, tipo 2 e gestacional, comparando-os com manifestações demográficas, clínicas, laboratoriais, fisiopatológicas e terapêuticas. -

Control of Meiotic Double-Strand-Break Formation by ATM: Local and Global Views
bioRxiv preprint doi: https://doi.org/10.1101/236984; this version posted December 21, 2017. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Control of meiotic double-strand-break formation by ATM: local and global views Agnieszka Lukaszewicza, Julian Langeb,c, Scott Keeneyb,c, Maria Jasina aDevelopmental Biology Program, Memorial Sloan Kettering Cancer Center, New York, NY, USA bMolecular Biology Program, Memorial Sloan Kettering Cancer Center, New York, NY, USA cHoward Hughes Medical Institute, Memorial Sloan Kettering Cancer Center, New York, NY, USA To whom correspondence should be addressed: Scott Keeney: [email protected] Maria Jasin: [email protected] Key words: meiotic recombination, double-strand break (DSB), ATM/Tel1 kinase 1 bioRxiv preprint doi: https://doi.org/10.1101/236984; this version posted December 21, 2017. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. ABSTRACT DNA double-strand breaks (DSBs) generated by the SPO11 protein initiate meiotic recombination, an essential process for successful chromosome segregation during gametogenesis. The activity of SPO11 is controlled by multiple factors and regulatory mechanisms, such that the number of DSBs is limited and DSBs form at distinct positions in the genome and at the right time. -

Linkage Analysis of a Model Quantitative Trait in Humans: Finger Ridge Count Shows Significant Multivariate Linkage to 5Q14.1 Sarah E
Virginia Commonwealth University VCU Scholars Compass Psychiatry Publications Dept. of Psychiatry 2007 Linkage Analysis of a Model Quantitative Trait in Humans: Finger Ridge Count Shows Significant Multivariate Linkage to 5q14.1 Sarah E. Medland Queensland Institute of Medical Research Danuta Z. Loesch La Trobe University Bogdan Mdzewski La Trobe University See next page for additional authors Follow this and additional works at: http://scholarscompass.vcu.edu/psych_pubs Part of the Psychiatry and Psychology Commons Copyright: © 2007 Medland et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Downloaded from http://scholarscompass.vcu.edu/psych_pubs/30 This Article is brought to you for free and open access by the Dept. of Psychiatry at VCU Scholars Compass. It has been accepted for inclusion in Psychiatry Publications by an authorized administrator of VCU Scholars Compass. For more information, please contact [email protected]. Authors Sarah E. Medland, Danuta Z. Loesch, Bogdan Mdzewski, Gu Zhu, Grant W. Montgomery, and Nicholas G. Martin This article is available at VCU Scholars Compass: http://scholarscompass.vcu.edu/psych_pubs/30 Linkage Analysis of a Model Quantitative Trait in Humans: Finger Ridge Count Shows Significant Multivariate Linkage to 5q14.1 Sarah E. Medland1,2*, Danuta Z. Loesch3, Bogdan Mdzewski3 , Gu Zhu1, Grant W. Montgomery1, Nicholas G. Martin1 1 Genetic Epidemiology Unit, Queensland Institute of Medical Research, Brisbane, Australia, 2 Virginia Institute of Psychiatric and Behavioral Genetics, Virginia Commonwealth University, Richmond, Virginia, United States, 3 Department of Psychological Science, La Trobe University, Melbourne, Australia The finger ridge count (a measure of pattern size) is one of the most heritable complex traits studied in humans and has been considered a model human polygenic trait in quantitative genetic analysis. -

Numerical Constraints and Feedback Control of Double-Strand Breaks in Mouse Meiosis
Downloaded from genesdev.cshlp.org on October 5, 2021 - Published by Cold Spring Harbor Laboratory Press Numerical constraints and feedback control of double-strand breaks in mouse meiosis Liisa Kauppi,1,2,3 Marco Barchi,4,5,8 Julian Lange,1,8 Fre´de´ric Baudat,4,6 Maria Jasin,4,9 and Scott Keeney1,7,9 1Molecular Biology Program, Memorial Sloan-Kettering Cancer Center, New York, New York 10065, USA; 2Research Programs Unit (Genome-Scale Biology), 3Institute of Biomedicine (Biochemistry and Developmental Biology), University of Helsinki, Helsinki FIN-00014, Finland; 4Developmental Biology Program, Memorial Sloan-Kettering Cancer Center, New York, New York 10065, USA; 5Department of Biomedicine and Prevention, Section of Anatomy, University of Rome Tor Vergata, 00133 Rome, Italy; 6Institute of Human Genetics, UPR1142/Centre National de la Recherche Scientifique (CNRS), 34936 Montpellier CEDEX 5, France; 7Howard Hughes Medical Institute, Memorial Sloan-Kettering Cancer Center, New York, New York 10065, USA Different organisms display widely different numbers of the programmed double-strand breaks (DSBs) that initiate meiotic recombination (e.g., hundreds per meiocyte in mice and humans vs. dozens in nematodes), but little is known about what drives these species-specific DSB set points or the regulatory pathways that control them. Here we examine male mice with a lowered dosage of SPO11, the meiotic DSB catalyst, to gain insight into the effect of reduced DSB numbers on mammalian chromosome dynamics. An approximately twofold DSB reduction was associated with the reduced ability of homologs to synapse along their lengths, provoking prophase arrest and, ultimately, sterility. In many spermatocytes, chromosome subsets displayed a mix of synaptic failure and synapsis with both homologous and nonhomologous partners (‘‘chromosome tangles’’). -

Transdifferentiation of Human Mesenchymal Stem Cells
Transdifferentiation of Human Mesenchymal Stem Cells Dissertation zur Erlangung des naturwissenschaftlichen Doktorgrades der Julius-Maximilians-Universität Würzburg vorgelegt von Tatjana Schilling aus San Miguel de Tucuman, Argentinien Würzburg, 2007 Eingereicht am: Mitglieder der Promotionskommission: Vorsitzender: Prof. Dr. Martin J. Müller Gutachter: PD Dr. Norbert Schütze Gutachter: Prof. Dr. Georg Krohne Tag des Promotionskolloquiums: Doktorurkunde ausgehändigt am: Hiermit erkläre ich ehrenwörtlich, dass ich die vorliegende Dissertation selbstständig angefertigt und keine anderen als die von mir angegebenen Hilfsmittel und Quellen verwendet habe. Des Weiteren erkläre ich, dass diese Arbeit weder in gleicher noch in ähnlicher Form in einem Prüfungsverfahren vorgelegen hat und ich noch keinen Promotionsversuch unternommen habe. Gerbrunn, 4. Mai 2007 Tatjana Schilling Table of contents i Table of contents 1 Summary ........................................................................................................................ 1 1.1 Summary.................................................................................................................... 1 1.2 Zusammenfassung..................................................................................................... 2 2 Introduction.................................................................................................................... 4 2.1 Osteoporosis and the fatty degeneration of the bone marrow..................................... 4 2.2 Adipose and bone -

Zimmer Cell Calcium 2013 Mammalian S100 Evolution.Pdf
Cell Calcium 53 (2013) 170–179 Contents lists available at SciVerse ScienceDirect Cell Calcium jo urnal homepage: www.elsevier.com/locate/ceca Evolution of the S100 family of calcium sensor proteins a,∗ b b,1 b Danna B. Zimmer , Jeannine O. Eubanks , Dhivya Ramakrishnan , Michael F. Criscitiello a Center for Biomolecular Therapeutics and Department of Biochemistry & Molecular Biology, University of Maryland School of Medicine, 108 North Greene Street, Baltimore, MD 20102, United States b Comparative Immunogenetics Laboratory, Department of Veterinary Pathobiology, College of Veterinary Medicine & Biomedical Sciences, Texas A&M University, College Station, TX 77843-4467, United States a r t i c l e i n f o a b s t r a c t 2+ Article history: The S100s are a large group of Ca sensors found exclusively in vertebrates. Transcriptomic and genomic Received 4 October 2012 data from the major radiations of mammals were used to derive the evolution of the mammalian Received in revised form 1 November 2012 S100s genes. In human and mouse, S100s and S100 fused-type proteins are in a separate clade from Accepted 3 November 2012 2+ other Ca sensor proteins, indicating that an ancient bifurcation between these two gene lineages Available online 14 December 2012 has occurred. Furthermore, the five genomic loci containing S100 genes have remained largely intact during the past 165 million years since the shared ancestor of egg-laying and placental mammals. Keywords: Nonetheless, interesting births and deaths of S100 genes have occurred during mammalian evolution. Mammals The S100A7 loci exhibited the most plasticity and phylogenetic analyses clarified relationships between Phylogenetic analyses the S100A7 proteins encoded in the various mammalian genomes. -
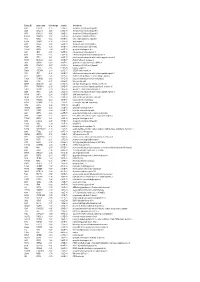
Entrez ID Gene Name Fold Change Q-Value Description
Entrez ID gene name fold change q-value description 4283 CXCL9 -7.25 5.28E-05 chemokine (C-X-C motif) ligand 9 3627 CXCL10 -6.88 6.58E-05 chemokine (C-X-C motif) ligand 10 6373 CXCL11 -5.65 3.69E-04 chemokine (C-X-C motif) ligand 11 405753 DUOXA2 -3.97 3.05E-06 dual oxidase maturation factor 2 4843 NOS2 -3.62 5.43E-03 nitric oxide synthase 2, inducible 50506 DUOX2 -3.24 5.01E-06 dual oxidase 2 6355 CCL8 -3.07 3.67E-03 chemokine (C-C motif) ligand 8 10964 IFI44L -3.06 4.43E-04 interferon-induced protein 44-like 115362 GBP5 -2.94 6.83E-04 guanylate binding protein 5 3620 IDO1 -2.91 5.65E-06 indoleamine 2,3-dioxygenase 1 8519 IFITM1 -2.67 5.65E-06 interferon induced transmembrane protein 1 3433 IFIT2 -2.61 2.28E-03 interferon-induced protein with tetratricopeptide repeats 2 54898 ELOVL2 -2.61 4.38E-07 ELOVL fatty acid elongase 2 2892 GRIA3 -2.60 3.06E-05 glutamate receptor, ionotropic, AMPA 3 6376 CX3CL1 -2.57 4.43E-04 chemokine (C-X3-C motif) ligand 1 7098 TLR3 -2.55 5.76E-06 toll-like receptor 3 79689 STEAP4 -2.50 8.35E-05 STEAP family member 4 3434 IFIT1 -2.48 2.64E-03 interferon-induced protein with tetratricopeptide repeats 1 4321 MMP12 -2.45 2.30E-04 matrix metallopeptidase 12 (macrophage elastase) 10826 FAXDC2 -2.42 5.01E-06 fatty acid hydroxylase domain containing 2 8626 TP63 -2.41 2.02E-05 tumor protein p63 64577 ALDH8A1 -2.41 6.05E-06 aldehyde dehydrogenase 8 family, member A1 8740 TNFSF14 -2.40 6.35E-05 tumor necrosis factor (ligand) superfamily, member 14 10417 SPON2 -2.39 2.46E-06 spondin 2, extracellular matrix protein 3437 -

Motif Signatures in Stretch Enhancers Are Enriched for Disease-Associated Genetic Variants
Quang et al. Epigenetics & Chromatin (2015) 8:23 DOI 10.1186/s13072-015-0015-7 RESEARCH Open Access Motif signatures in stretch enhancers are enriched for disease‑associated genetic variants Daniel X Quang1,2, Michael R Erdos3, Stephen C J Parker4*† and Francis S Collins3† Abstract Background: Stretch enhancers (SEs) are large chromatin-defned regulatory elements that are at least 3,000 base pairs (bps) long, in contrast to the median enhancer length of 800 bps. SEs tend to be cell-type specifc, regulate cell- type specifc gene expression, and are enriched in disease-associated genetic variants in disease-relevant cell types. Transcription factors (TFs) can bind to enhancers to modulate enhancer activity, and their sequence specifcity can be represented by motifs. We hypothesize motifs can provide a biological context for how genetic variants contribute to disease. Results: We integrated chromatin state, gene expression, and chromatin accessibility [measured as DNase I Hyper- sensitive Sites (DHSs)] maps across nine diferent cell types. Motif enrichment analyses of chromatin-defned enhancer sequences identify several known cell-type specifc “master” factors. Furthermore, de novo motif discovery not only recovers many of these motifs, but also identifes novel non-canonical motifs, providing additional insight into TF binding preferences. Across the length of SEs, motifs are most enriched in DHSs, though relative enrichment is also observed outside of DHSs. Interestingly, we show that single nucleotide polymorphisms associated with diseases or quantitative traits signifcantly overlap motif occurrences located in SEs, but outside of DHSs. Conclusions: These results reinforce the role of SEs in infuencing risk for diseases and suggest an expanded regu- latory functional role for motifs that occur outside highly accessible chromatin. -

Human Pancreatic Islet Three-Dimensional Chromatin Architecture Provides Insights Into the Genetics of Type 2 Diabetes
ARTICLES https://doi.org/10.1038/s41588-019-0457-0 Human pancreatic islet three-dimensional chromatin architecture provides insights into the genetics of type 2 diabetes Irene Miguel-Escalada1,2,3,4,33, Silvia Bonàs-Guarch1,2,3,4,33, Ines Cebola 1,33, Joan Ponsa-Cobas 1, Julen Mendieta-Esteban 5, Goutham Atla1,2,3,4, Biola M. Javierre6,7, Delphine M. Y. Rolando1, Irene Farabella 5, Claire C. Morgan1,2, Javier García-Hurtado2,3,4, Anthony Beucher1, Ignasi Morán 1,8, Lorenzo Pasquali 3,7,9, Mireia Ramos-Rodríguez9, Emil V. R. Appel 10, Allan Linneberg 11,12, Anette P. Gjesing10, Daniel R. Witte13,14, Oluf Pedersen 10, Niels Grarup 10, Philippe Ravassard 15, David Torrents8,16, Josep M. Mercader 8,17,18, Lorenzo Piemonti 19,20, Thierry Berney 21, Eelco J. P. de Koning22,23, Julie Kerr-Conte24, Francois Pattou 24, Iryna O. Fedko25,26, Leif Groop 27, Inga Prokopenko 28,29, Torben Hansen 10, Marc A. Marti-Renom 5,16,30,31, Peter Fraser 6,32 and Jorge Ferrer 1,2,3* Genetic studies promise to provide insight into the molecular mechanisms underlying type 2 diabetes (T2D). Variants asso- ciated with T2D are often located in tissue-specific enhancer clusters or super-enhancers. So far, such domains have been defined through clustering of enhancers in linear genome maps rather than in three-dimensional (3D) space. Furthermore, their target genes are often unknown. We have created promoter capture Hi-C maps in human pancreatic islets. This linked diabetes- associated enhancers to their target genes, often located hundreds of kilobases away. -

Modelling the Developmental Spliceosomal Craniofacial Disorder
bioRxiv preprint doi: https://doi.org/10.1101/2020.05.13.094029; this version posted May 14, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Modelling the developmental spliceosomal craniofacial disorder Burn -McKeown syndrome using induced pluripotent stem cells Short title: Modelling Burn -McKeown Syndrome using induced pluripotent stem cells Katherine A. Wood 1,2 , Charlie F. Rowlands 1,2 , Huw B. Thomas 1, Steven Woods 3, Julieta O’Flaherty 3, Sofia Dou zg ou 1,2 , Su san J. Kimbe r3, William G. Newman 1,2 *,Raymond T. O’Keefe 1* 1Division of Evolution and Genomic Sciences, School of Biological Sciences, Faculty of Biology, Medicine and Health, The University of Manchester, UK 2Manchester Centre for Genomic Medicine , Manchester University NHS Foundation Trust , Manchester Academic Health Science Centre, Manc hester, UK 3Division of Cell Matrix Biology and Regenerative Medicine, School of Biology, Faculty of Biology, Medicine and Health, University of Manchester, Manchester, UK *To whom correspondence should be addressed. Email: [email protected] ; [email protected] 1 bioRxiv preprint doi: https://doi.org/10.1101/2020.05.13.094029; this version posted May 14, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. -

Pancreatic Islet Transcriptional Enhancers and Diabetes
Current Diabetes Reports (2019) 19:145 https://doi.org/10.1007/s11892-019-1230-6 GENETICS (AP MORRIS, SECTION EDITOR) Pancreatic Islet Transcriptional Enhancers and Diabetes Inês Cebola1 # The Author(s) 2019 Abstract Purpose of Review Common genetic variants that associate with type 2 diabetes risk are markedly enriched in pancreatic islet transcriptional enhancers. This review discusses current advances in the annotation of islet enhancer variants and their target genes. Recent Findings Recent methodological advances now allow genetic and functional mapping of diabetes causal variants at unprecedented resolution. Mapping of enhancer-promoter interactions in human islets has provided a unique appreciation of the complexity of islet gene regulatory processes and enabled direct association of noncoding diabetes risk variants to their target genes. Summary The recently improved human islet enhancer annotations constitute a framework for the interpretation of diabetes genetic signals in the context of pancreatic islet gene regulation. In the future, integration of existing and yet to come regulatory maps with genetic fine-mapping efforts and in-depth functional characterization will foster the discovery of novel diabetes molecular risk mechanisms. Keywords Transcriptional enhancers . Human genetics . Type 2 diabetes . Gene regulation . Epigenomics . Noncoding genome function Introduction associated traits are noncoding and concentrate within ac- cessible chromatin regions of disease-relevant tissues [7]. In recent years, clinical genomics and the investigation of This observation is also true for type 2 diabetes (T2D), for noncoding genome functions, including microRNAs which common noncoding variants predominantly influ- (miRNAs), long noncoding RNAs (lncRNAs) and tran- ence risk [8•], residing in pancreatic islet transcriptional scriptional enhancers, have proved to be fertile ground enhancers [9–12, 13••, 14, 15], particularly within clus- to the discovery of genetic disease mechanisms [1]. -

Content Based Search in Gene Expression Databases and a Meta-Analysis of Host Responses to Infection
Content Based Search in Gene Expression Databases and a Meta-analysis of Host Responses to Infection A Thesis Submitted to the Faculty of Drexel University by Francis X. Bell in partial fulfillment of the requirements for the degree of Doctor of Philosophy November 2015 c Copyright 2015 Francis X. Bell. All Rights Reserved. ii Acknowledgments I would like to acknowledge and thank my advisor, Dr. Ahmet Sacan. Without his advice, support, and patience I would not have been able to accomplish all that I have. I would also like to thank my committee members and the Biomed Faculty that have guided me. I would like to give a special thanks for the members of the bioinformatics lab, in particular the members of the Sacan lab: Rehman Qureshi, Daisy Heng Yang, April Chunyu Zhao, and Yiqian Zhou. Thank you for creating a pleasant and friendly environment in the lab. I give the members of my family my sincerest gratitude for all that they have done for me. I cannot begin to repay my parents for their sacrifices. I am eternally grateful for everything they have done. The support of my sisters and their encouragement gave me the strength to persevere to the end. iii Table of Contents LIST OF TABLES.......................................................................... vii LIST OF FIGURES ........................................................................ xiv ABSTRACT ................................................................................ xvii 1. A BRIEF INTRODUCTION TO GENE EXPRESSION............................. 1 1.1 Central Dogma of Molecular Biology........................................... 1 1.1.1 Basic Transfers .......................................................... 1 1.1.2 Uncommon Transfers ................................................... 3 1.2 Gene Expression ................................................................. 4 1.2.1 Estimating Gene Expression ............................................ 4 1.2.2 DNA Microarrays ......................................................