Poliomyelriis in 1954 A
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Some Notes on the Malayan Law of Negligence
Cleveland State Law Review Volume 9 Issue 3 Psychiatry and Law (A Symposium) Article 10 1960 Some Notes on the Malayan Law of Negligence A. E. S. Tay J. H. M. Heah Follow this and additional works at: https://engagedscholarship.csuohio.edu/clevstlrev Part of the Comparative and Foreign Law Commons, and the Torts Commons How does access to this work benefit ou?y Let us know! Recommended Citation A. E. S. Tay & J. H. M. Heah, Some Notes on the Malayan Law of Negligence, 9 Clev.-Marshall L. Rev. 490 (1960) This Article is brought to you for free and open access by the Journals at EngagedScholarship@CSU. It has been accepted for inclusion in Cleveland State Law Review by an authorized editor of EngagedScholarship@CSU. For more information, please contact [email protected]. Some Notes on the Malayan Law of Negligence A. E. S. Tay* and J. H. M. Heah** T HE TERM "MALAYA" COVERS what are now two distinct political units: the fully independent Federation of Malaya and the semi-independent State of Singapore, which have emerged from a tangle of British settlements and colonies and British-protected Malay states. The State of Singapore has sprung from the Crown Colony of Singapore, which between 1826 and 1946 formed part of the larger Crown Colony of the Straits Settle- ments. The two remaining Straits settlements-Penang (includ- ing Province Wellesley) and Malacca-together with nine Malay states' have become the Federation of Malaya. Although Penang and Malacca, as British territories, have a very different legal history from that of the Malay states, their welding together into a political unit has been followed by legislation giving statu- tory foundation for the application of the English common law throughout the Federation; the historical differences, then, have lost their practical point. -

The State of Food and Agriculture, 1954
iilliiill 111111111111 1111 .11 ii111111 11 iiiiiill 11111111 11111111111 1111 11 Review and Outioo 11 11 11 11 11 1111 11111 11 1111111 111111111 uu ' 1111111111i 1111111111111 111 III pill!! 1111 111111111 11 HO 11 11 11111111 dK¿,1tur u,11 11 11 11 1111 11 1111111 YL AN[ fiULTi -STICS-1953 _RT I- PRODUCTION Part I provides basic statistics on world agricultural production.It gives authoritative infor- mation on landuse, agricultural population, crops, livestock numbers and products, food supplies and their utilization, and on commercial fertilizers, pesticides, and agricultural machinery.It also includes the more important series of agricultural commodity prices in many countries, as well asindex numbers of prices received and paidby farmers, and of agricultural production. PART II- TRADE The second partisa basic reference work on world trade in agricultural products and gives statistics of the imports and exports of the major agricultural commodities.It includes regional and world totals, computed from official and unofficial information.For some major commodities, data are given by trade season aswell as by calendar year. This two-volume yearbookisa valuable reference work for importers, exporters, and com- mercial houses, as well as official bodies concerned with food and agriculture.Itis available from any bookseller, or from any of the FAO sales agents listed on the back cover of this publication. Price :Each part $3.50 or 17s.6d FAO STATISTICAP, PUBLIC L'IONS Monthly Bulletin of Agricultural Economics and Statistics Single copy $0.50, 2s.6d. Annual subscription $5.00, 25s. This bulletin gives statistics of production, trade and prices based on information available on the 25th of the month preceding that of issue.Each number contains one or two articles on mat- ters of current interest in the field of agricultural economics, and a section of commodity notes. -
Copy of Age Eligibility from 6 April 10
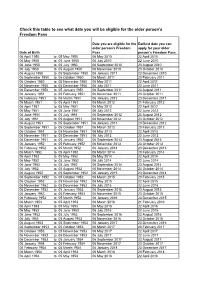
Check this table to see what date you will be eligible for the older person's Freedom Pass Date you are eligible for the Earliest date you can older person's Freedom apply for your older Date of Birth Pass person's Freedom Pass 06 April 1950 to 05 May 1950 06 May 2010 22 April 2010 06 May 1950 to 05 June 1950 06 July 2010 22 June 2010 06 June 1950 to 05 July 1950 06 September 2010 23 August 2010 06 July 1950 to 05 August 1950 06 November 2010 23 October 2010 06 August 1950 to 05 September 1950 06 January 2011 23 December 2010 06 September 1950 to 05 October 1950 06 March 2011 20 February 2011 06 October 1950 to 05 November 1950 06 May 2011 22 April 2011 06 November 1950 to 05 December 1950 06 July 2011 22 June 2011 06 December 1950 to 05 January 1951 06 September 2011 23 August 2011 06 January 1951 to 05 February 1951 06 November 2011 23 October 2011 06 February 1951 to 05 March 1951 06 January 2012 23 December 2011 06 March 1951 to 05 April 1951 06 March 2012 21 February 2012 06 April 1951 to 05 May 1951 06 May 2012 22 April 2012 06 May 1951 to 05 June 1951 06 July 2012 22 June 2012 06 June 1951 to 05 July 1951 06 September 2012 23 August 2012 06 July 1951 to 05 August 1951 06 November 2012 23 October 2012 06 August 1951 to 05 September 1951 06 January 2013 23 December 2012 06 September 1951 to 05 October 1951 06 March 2013 20 February 2013 06 October 1951 to 05 November 1951 06 May 2013 22 April 2013 06 November 1951 to 05 December 1951 06 July 2013 22 June 2013 06 December 1951 to 05 January 1952 06 September 2013 23 August 2013 06 -

Country Coding Units
INSTITUTE Country Coding Units v11.1 - March 2021 Copyright © University of Gothenburg, V-Dem Institute All rights reserved Suggested citation: Coppedge, Michael, John Gerring, Carl Henrik Knutsen, Staffan I. Lindberg, Jan Teorell, and Lisa Gastaldi. 2021. ”V-Dem Country Coding Units v11.1” Varieties of Democracy (V-Dem) Project. Funders: We are very grateful for our funders’ support over the years, which has made this ven- ture possible. To learn more about our funders, please visit: https://www.v-dem.net/en/about/ funders/ For questions: [email protected] 1 Contents Suggested citation: . .1 1 Notes 7 1.1 ”Country” . .7 2 Africa 9 2.1 Central Africa . .9 2.1.1 Cameroon (108) . .9 2.1.2 Central African Republic (71) . .9 2.1.3 Chad (109) . .9 2.1.4 Democratic Republic of the Congo (111) . .9 2.1.5 Equatorial Guinea (160) . .9 2.1.6 Gabon (116) . .9 2.1.7 Republic of the Congo (112) . 10 2.1.8 Sao Tome and Principe (196) . 10 2.2 East/Horn of Africa . 10 2.2.1 Burundi (69) . 10 2.2.2 Comoros (153) . 10 2.2.3 Djibouti (113) . 10 2.2.4 Eritrea (115) . 10 2.2.5 Ethiopia (38) . 10 2.2.6 Kenya (40) . 11 2.2.7 Malawi (87) . 11 2.2.8 Mauritius (180) . 11 2.2.9 Rwanda (129) . 11 2.2.10 Seychelles (199) . 11 2.2.11 Somalia (130) . 11 2.2.12 Somaliland (139) . 11 2.2.13 South Sudan (32) . 11 2.2.14 Sudan (33) . -

Economic Development of Malaya
ECONOMIC DEVELOPMENT OF MALAYA The Institute of Asian Economic Affairs, MaraJ'a Shingap5ru no Keizai Kaihatsu (Economic Development in the Federation of Malaya and the State of Singapore), Tokyo, 1962, 348 pp. This book is the result of a joint study conducted by the follovving research group headed by Hiroshi Matsuo under the auspices of the Institute of Asian Economic Affairs : Shigeo Shimizu~awa, Assistant Professor of Meiji University (Chapter I) ; Hiroshi Matsuo, Professor of Meiji Utriversify (Chapters 11 & IV) ; Kikuo Yamaoka, Professor of Chiba University (Chapter 111) ; Yasuaki Yoshimura, chief of the research department of the~ C;verseas Mineral Resources Development Company (Chapter V) ; and Yasushi Oiwa, Yawata lron and Steel Co., Ltd. (Chapter VI). This comprehensive study examines the problems of economic develop- ment of the Federation of Malaya and the State pf Singapore based on data obtained through on-the-spot suiveys ofthe two countries. The study analyses the economic structure of the two countries, and other matters related to their economic development. This study does not purport to be the kind of theoretical analysis which makes use of the models and hypotheses of modern economics. The writers have discussed the following points : recognition of the peculiar characteristics of Malayan politics, economy and society ; study - of the historical process of economic developinent ; outline and character- istics of economic development plan ; examination of problems during the process of economic development ; role of foreign investments ; and status and future prospects of development 6f mineral resources. Economic development in any nation should be built on political, economic and social foundations. -

Issn 1198-6727
ISSN 1198-6727 FISHERIES CATCH RECONSTRUCTIONS: ISLANDS, PART IV Fisheries Centre Research Reports 2014 Volume 22 Number 2 ISSN 1198-6727 Fisheries Centre Research Reports 2014 VOLUME 22 NUMBER 2 FISHERIES CATCH RECONSTRUCTIONS: ISLANDS, PART IV Fisheries Centre, University of British Columbia, Canada Edited by Kyrstn Zylich, Dirk Zeller, Melanie Ang and Daniel Pauly Fisheries Centre Research Reports 22(2) 157 pages © published 2014 by The Fisheries Centre, University of British Columbia 2202 Main Mall Vancouver, B.C., Canada, V6T 1Z4 ISSN 1198-6727 Fisheries Centre Research Reports 22(2) 2014 Edited by Kyrstn Zylich, Dirk Zeller, Melanie Ang and Daniel Pauly CONTENT Preface i Reconstruction of total marine fisheries catches for Anguilla (1950 - 2010) 1 Robin Ramdeen, Kyrstn Zylich, and Dirk Zeller Reconstruction of total marine fisheries catches for the British Virgin Islands (1950 - 2010) 9 Robin Ramdeen, Sarah Harper, Kyrstn Zylich, and Dirk Zeller Reconstruction of domestic fisheries catches in the Chagos Archipelago: 1950 - 2010 17 Dirk Zeller and Daniel Pauly Reconstruction of total marine fisheries catches for Cuba (1950 - 2010) 25 Andrea Au, Kyrstn Zylich, and Dirk Zeller Reconstruction of total marine fisheries catches for Dominica (1950 - 2010) 33 Robin Ramdeen, Sarah Harper, and Dirk Zeller Reconstruction of total marine fisheries catches for the Dominican Republic (1950 - 2010) 43 Liesbeth van der Meer, Robin Ramdeen, Kyrstn Zylich, and Dirk Zeller The catch of living marine resources around Greenland from 1950 t0 2010 55 -

1052 Public Law 761 CHAPTER 1206 Be It Enacted Hy the Senate And
1052 PUBLIC LAW 761-SEPT. 1, 1954 [68 ST AT. Public Law 761 CHAPTER 1206 September 1, 1954 AN ACT [H. R. 9366] To amend the Social Security Act and the Internal Revenue Code so as to extend coverage under the old-age and survivors insurance program, increase the benefits payable thereunder, preserve the insurance rights of disabled indi viduals, and increase the amount of earnings permitted without loss of bene fits, and for other purposes. Be it enacted hy the Senate and House of Representatives of the S o c i al Security Amendments of United States of America in Congress assembled^ That this Act may 1954. be cited as the "Social Security Amendments of 1954". TITLE I—AMENDMENTS TO TITLE II OF THE SOCIAL SECURITY ACT EXTENSION OF COVERAGE DOMESTIC SERVICE, SERVICE NOT IN COURSE OF EMPLOYER'S BUSINESS, AND AGRICULTURAL LABOR 64 Stat, 493. 42 use 409. SEC. 101. (a) (1) Paragraph (2) of section 209 (g) of the Social Security Act is amended to read as follows: "(2) Cash remuneration paid by an employer in any calendar quarter to an employee for domestic service in a private home of the employer, if the cash remuneration paid in such quarter by the employer to the employee for such service is less than $50. As used in this paragraph, the term 'domestic service in a private home of the employer' does not include service described in section 42 use 410. 210 (f) (5) ;". (2) Section 209 (g) of such Act is amended by adding at the end thereof the following new paragraph: "(3) Cash remuneration paid by an employer in any calendar quarter to an employee for service not in the course of the employer's trade or business, if the cash remuneration paid in such quarter by the employer to the employee for such service is less than $50. -

AUGUST 1954 Rar
AUGUST 1954 rar U. S. DEPARTMENT OF COMMERCE OFFICE OF BUSINESS ECONOMICS OF CURRENT •DEPAKTM/ECVr OF CQM'M.-EKCIK FIELD/SERVICE • - Altvu-qwwitje, N. Max.. No. 8 204 S. 10th St. 1031 S. Rn>*d«r«? AUGUST 1951 Atlanta 5,-Ga. 50 Sfcveatij £t. N18, 229 Fed-e Boutin *>, Maw. ' Miami 32, FU. U. S. Post Offic» *ai4 36 3NE. Fu-f Cowrtlionac Bldg, Mitmeapoli^ 2, Mia Buffalo 3. N. Y. 607 Marc PAGE N*w Orbans 12. La. o« 4, S. C. 385 St. Charlea A< , THE BUSINESS SITUATION .......... 1 ant Jasper N«w York 13, W. Y. National Income and Product . * . HS Wyo. 346 Broad«r 307 Federal Oflie* BM«, A Review of the Second Quarter ..... 2 ia I, Pa. 1015 Chcxttnu Chicago 1, 111, Foreign Countries Get $2.5 Billion 226 W. Jacks**) BUkC from U. S. Military Outlays .."..•..-.-.- 7 Pisoenix, Am^ Gmcirmati 2, Ohio 137 N, Sw^d 422 U. S, Post Ofl6i*9 Pitt«bur«h 22, l'^. 107 SJist * * * elajkL 11, Ohio Portland 4, Ort»#. 1100 Ch#at«r A\Y«, SPECIAL ARTICLES 520 SW. Miwis. as 2, Tex. iUno, Nar, State Income Payments in 1953 ....... 9 1 1 14 CIJ^HBUNW -5t. Farm Income Dearer 2, Colo, Richmond., V*. 142 New Custom 400£a>*i MamST-., and Gross National Product * . IS Detroit 2-6, Mi A, St. Loui» 1. M,». 2SO W, F. 1114 Market ••*(:. Salt Lake City I, Uta!r 109 W. Second 5 1. So.. MONTHLY BUSINESS STATISTICS , . S-l to SHW 'Ston, I'ex. S-a« l''r<uiei*xj 11, CflSff 430 Lanwr^t. -

An Analysis of the Underlying Factors That Affected Malaysia-Singapore Relations During the Mahathir Era: Discords and Continuity
An Analysis of the Underlying Factors That Affected Malaysia-Singapore Relations During the Mahathir Era: Discords and Continuity Rusdi Omar Thesis submitted for the degree of Doctor of Philosophy in the Discipline of Politics and International Studies School of History and Politics Faculty of Humanities and Social Sciences The University of Adelaide May 2014 TABLE OF CONTENTS TITLE PAGE TABLE OF CONTENTS i ABSTRACT v DECLARATION vi ACKNOWLEDGEMENTS vii ABBREVIATIONS/ACRONYMS ix GLOSSARY xii 1 INTRODUCTION 1 1.1. Introductory Background 1 1.2. Statement of the Problem 3 1.3. Research Aims and Objectives 5 1.4. Scope and Limitation 6 1.5. Literature Review 7 1.6. Theoretical/ Conceptual Framework 17 1.7. Research Methodology 25 1.8. Significance of Study 26 1.9. Thesis Organization 27 2 HISTORICAL BACKGROUND OF MALAYSIA-SINGAPORE RELATIONS 30 2.1. Introduction 30 2.2. The Historical Background of Malaysia 32 2.3. The Historical Background of Singapore 34 2.4. The Period of British Colonial Rule 38 i 2.4.1. Malayan Union 40 2.4.2. Federation of Malaya 43 2.4.3. Independence for Malaya 45 2.4.4. Autonomy for Singapore 48 2.5. Singapore’s Inclusion in the Malaysian Federation (1963-1965) 51 2.6. The Period after Singapore’s Separation from Malaysia 60 2.6.1. Tunku Abdul Rahman’s Era 63 2.6.2 Tun Abdul Razak’s Era 68 2.6.3. Tun Hussein Onn’s Era 76 2.7. Conclusion 81 3 CONTENTIOUS ISSUES IN MALAYSIA-SINGAPORE RELATIONS 83 3.1. Introduction to the Issues Affecting Relations Between Malaysia and Singapore 83 3.2. -

Colony of North Borneo Annual Report
«r; • c- 2.^.0- COLONIAL REPORTS North Borneo .-•■■'■ . ■ - - ■ LONDON HER MAJESTY’S STATIONERY OFFICE 1956 1 i Designed, printed and bound by the Technical Staff of the Government Printing Department, North Borneo, 1956 Contents Page PART i Chapter 1 General Review ... ... ... ... 1 PART II Chapter 1 Population ... ... ... ... 9 2 Occupation, Wages and Labour Organisation ... 14 3 Public Finance and Taxation ... ... 20 4 Currency and Banking ... ... ... 27 5 Commerce ... ... ... ... 28 6 Production Land Utilisation and Ownership ... ... 34 Agriculture ... ... ... ... 39 Animal Husbandry ... ... ... 46 Drainage and Irrigation ... .. 48 Forests ... ... ... ... 49 Fisheries ... ... ... ... 57 7 Social Services Education ... ... ... ... 60 Public Health ... ... ... ... 68 Housing and Town Planning ... 74 Social Welfare ... ... ... ... 77 8 Legislation ... ... ... ... 84 9 Justice, Police and Prisons Justice ... ... ... ... 86 Police ... ... ... ... 87 Prisons ... ... ... ... 93 10 Public Utilities and Public Works Public Works Department ... ... 96 Electricity ... ... ... ... 98 Water ... ... ... ... 99 11 Communications Harbours and Shipping ... ... 102 Railways ... ... ... ... 106 Roads ... ... ... ... 109 Road Transport ... ... Ill Air Communications ... ... ... Ill Posts ... ... ... ... 114 Telecommunications ... ... ... 114 12 Government Information Services, Broadcasting, Press and Films ... ... ... 116 13 Geology ... ... ... ... 122 PART III Chapter 1 Geography and Climate ... ... ... 129 2 History History ... ... ... ... 134 List -

Download Download
Downloaded from the Humanities Digital Library http://www.humanities-digital-library.org Open Access books made available by the School of Advanced Study, University of London Press ***** Publication details: Administering the Empire, 1801-1968: A Guide to the Records of the Colonial Office in the National Archives of the UK by Mandy Banton http://humanities-digital-library.org/index.php/hdl/catalog/book/administering-the- empire-1801-1968 DOI: 10.14296/0920.9781912702787 ***** This edition published 2020 by UNIVERSITY OF LONDON PRESS SCHOOL OF ADVANCED STUDY INSTITUTE OF HISTORICAL RESEARCH Senate House, Malet Street, London WC1E 7HU, United Kingdom ISBN 978-1-912702-78-7 (PDF edition) This work is published under a Creative Commons Attribution-NonCommercial- NoDerivatives 4.0 International License. More information regarding CC licenses is available at https://creativecommons.org/licenses A Guide to the Records of the Colonial Office in The National Archives of the UK Archives National The Office in of the Colonial to the Records A Guide 1801–1968Administering the Empire, Administering the Empire, 1801-1968 is an indispensable introduction to British colonial rule during Administering the Empire, 1801–1968 the nineteenth and twentieth centuries. It provides an essential guide to the records of the British Colonial Office, and those of other departments responsible for colonial administration, which are A Guide to the Records of the Colonial Office in now held in The National Archives of the United Kingdom. The National Archives of the UK As a user-friendly archival guide, Administering the Empire explains the organisation of these records, the information they provide, and how best to explore them using contemporary finding aids. -
Subscription Libraries, Literacy & Acculturation in the Colonies Of
Florida State University Libraries Electronic Theses, Treatises and Dissertations The Graduate School 2008 Empire of the Mind: Subscription Libraries, Literacy & Acculturation in the Colonies of the British Empire Sterling Joseph Coleman Follow this and additional works at the FSU Digital Library. For more information, please contact [email protected] FLORIDA STATE UNIVERSITY COLLEGE OF ARTS AND SCIENCES EMPIRE OF THE MIND: SUBSCRIPTION LIBRARIES, LITERACY & ACCULTURATION IN THE COLONIES OF THE BRITISH EMPIRE By STERLING JOSEPH COLEMAN, JR. A Dissertation submitted to the Department of History in partial fulfillment of the requirements for the degree of Doctor of Philosophy Degree Awarded: Fall Semester, 2008 Copyright © 2008 Sterling Joseph Coleman, Jr. All Rights Reserved The members of the Committee approve the Dissertation of Sterling Joseph Coleman, Jr. defended on October 27, 2008. _____________________________ Charles Upchurch Professor Directing Dissertation _____________________________ Wayne Wiegand Outside Committee Member _____________________________ Peter Garretson Committee Member _____________________________ Jonathan Grant Committee Member _____________________________ Nathan Stoltzfus Committee Member The Office of Graduate Studies has verified and approved the above named committee members. ii ACKNOWLEDGMENTS The author would like to thank his father, Sterling Joseph Coleman, Sr. for giving him the strength of character to see this project through, his mother, Rosie Coleman, for granting him the knowledge and wisdom necessary