Type of Article
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ipsilateral Subclavian Steal in Association with Aberrant Origin of the Left Vertebral Artery from the Aortic Arch
411 Ipsilateral Subclavian Steal in Association with Aberrant Origin of the Left Vertebral Artery from the Aortic Arch John Holder1 Five cases are reported of left subclavian steal syndrome associated with anomalous Eugene F. Binet2 origin of the left vertebral artery from the aortic arch. In all five instances blood flow at Bernard Thompson3 the origin of the left vertebral artery was in an antegrade direction contrary to that usually reported in this condition. The distal subclavian artery was supplied via an extensive collateral network of vessels connecting the vertebral artery to the thyro cervical trunk. If a significant stenosis or occlusion is present within the left subc lavi an artery proximal to the origin of the left vertebral artery, the direction of the bl ood fl ow within the vertebral artery will reverse toward the parent vessel (retrograde flow). This phenomenon occurs when a negative pressure gradient of 20-40 torr exists between the vertebral-basilar artery junction and th e vertebral-subc lavian artery junction [1-3]. We describe five cases of subclavian steal confirmed by angiography where a significant stenosis or occlusion of the left subclavian artery was demonstrated in association with anomalous origin of th e left vertebral artery directly from the aortic arch. In all five cases blood flow at the origin of the left vertebral artery was in an antegrade direction contrary to that more commonly reported in the subclavian steal syndrome. Materials and Methods The five patients were all 44- 58-year-old men. Three sought medical attention for symptoms specificall y related to th e left arm . -

ANGIOGRAPHY of the UPPER EXTREMITY Printed in the Netherlands by Koninklijke Drukkerij G.J.Thieme Bv, Nijmegen ANGIOGRAPHY of the UPPER EXTREMITY
1 f - h-' ^^ ANGIOGRAPHY OF THE UPPER EXTREMITY Printed in The Netherlands by Koninklijke drukkerij G.J.Thieme bv, Nijmegen ANGIOGRAPHY OF THE UPPER EXTREMITY PROEFSCHRIFT ter verkrijging van de graad van Doctor in de Geneeskunde aan de Rijksuniversiteit te Leiden, op gezag van de Rector Magni- ficus Dr. A. A. H. Kassenaar, Hoogleraar in de faculteit der Geneeskunde, volgens besluit van het college van dekanen te verdedigen op donderdag 6 mei 1982 te klokke 15.15 uur DOOR BLAGOJA K. JANEVSKI geborcn 8 februari 1934 te Gradsko, Joegoslavie MARTINUS NIJHOFF PUBLISHERS THE HAGUE - BOSTON - LONDON 1982 PROMOTOR: Prof. Dr. A. E. van Voorthuisen REPERENTEN: Prof. Dr. J. M. F. LandLandsmees r 1 Prof. Dr. J. L. Terpstra ! I Copyright © 1982 by Martinus Nijhoff Publishers, The Hague All rights reserved. No part of this publication may be repro- duced, stored in a retrieval system, or transmitted in any form or by any means, mechanical, photocopying, recording, or otherwise, without the prior written permission of the pub- lishers, Martinus Nijhoff Publishers,P.O. Box 566,2501 CN The Hague, The Netherlands if ••»• 7b w^ wife Charlotte To Lucienne, Lidia and Dejan h {, ,;T1 ii-"*1 ™ ffiffp"!»3^>»'*!W^iyJiMBiaMMrar^ ACKNOWLEDGEMENTS This thesis was produced in the Department of Radiology, Sirit Annadal Hospital, Maastricht. i Case material: Prof. Dr. H. A. J. Lemmens, surgeon. Technical assistence: Miss J. Crijns, Mrs. A. Rousie-Panis, Miss A. Mordant and Miss H. Nelissen. Secretarial help: Mrs. M. Finders-Velraad and Miss Y. Bessems. Photography: Mr. C. Evers. Graphical illustrations: Mr. C. Voskamp. Correction English text: Dr. -

Vessels and Circulation
CARDIOVASCULAR SYSTEM OUTLINE 23.1 Anatomy of Blood Vessels 684 23.1a Blood Vessel Tunics 684 23.1b Arteries 685 23.1c Capillaries 688 23 23.1d Veins 689 23.2 Blood Pressure 691 23.3 Systemic Circulation 692 Vessels and 23.3a General Arterial Flow Out of the Heart 693 23.3b General Venous Return to the Heart 693 23.3c Blood Flow Through the Head and Neck 693 23.3d Blood Flow Through the Thoracic and Abdominal Walls 697 23.3e Blood Flow Through the Thoracic Organs 700 Circulation 23.3f Blood Flow Through the Gastrointestinal Tract 701 23.3g Blood Flow Through the Posterior Abdominal Organs, Pelvis, and Perineum 705 23.3h Blood Flow Through the Upper Limb 705 23.3i Blood Flow Through the Lower Limb 709 23.4 Pulmonary Circulation 712 23.5 Review of Heart, Systemic, and Pulmonary Circulation 714 23.6 Aging and the Cardiovascular System 715 23.7 Blood Vessel Development 716 23.7a Artery Development 716 23.7b Vein Development 717 23.7c Comparison of Fetal and Postnatal Circulation 718 MODULE 9: CARDIOVASCULAR SYSTEM mck78097_ch23_683-723.indd 683 2/14/11 4:31 PM 684 Chapter Twenty-Three Vessels and Circulation lood vessels are analogous to highways—they are an efficient larger as they merge and come closer to the heart. The site where B mode of transport for oxygen, carbon dioxide, nutrients, hor- two or more arteries (or two or more veins) converge to supply the mones, and waste products to and from body tissues. The heart is same body region is called an anastomosis (ă-nas ′tō -mō′ sis; pl., the mechanical pump that propels the blood through the vessels. -

The Variations of the Subclavian Artery and Its Branches Ahmet H
Okajimas Folia Anat. Jpn., 76(5): 255-262, December, 1999 The Variations of the Subclavian Artery and Its Branches By Ahmet H. YUCEL, Emine KIZILKANAT and CengizO. OZDEMIR Department of Anatomy, Faculty of Medicine, Cukurova University, 01330 Balcali, Adana Turkey -Received for Publication, June 19,1999- Key Words: Subclavian artery, Vertebral artery, Arterial variation Summary: This study reports important variations in branches of the subclavian artery in a singular cadaver. The origin of the left vertebral artery was from the aortic arch. On the right side, no thyrocervical trunk was found. The two branches which normally originate from the thyrocervical trunk had a different origin. The transverse cervical artery arose directly from the subclavian artery and suprascapular artery originated from the internal thoracic artery. This variation provides a short route for posterior scapular anastomoses. An awareness of this rare variation is important because this area is used for diagnostic and surgical procedures. The subclavian artery, the main artery of the The variations of the subclavian artery and its upper extremity, also gives off the branches which branches have a great importance both in blood supply the neck region. The right subclavian arises vessels surgery and in angiographic investigations. from the brachiocephalic trunk, the left from the aortic arch. Because of this, the first part of the right and left subclavian arteries differs both in the Subjects origin and length. The branches of the subclavian artery are vertebral artery, internal thoracic artery, This work is based on a dissection carried out in thyrocervical trunk, costocervical trunk and dorsal the Department of Anatomy in the Faculty of scapular artery. -

Head & Neck Muscle Table
Robert Frysztak, PhD. Structure of the Human Body Loyola University Chicago Stritch School of Medicine HEAD‐NECK MUSCLE TABLE PROXIMAL ATTACHMENT DISTAL ATTACHMENT MUSCLE INNERVATION MAIN ACTIONS BLOOD SUPPLY MUSCLE GROUP (ORIGIN) (INSERTION) Anterior floor of orbit lateral to Oculomotor nerve (CN III), inferior Abducts, elevates, and laterally Inferior oblique Lateral sclera deep to lateral rectus Ophthalmic artery Extra‐ocular nasolacrimal canal division rotates eyeball Inferior aspect of eyeball, posterior to Oculomotor nerve (CN III), inferior Depresses, adducts, and laterally Inferior rectus Common tendinous ring Ophthalmic artery Extra‐ocular corneoscleral junction division rotates eyeball Lateral aspect of eyeball, posterior to Lateral rectus Common tendinous ring Abducent nerve (CN VI) Abducts eyeball Ophthalmic artery Extra‐ocular corneoscleral junction Medial aspect of eyeball, posterior to Oculomotor nerve (CN III), inferior Medial rectus Common tendinous ring Adducts eyeball Ophthalmic artery Extra‐ocular corneoscleral junction division Passes through trochlea, attaches to Body of sphenoid (above optic foramen), Abducts, depresses, and medially Superior oblique superior sclera between superior and Trochlear nerve (CN IV) Ophthalmic artery Extra‐ocular medial to origin of superior rectus rotates eyeball lateral recti Superior aspect of eyeball, posterior to Oculomotor nerve (CN III), superior Elevates, adducts, and medially Superior rectus Common tendinous ring Ophthalmic artery Extra‐ocular the corneoscleral junction division -
The Vertebral Artery in the Vascular Lab: What Does It Mean?
The Vertebral Artery in the Vascular Lab: What Does It Mean? Caron Rockman MD Frances and Joseph Ritroto Professor of Surgery Program Director, Vascular Surgery New York University Langone Medical Center Disclosures •None Division of Vascular and Endovascular Surgery Subclavian Steal Occlusion of proximal Subclavian Art Vertebral artery supplies retrograde flow Posterior brain receives decreased flow 55 years + Men > Women more than 2:1 LSA affected 3x more than RSA Division of Vascular and Endovascular Surgery Subclavian Steal Causes: - Arteriosclerosis of subclavian artery (>95% cases) - Embolism - Takayasu’s Arteritis -Dissecting Aneurysm Risk Factors: (similar to CAD) -Smoking -Hypertension -Hyperlipidemia -Hypertension Division of Vascular and Endovascular Surgery Symptoms of Subclavian Steal Vertebrobasilar Insufficiency (posterior circulation symptoms) Light headedness or dizziness Ataxia or Vertigo Visual Disturbance Headache Syncope Confusion Division of Vascular and Endovascular Surgery Symptoms of Subclavian Steal Subclavian Insufficiency Arm weakness, coldness Numbness or “tingling” Arm Claudication with exercise Symptoms can be exacerbated with: Vigorous exercise Sudden turning of head to affected side Division of Vascular and Endovascular Surgery Signs of Subclavian Steal Diminished pulses (radial/ulnar) Discrepant blood pressures in upper extremities (>20mmHg) (Pitfall with bilateral disease) Subclavian Bruit 7 Division of Vascular and Endovascular Surgery Subclavian steal on Duplex Exam Incomplete steal •Striking deceleration of velocity in mid or late systole •High grade stenosis of subclavian rather than occlusion Complete Steal •Complete reversal of flow within the vertebral artery Division of Vascular and Endovascular Surgery Vertebral Retrograde Flow • Reversal of flow in the vertebral artery is a common finding identified on cerebrovascular duplex ultrasound. • The clinical significance and natural history of patients presenting with this finding, however, is poorly understood. -

Complications Associated with Clavicular Fracture
NOR200061.qxd 9/11/09 1:23 PM Page 217 Complications Associated With Clavicular Fracture George Mouzopoulos ▼ Emmanuil Morakis ▼ Michalis Stamatakos ▼ Mathaios Tzurbakis The objective of our literature review was to inform or- subclavian vein, due to its stable connection with the thopaedic nurses about the complications of clavicular frac- clavicle via the cervical fascia, can also be subjected to ture, which are easily misdiagnosed. For this purpose, we injuries (Casbas et al., 2005). Damage to the internal searched MEDLINE (1965–2005) using the key words clavicle, jugular vein, the suprascapular artery, the axillary, and fracture, and complications. Fractures of the clavicle are usu- carotid artery after a clavicular fracture has also been ally thought to be easily managed by symptomatic treatment reported (Katras et al., 2001). About 50% of injuries to the subclavian arteries are in a broad arm sling. However, it is well recognized that not due to fractures of the clavicle because the proximal all clavicular fractures have a good outcome. Displaced or part is dislocated superiorly by the sternocleidomas- comminuted clavicle fractures are associated with complica- toid, causing damage to the vessel (Sodhi, Arora, & tions such as subclavian vessels injury, hemopneumothorax, Khandelwal, 2007). If no injury happens during the ini- brachial plexus paresis, nonunion, malunion, posttraumatic tial displacement of the fractured part, then it is un- arthritis, refracture, and other complications related to os- likely to happen later, because the distal segment is dis- teosynthesis. Herein, we describe what the orthopaedic nurse placed downward and forward due to shoulder weight, should know about the complications of clavicular fractures. -

Dr. Neelesh Kanasker Original Research Paper Anatomy Dr.Preeti
Original Research Paper Volume - 11 | Issue - 04 | April - 2021 | PRINT ISSN No. 2249 - 555X | DOI : 10.36106/ijar Anatomy SURGICAL IMPORTANCE OF VARIABLE BRANCHING PATTERN OF THYROCERVICAL TRUNK IN NECK ROOT SURGERIES Dr. Neelesh Associate professor, Department of Anatomy, Dr. D. Y. Patil Medical College, Hospital Kanasker and Research Center, Dr.D.Y.Patil Vidyapeeth , Pimpri Pune. Professor, Department of Anatomy, Dr. D. Y. Patil Medical College, Hospital and Dr.Preeti Sonje* Research Center, Dr.D.Y.Patil Vidyapeeth , Pimpri Pune. *Corresponding Author Dr. P. Professor and Director Academics, Department of Anatomy, Dr. D. Y. Patil Medical Vatsalaswamy College, Hospital and Research Center, Dr.D.Y.Patil Vidyapeeth , Pimpri Pune. ABSTRACT Objectives: Variations in the arteries of human body are important clinically as well as anatomically. Accurate knowledge and understanding of anomalous variations in the origin and course of arteries have serious implications in angiographic and surgical procedures hence it is of great importance to be aware of such possibilities of variations. Background and Results: Thyrocervical Trunk is short wide vessel arising from rst part of subclavian artery and divides into its three terminal branches i.e. Suprascapular, Inferior Thyroid and Transverse cervical artery. 30 formalin xed cadavers were dissected to study variations in Thyrocervical Trunk and its branches if any. Conclusion: Awareness of variations in the origin and branching pattern is of utmost importance during Doppler scanning of blood vessels for clinical diagnosis and surgical management and to avoid major complications in head and neck surgeries. KEYWORDS : Thyrocervical Trunk, Anomalous variations, Doppler scanning, Head and neck surgeries. INTRODUCTION anterior muscle and then arches medially at the level of C7 vertebra Subclavian artery is the artery of upper limb, but is supplies a between the vertebral vessels behind and carotid sheath in front. -

Spontaneous Arteriovenous Malformations in the Cervical Area
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.33.3.303 on 1 June 1970. Downloaded from J. Neurol. Neurosurg. Psychiat., 1970, 33, 303-309 Spontaneous arteriovenous malformations in the cervical area J. GREENBERG, M.D. From the Department of Neurology, Episcopal Hospital, Philadelphia, Pennsylvania 19125, U.S.A. SUMMARY Four patients with spontaneous arteriovenous malformations of cervical vessels have been presented. The embryology of these vessels has been discussed in order to suggest an ex- planation for the apparent difference in the incidence of arteriovenous malformations involving the internal carotid artery and those involving either the vertebral or the external carotid arteries. A fifth case (S.T.) is presented as a probable iatrogenic arteriovenous fistula and is to be added to the steadily growing reports of this phenomenon. Trauma is the most common cause of arteriovenous had sustained a minor injury to the posterior aspect communications between the blood vessels in of the right ear. Routine skull films at the time did not the cervical area (Aronson, 1961). Iatrogenic reveal a fracture, and there was no evidence of local Protected by copyright. deep tissue injury noted. fistulae occurring after carotid or vertebral angio- On the present admission, a slight prominence of the graphy are being reported with regularity in the right retroauricular region was noted and a thrill and recent literature (Sutton, 1962). Spontaneous mal- bruit were present. The bruit could be obliterated by formations in this area also occur. Thus far, eight local pressure. cases have been reported involving the vertebral The neurological examination was within normal vessels (Norman, Schmidt, and Grow, 1950; limits. -

Axis Scientific Human Circulatory System 1/2 Life Size A-105864
Axis Scientific Human Circulatory System 1/2 Life Size A-105864 05. Superior Vena Cava 13. Ascending Aorta 21. Hepatic Vein 28. Celiac Trunk II. Lung 09. Pulmonary Trunk 19. Common III. Spleen Hepatic Artery 10. Pulmonary 15. Pulmonary Artery 17. Splenic Artery (Semilunar) Valve 20. Portal Vein 03. Left Atrium 18. Splenic Vein 01. Right Atrium 16. Pulmonary Vein 26. Superior 24. Superior 02. Right Ventricle Mesenteric Vein Mesenteric Artery 11. Supraventricular Crest 07. Interatrial Septum 22. Renal Artery 27. Inferior 14. Aortic (Semilunar) Valve Mesenteric Vein 08. Tricuspid (Right 23. Renal Vein 12. Mitral (Left Atrioventricular) Valve VI. Large Intestine Atrioventricular) Valve 29. Testicular / 30. Common Iliac Artery Ovarian Artery 32. Internal Iliac Artery 25. Inferior 31. External Iliac Artery Mesenteric Artery 33. Median Sacral Artery 41. Posterior Auricular Artery 57. Deep Palmar Arch 40. Occipital Artery 43. Superficial Temporal Artery 58. Dorsal Venous Arch 36. External Carotid Artery 42. Maxillary Artery 56. Superficial Palmar Arch 35. Internal Carotid Artery 44. Internal Jugular Vein 39. Facial Artery 45. External Jugular Vein 38. Lingual Artery and Vein 63. Deep Femoral Artery 34. Common Carotid Artery 37. Superior Thyroid Artery 62. Femoral Artery 48. Thyrocervical Trunk 49. Inferior Thyroid Artery 47. Subclavian Artery 69. Great Saphenous Vein 46. Subclavian Vein I. Heart 51. Thoracoacromial II. Lung Artery 64. Popliteal Artery 50. Axillary Artery 03. Left Atrium 01. Right Atrium 04. Left Ventricle 02. Right Ventricle 65. Posterior Tibial Artery 52. Brachial Artery 66. Anterior Tibial Artery 53. Deep Brachial VII. Descending Artery Aorta 70. Small Saphenous Vein IV. Liver 59. -
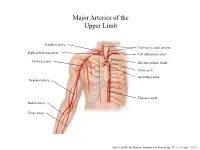
Major Arteries of the Upper Limb
Major Arteries of the Upper Limb Vertebral artery Common carotid arteries Right subclavian artery Left subclavian artery Axillary artery Brachiocephalic trunk Aortic arch Ascending aorta Brachial artery Thoracic aorta Radial artery Ulnar artery Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.23 Major Arteries of the Abdominal Region Renal artery Celiac trunk Abdominal aorta Superior mesenteric artery Gonadal artery Inferior mesenteric artery Common iliac artery Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.24 Common iliac artery Internal iliac artery Major Arteries of the External iliac artery Lower Limb Femoral artery Popliteal artery Anterior tibial artery Fibular artery Posterior tibial artery Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.25 Major Veins of the Upper Limb Internal jugular vein (left) Subclavian vein (right) External jugular vein (left) Axillary vein Brachiocephalic veins Cephalic vein Superior vena cava Brachial vein Basilic vein Median cubital vein Inferior vena cava Radial vein Ulnar vein Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.28 Major Veins of the Abdominal Cavity – Part 1 Hepatic veins Inferior vena cava Renal vein (left) Gonadal vein (left) Gonadal vein (right) Common iliac vein (left) Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.29 Major Veins of the Abdominal Cavity – Part 2 (Hepatic portal circulation) Hepatic portal vein Splenic vein Inferior mesenteric vein Superior mesenteric vein Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.29 Common iliac vein (left) Internal iliac vein Major Veins of the External iliac vein Lower Limb Great saphenous vein Femoral vein Popliteal vein Fibular vein Small saphenous vein Anterior tibial Posterior tibial vein vein Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.30 . -

Arterial Supply to the Rotator Cuff Muscles
Int. J. Morphol., 32(1):136-140, 2014. Arterial Supply to the Rotator Cuff Muscles Suministro Arterial de los Músculos del Manguito Rotador N. Naidoo*; L. Lazarus*; B. Z. De Gama*; N. O. Ajayi* & K. S. Satyapal* NAIDOO, N.; LAZARUS, L.; DE GAMA, B. Z.; AJAYI, N. O. & SATYAPAL, K. S. Arterial supply to the rotator cuff muscles.Int. J. Morphol., 32(1):136-140, 2014. SUMMARY: The arterial supply to the rotator cuff muscles is generally provided by the subscapular, circumflex scapular, posterior circumflex humeral and suprascapular arteries. This study involved the bilateral dissection of the scapulohumeral region of 31 adult and 19 fetal cadaveric specimens. The subscapularis muscle was supplied by the subscapular, suprascapular and circumflex scapular arteries. The supraspinatus and infraspinatus muscles were supplied by the suprascapular artery. The infraspinatus and teres minor muscles were found to be supplied by the circumflex scapular artery. In addition to the branches of these parent arteries, the rotator cuff muscles were found to be supplied by the dorsal scapular, lateral thoracic, thoracodorsal and posterior circumflex humeral arteries. The variations in the arterial supply to the rotator cuff muscles recorded in this study are unique and were not described in the literature reviewed. Due to the increased frequency of operative procedures in the scapulohumeral region, the knowledge of variations in the arterial supply to the rotator cuff muscles may be of practical importance to surgeons and radiologists. KEY WORDS: Arterial supply; Variations; Rotator cuff muscles; Parent arteries. INTRODUCTION (Abrassart et al.). In addition, the muscular parts of infraspinatus and teres minor muscles were supplied by the circumflex scapular artery while the tendinous parts of these The rotator cuff is a musculotendionous cuff formed muscles received branches from the posterior circumflex by the fusion of the tendons of four muscles – viz.