Frequently Asked Questions About CPT Coding
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Routine Use of Feeding Jejunostomy in Pancreaticoduodenectomuy: A
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 95 JuneSeptember 2020 2020 doi:10.20944/preprints202006.0114.v1 doi:10.20944/preprints202006.0114.v2 Routine use of Feeding Jejunostomy in Pancreaticoduodenectomuy: A Metaanalysis. DR.Bhavin Vasavada Consultant HepatoPancreaticobiliary and Liver Transplant Surgeon, Shalby Hospitals, Ahmedabad. Email: [email protected] Dr.Hardik Patel Consultant HepatoPancreaticobiliary and Liver Transplant Surgeon, Shalby Hospitals, Ahmedabad. Conflict of Interests: none. Funding disclosure: none. Abbreviations: Post operative pancreatic fistula (POPF), total parentral nutrition (TPN), Surgical site infections. (SSI) Keywords: Pancreaticoduodenectomy; feeding jejunostomy; morbidity; mortality Abstract: Aims and objectives: The primary aim of our study was to evaluate morbidity and mortality following feeding jejunostomy in pancreaticoduodenectomy compared to the control group. We © 2020 by the author(s). Distributed under a Creative Commons CC BY license. Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 95 JuneSeptember 2020 2020 doi:10.20944/preprints202006.0114.v1 doi:10.20944/preprints202006.0114.v2 also evaluated individual complications like delayed gastric emptying, post operative pancreatic fistula, superficial and deep surgical site infection. We also looked for time to start oral nutrition and requirement of total parentral nutrition. Material and Methods: The study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and MOOSE guidelines. [9,10]. We searched pubmed, cochrane library, embase, google scholar with keywords like “feeding jejunostomy in pancreaticodudenectomy”, “entral nutrition in pancreaticoduodenectomy, “total parentral nutrition in pancreaticoduodenectomy’, “morbidity and mortality following pancreaticoduodenectomy”. Two independent authors extracted the data (B.V and H.P). The meta-analysis was conducted using Open meta-analysis software. -

Laparoscopic Truncal Vagotomy and Gatrojejunostomy for Pyloric Stenosis
ORIGINAL ARTICLE pISSN 2234-778X •eISSN 2234-5248 J Minim Invasive Surg 2015;18(2):48-52 Journal of Minimally Invasive Surgery Laparoscopic Truncal Vagotomy and Gatrojejunostomy for Pyloric Stenosis Jung-Wook Suh, M.D.1, Ye Seob Jee, M.D., Ph.D.1,2 Department of Surgery, 1Dankook University Hospital, 2Dankook University School of Medicine, Cheonan, Korea Purpose: Peptic ulcer disease (PUD) remains one of the most prevalent gastrointestinal diseases and Received January 27, 2015 an important target for surgical treatment. Laparoscopy applies to most surgical procedures; however Revised 1st March 9, 2015 its use in elective peptic ulcer surgery, particularly in cases of pyloric stenosis, has not been popular. 2nd March 28, 2015 The aim of this study was to describe the role of laparoscopic surgery and an easily performed Accepted April 20, 2015 procedure for pyloric stenosis. We accordingly performed laparoscopic truncal vagotomy with gastrojejunostomy in 10 consecutive patients with pyloric stenosis. Corresponding author Ye Seob Jee Methods: Data were collected prospectively from all patients who underwent laparoscopic truncal Department of Surgery, Dankook vagotomy with gastrojejunostomy from August 2009 to May 2014 and reviewed retrospectively. University Hospital, Dankook Results: A total of 10 patients underwent laparoscopic trucal vagotomy with gastrojejunostomy for University School of Medicine, 119, peptic ulcer obstruction from August 2009 to May 2014 in ○○ university hospital. The mean age was Dandae-ro, Dongnam-gu, Cheonan 62.6 (±16.4) years old and mean BMI was 19.3 (±2.5) kg/m2. There were no conversions to open 330-714, Korea surgery and no occurrence of intra-operative complications. -

Utility of the Digital Rectal Examination in the Emergency Department: a Review
The Journal of Emergency Medicine, Vol. 43, No. 6, pp. 1196–1204, 2012 Published by Elsevier Inc. Printed in the USA 0736-4679/$ - see front matter http://dx.doi.org/10.1016/j.jemermed.2012.06.015 Clinical Reviews UTILITY OF THE DIGITAL RECTAL EXAMINATION IN THE EMERGENCY DEPARTMENT: A REVIEW Chad Kessler, MD, MHPE*† and Stephen J. Bauer, MD† *Department of Emergency Medicine, Jesse Brown VA Medical Center and †University of Illinois-Chicago College of Medicine, Chicago, Illinois Reprint Address: Chad Kessler, MD, MHPE, Department of Emergency Medicine, Jesse Brown Veterans Hospital, 820 S Damen Ave., M/C 111, Chicago, IL 60612 , Abstract—Background: The digital rectal examination abdominal pain and acute appendicitis. Stool obtained by (DRE) has been reflexively performed to evaluate common DRE doesn’t seem to increase the false-positive rate of chief complaints in the Emergency Department without FOBTs, and the DRE correlated moderately well with anal knowing its true utility in diagnosis. Objective: Medical lit- manometric measurements in determining anal sphincter erature databases were searched for the most relevant arti- tone. Published by Elsevier Inc. cles pertaining to: the utility of the DRE in evaluating abdominal pain and acute appendicitis, the false-positive , Keywords—digital rectal; utility; review; Emergency rate of fecal occult blood tests (FOBT) from stool obtained Department; evidence-based medicine by DRE or spontaneous passage, and the correlation be- tween DRE and anal manometry in determining anal tone. Discussion: Sixteen articles met our inclusion criteria; there INTRODUCTION were two for abdominal pain, five for appendicitis, six for anal tone, and three for fecal occult blood. -

The Differences Between ICD-9 and ICD-10
Preparing for the ICD-10 Code Set: Fact Sheet 2 October 1, 2015 Compliance Date Get the Facts to be Compliant Alert: The new ICD-10 compliance date is October 1, 2015. The Differences Between ICD-9 and ICD-10 This is the second fact sheet in a series and is focused on the differences between the ICD-9 and ICD-10 code sets. Collectively, the fact sheets will provide information, guidance, and checklists to assist you with understanding what you need to do to implement the ICD-10 code set. The ICD-10 code sets are not a simple update of the ICD-9 code set. The ICD-10 code sets have fundamental changes in structure and concepts that make them very different from ICD-9. Because of these differences, it is important to develop a preliminary understanding of the changes from ICD-9 to ICD-10. This basic understanding of the differences will then identify more detailed training that will be needed to appropriately use the ICD-10 code sets. In addition, seeing the differences between the code sets will raise awareness of the complexities of converting to the ICD-10 codes. Overall Comparisons of ICD-9 to ICD-10 Issues today with the ICD-9 diagnosis and procedure code sets are addressed in ICD-10. One concern today with ICD-9 is the lack of specificity of the information conveyed in the codes. For example, if a patient is seen for treatment of a burn on the right arm, the ICD-9 diagnosis code does not distinguish that the burn is on the right arm. -

The American Society of Colon and Rectal Surgeons' Clinical Practice
CLINICAL PRACTICE GUIDELINES The American Society of Colon and Rectal Surgeons’ Clinical Practice Guideline for the Evaluation and Management of Constipation Ian M. Paquette, M.D. • Madhulika Varma, M.D. • Charles Ternent, M.D. Genevieve Melton-Meaux, M.D. • Janice F. Rafferty, M.D. • Daniel Feingold, M.D. Scott R. Steele, M.D. he American Society of Colon and Rectal Surgeons for functional constipation include at least 2 of the fol- is dedicated to assuring high-quality patient care lowing symptoms during ≥25% of defecations: straining, Tby advancing the science, prevention, and manage- lumpy or hard stools, sensation of incomplete evacuation, ment of disorders and diseases of the colon, rectum, and sensation of anorectal obstruction or blockage, relying on anus. The Clinical Practice Guidelines Committee is com- manual maneuvers to promote defecation, and having less posed of Society members who are chosen because they than 3 unassisted bowel movements per week.7,8 These cri- XXX have demonstrated expertise in the specialty of colon and teria include constipation related to the 3 common sub- rectal surgery. This committee was created to lead inter- types: colonic inertia or slow transit constipation, normal national efforts in defining quality care for conditions re- transit constipation, and pelvic floor or defecation dys- lated to the colon, rectum, and anus. This is accompanied function. However, in reality, many patients demonstrate by developing Clinical Practice Guidelines based on the symptoms attributable to more than 1 constipation sub- best available evidence. These guidelines are inclusive and type and to constipation-predominant IBS, as well. The not prescriptive. -
OT Resource for K9 Overview of Surgical Procedures
OT Resource for K9 Overview of surgical procedures Prepared by: Hannah Woolley Stage Level 1 2 Gynecology/Oncology Surgeries Lymphadenectomy (lymph node dissection) Surgical removal of lymph nodes Radical: most/all of the lymph nodes in tumour area are removed Regional: some of the lymph nodes in the tumour area are removed Omentectomy Surgical procedure to remove the omentum (thin abdominal tissue that encases the stomach, large intestine and other abdominal organs) Indications for omenectomy: Ovarian cancer Sometimes performed in combination with TAH/BSO Posterior Pelvic Exenteration Surgical removal of rectum, anus, portion of the large intestine, ovaries, fallopian tubes and uterus (partial or total removal of the vagina may also be indicated) Indications for pelvic exenteration Gastrointestinal cancer (bowel, colon, rectal) Gynecological cancer (cervical, vaginal, ovarian, vulvar) Radical Cystectomy Surgical removal of the whole bladder and proximal lymph nodes In men, prostate gland is also removed In women, ovaries and uterus may also be removed Following surgery: Urostomy (directs urine through a stoma on the abdomen) Recto sigmoid pouch/Mainz II pouch (segment of the rectum and sigmoid colon used to provide anal urinary diversion) 3 Radical Vulvectomy Surgical removal of entire vulva (labia, clitoris, vestibule, introitus, urethral meatus, glands/ducts) and surrounding lymph nodes Indication for radical vulvectomy Treatment of vulvar cancer (most common) Sentinel Lymph Node Dissection (SLND) Exploratory procedure where the sentinel lymph node is removed and examined to determine if there is lymph node involvement in patients diagnosed with cancer (commonly breast cancer) Total abdominal hysterectomy/bilateral saplingo-oophorectomy (TAH/BSO) Surgical removal of the uterus (including cervix), both fallopian tubes and ovaries Indications for TAH/BSO: Uterine fibroids: benign growths in the muscle of the uterus Endometriosis: condition where uterine tissue grows on structures outside the uterus (i.e. -
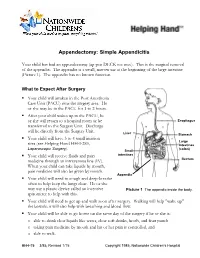
Appendectomy: Simple Appendicitis
Appendectomy: Simple Appendicitis Your child has had an appendectomy (ap pen DECK toe mee). This is the surgical removal of the appendix. The appendix is a small, narrow sac at the beginning of the large intestine (Picture 1). The appendix has no known function. What to Expect After Surgery . Your child will awaken in the Post Anesthesia Care Unit (PACU) near the surgery area. He or she may be in the PACU for 1 to 2 hours. After your child wakes up in the PACU, he or she will return to a hospital room or be Esophagus transferred to the Surgery Unit. Discharge will be directly from the Surgery Unit. Liver Stomach . Your child will have 3 to 4 small incision Large sites (see Helping Hand HH-I-283, Intestines Laparoscopic Surgery (colon) ). Small . Your child will receive fluids and pain intestines medicine through an intravenous line (IV). Rectum When your child can take liquids by mouth, pain medicine will also be given by mouth. Appendix . Your child will need to cough and deep-breathe often to help keep the lungs clear. He or she may use a plastic device called an incentive Picture 1 The appendix inside the body. spirometer to help with this. Your child will need to get up and walk soon after surgery. Walking will help "wake up" the bowels; it will also help with breathing and blood flow. Your child will be able to go home on the same day of the surgery if he or she is: o able to drink clear liquids like water, clear soft drinks, broth, and fruit punch o taking pain medicine by mouth and his or her pain is controlled, and o able to walk. -

Intestine Transplant Manual
Intestine Transplant Manual Toronto Intestine Transplant Program TRANSPLANT MANUAL E INTESTIN This manual is dedicated to our donors, our patients and their families Acknowledgements Dr. Mark Cattral, MD, (FRCSC) Dr. Yaron Avitzur, MD Andrea Norgate, RN, BScN Sonali Pendharkar, BA (Hons), BSW, MSW, RSW Anna Richardson, RD We acknowledge the contribution of previous members of the team and to Cheryl Beriault (RN, BScN) for creating this manual. 2 TABLE OF CONTENTS Dedications and Acknowledgements 2 Welcome 5 Our Values and Philosophy of Care Our Expectations of You Your Transplant Team 6 The Function of the Liver and Intestines 9 Where are the abdominal organs located and what do they look like? What does your Stomach do? What does your Intestine do? What does your Liver do? What does your Pancreas do? When Does a Patient Need an Intestine Transplant? 12 Classification of Intestine Failure Am I Eligible for an Intestine Transplant? Advantages and Disadvantages of Intestine Transplant The Transplant Assessment 14 Investigations Consultations Active Listing for Intestine Transplantation (Placement on the List) 15 Preparing for the Intestine Transplant Trillium Drug Program Other Sources of Funding for Drug Coverage Financial Planning Insurance Issues Other Financial Considerations Related to the Hospital Stay Legal Considerations for Transplant Patients Advance Care Planning Waiting for the Intestine Transplant 25 Your Place on the Waiting List Maintaining Contact with the Transplant Team Coping with Stress Maintaining your Health While -

Information for Patients Having a Sigmoid Colectomy
Patient information – Pre-operative Assessment Clinic Information for patients having a sigmoid colectomy This leaflet will explain what will happen when you come to the hospital for your operation. It is important that you understand what to expect and feel able to take an active role in your treatment. Your surgeon will have already discussed your treatment with you and will give advice about what to do when you get home. What is a sigmoid colectomy? This operation involves removing the sigmoid colon, which lies on the left side of your abdominal cavity (tummy). We would then normally join the remaining left colon to the top of the rectum (the ‘storage’ organ of the bowel). The lines on the attached diagram show the piece of bowel being removed. This operation is done with you asleep (general anaesthetic). The operation not only removes the bowel containing the tumour but also removes the draining lymph glands from this part of the bowel. This is sent to the pathologists who will then analyse each bit of the bowel and the lymph glands in detail under the microscope. This operation can often be completed in a ‘keyhole’ manner, which means less trauma to the abdominal muscles, as the biggest wound is the one to remove the bowel from the abdomen. Sometimes, this is not possible, in which case the same operation is done through a bigger incision in the abdominal wall – this is called an ‘open’ operation. It does take longer to recover with an open operation but, if it is necessary, it is the safest thing to do. -

Tube Feeding Protocol: Supporting an Individual with a Feeding Tube
Tube Feeding Protocol: Supporting an Individual with a Feeding Tube Introduction Some people may be unable to take foods or fluids by mouth due to dysphagia. Others may require supplementation because they are unable to take sufficient foods or fluids by mouth, and formula delivered through a feeding tube may provide them with much needed additional nutrients. It is helpful if guidelines (A Tube Feeding Protocol) are in place prior to the need for this intervention. Below are some suggested guidelines for supporting an Individual with a feeding tube. Information to be documented by the physician The reason (medical diagnosis) requiring feeding tube insertion Type of feeding tube inserted Types of feeding tubes The Nasogastric Tube (NG tube): Passed into either nostril, down the esophagus and into the stomach. This is used for short term feedings. The Gastrostomy tube (G - tube or PEG): Surgically placed through the abdominal wall into the stomach. The tube will be located below the rib cage and to the left. The Jejunostomy tube (J - tube or PEJ): Surgically implanted in the upper portion of the jejunum (Part of the small intestine.) The tube will be located lower in the abdomen and more toward the center than the G – tube. Feedings through a J – tube must always be by pump. The Gastrostomy-Jejunostomy (GJ - tube): Surgically placed in the stomach, like the G – tube, but the tubing is longer, the end is in the jejunum, and there are two ports. Feeding technique Feeding techniques Bolus: A set amount of formula is given over a short period of time via syringe. -

Enteroliths in a Kock Continent Ileostomy: Case Report and Review of the Literature
E200 Cases and Techniques Library (CTL) similar symptoms recurred 2 years later. A second ileoscopy showed a narrowed Enteroliths in a Kock continent ileostomy: efferent loop that was dilated by insertion case report and review of the literature of the colonoscope, with successful relief of her symptoms. Chemical analysis of one of the retrieved enteroliths revealed calcium oxalate crystals. Five cases have previously been noted in the literature Fig. 1 Schematic (●" Table 1). representation of a Kock continent The alkaline milieu of succus entericus in ileostomy. the ileum may induce the precipitation of a calcium oxalate concretion; in contrast, the acidic milieu found more proximally in the intestine enhances the solubility of calcium. The gradual precipitation of un- conjugated bile salts, calcium oxalate, and Valve calcium carbonate crystals around a nidus composed of fecal material or undigested Efferent loop fiber can lead to the formation of calcium oxalate calculi over time [5]. Endoscopy_UCTN_Code_CCL_1AD_2AJ Reservoir Competing interests: None Hadi Moattar1, Jakob Begun1,2, Timothy Florin1,2 1 Department of Gastroenterology, Mater Adult Hospital, South Brisbane, Australia The Kock continent ileostomy (KCI) was dure was done to treat ulcerative pan- 2 Mater Research, University of Queens- designed by Nik Kock, who used an intus- colitis complicated by colon cancer. She land, Translational Research Institute, suscepted ileostomy loop to create a nip- had a well-functioning KCI that she had Woolloongabba, Australia ple valve (●" Fig.1) that would not leak catheterized daily for 34 years before she and would allow ileal effluent to be evac- presented with intermittent abdominal uated with a catheter [1]. -

Septicaemia After Colonoscopy in Patients With
450 Gut, 1991,32,450-451 Septicaemia after colonoscopy in patients with cirrhosis Gut: first published as 10.1136/gut.32.4.450 on 1 April 1991. Downloaded from j R Thornton, M S Losowsky Abstract PATIENT 2 Two patients with ulcerative colitis and In 1987, a 34 year old man underwent routine chronic active hepatitis with cirrhosis, who colonoscopy because ofhis ulcerative colitis of 12 developed Gram negative septicaemia after years' duration. Twenty three years earlier a colonoscopy are described. These and two liver biopsy had shown that he had chronic similar reported cases indicate that giving active hepatitis and cirrhosis. Hepatitis B prophylactic antibiotics to patients with cir- markers were negative. In 1983 he developed rhosis undergoing colonoscopy should be con- ascites and had remained on spironolactone since sidered, particularly when the cirrhosis is then. advanced. At the time ofhis colonoscopy he claimed that he felt reasonably well and was continuing to work. However, he had a moderate amount of Prophylactic antibiotics have been advised for ascites. His medication was: prednisolone 5 mg patients undergoing colonoscopy who have daily, spironolactone 200 mg daily, and sul- valvular heart disease, cardiac prostheses, severe phasalazine 1 g twice daily. Preoperative blood immunodepression, or hepatic cirrhosis with tests were: bilirubin 53 ,umol/1, alanine amino- ascites.' The last of these recommendations is transferase 38 IU/, alkaline phosphatase 206 IU/ based on a single case report in which it was not 1, albumin 28 g/l, prothrombin time 16 seconds certain that colonoscopy was responsible for the (control 14 seconds). infection, as hepatic angiography was performed After bowel preparation with three litres of the day before peritonitis developed.' We were Golytely, colonoscopy to the caecum was per- unaware of this case but our recent experience formed.