WHO Healthy Workplace Framework and Model: Background and Supporting Literature and Practices by Joan Burton
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

OCCUPATIONAL MEDICINE PROGRAM HANDBOOK October 2005
U.S. DEPARTMENT OF THE INTERIOR OFFICE OF OCCUPATIONAL HEALTH AND SAFETY OCCUPATIONAL MEDICINE PROGRAM HANDBOOK October 2005 This Occupational Medicine Program Handbook was prepared by the U.S. Department of the Interior’s Office of Occupational Health and Safety, in consultation with the U.S. Office of Personnel Management and the U.S. Public Health Service’s Federal Occupational Health service. This edition of the Handbook represents the continuing efforts of the contributing agencies to improve occupational health services for DOI employees. It reflects the comments and suggestions offered by users over the years since it was first introduced, and addresses the findings, concerns, and recommendations summarized in the final report of a program review completed in 1994 by representatives of the Uniformed Services University of the Health Sciences. That report, entitled “A Review of the Occupational Health Program of the United States Department of the Interior,” was prepared by Margaret A.K. Ryan, M.D., M.P.H., Gail Gullickson, M.D., M.P.H., W. Garry Rudolph, M.D., M.P.H., and Elizabeth Odell. The report led to the establishment of the Department’s Occupational Health Reinvention Working Group, composed of representatives from the DOI bureaus and operating divisions. The recommendations from the Reinvention Working Group final report, published in May of 1996, were addressed and are reflected in what became this Handbook. First published in 1997, the Handbook underwent a major update in July, 2000. This 2005 version of the Handbook incorporates the updates and enhancements that have been made in DOI policies and occupational medicine practice since the last edition. -
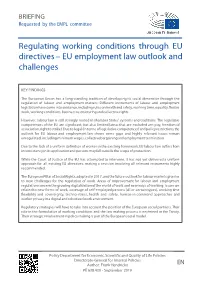
Regulating Working Conditions Through EU Directives – EU Employment Law Outlook and Challenges
BRIEFING Requested by the EMPL committee Regulating working conditions through EU directives – EU employment law outlook and challenges KEY FINDINGS The European Union has a long-standing tradition of developing its social dimension through the regulation of labour and employment matters. Different instruments of labour and employment legislation have come into existence, including rules on health and safety, working time, equality, flexible work, working conditions, business restructuring and collective rights. However, labour law is still strongly rooted in Member States’ systems and traditions. The legislative competences of the EU are significant, but also limited (areas that are excluded are: pay, freedom of association, right to strike). Due to legal (in terms of legislative competences) and policy restrictions, the outlook for EU labour and employment law shows some gaps and highly relevant issues remain unregulated, including minimum wages, collective bargaining and employment termination. Due to the lack of a uniform definition of worker in the existing framework, EU labour law suffers from inconsistency in its application and persons may fall outside the scope of protection. While the Court of Justice of the EU has attempted to intervene, it has not yet delivered a uniform approach for all existing EU directives, making a revision involving all relevant instruments highly recommended. The European Pillar of Social Rights, adopted in 2017, and the future outlook for labour markets give rise to new challenges for the regulation of work. Areas of improvement for labour and employment regulation concern the growing digitalization of the world of work and new ways of working. Issues are related to new forms of work, coverage of self-employed persons (all or certain types), working time flexibility and sovereignty, techno-stress, health and safety, human-in-command approaches and worker privacy in a digital and robotized work environment. -

Grim Consequences of Workplace Traditional Bullying and Cyberbullying by Way of Mediation: a Case of Service Sector of Pakistan Mehwish Iftikhar , Loo-See Beh
International Journal of Recent Technology and Engineering (IJRTE) ISSN: 2277-3878, Volume-8 Issue-2S, July 2019 Grim Consequences of Workplace Traditional Bullying and Cyberbullying by Way of Mediation: A Case of Service Sector of Pakistan Mehwish Iftikhar , Loo-See Beh healthy workforce. Therefore, a healthy workforce is the Abstract: Various studies have been conducted to measure precondition of productivity and economic development bullying incidence and prevalence in multiple organizational (World Health Organization (WHO), 2007). Employee settings based on a variety of methods and research design. health plays a significant role in the efficiency of any Nonetheless, these studies indicate that bullying is a devastating organization. Accordingly, providing a healthy work and crippling problem that should be addressed in relation to its environment should be the leading priority of each adverse effects and implications. This study identified several organization. Every work environment is considered healthy gaps in the literature when expanded specifically to the service sector of Pakistan, where the problem of bullying is prevalent. if harmful working conditions are absent and This research endeavored to fill in the aforementioned gaps by health-promoting activities and actions are present. The precisely focusing on organizational climate as a cause of maintenance of occupational health is costly (i.e., to promote bullying (based on frustration–aggression theory and social and maintain the highest degree of physical, mental, and interaction approach), technology in relation to cyberbullying, emotional well-being of workers) and the burden of such cost and effects on employee health. Hence, this study contributes to is increasing. The WHO Factsheet (2014) indicated that a the emergent discussion in identifying the debilitating outcomes majority of countries faced an economic loss of 4% to 6% of of bullying. -

Mobbing, Subjective Perception, Demographic Factors And
Cent Eur J Public Health 2020; 28 (Suppl): S57–S64 MOBBING, SUBJECTIVE PERCEPTION, DEMOGRAPHIC FACTORS AND PREVALENCE OF BURNOUT SYNDROME IN NURSES Šárka Vévodová, Jiří Vévoda, Bronislava Grygová Department of Humanities and Social Sciences, Faculty of Health Sciences, Palacký University in Olomouc, Olomouc, Czech Republic SUMMARY Objectives: The aim of the study was to assess the prevalence of burnout syndrome and mobbing, to determine their mutual relationship, and to identify predictors related to the probability of occurrence of burnout syndrome in general nurses working in hospitals. Methods: The work is designed as a cross-sectional study. The research took place in 2018 and the sample included 250 general nurses. Sta- tistical evaluation was performed by means of descriptive statistics, Spearman’s correlation coefficient, and logistic regression. Three standardized questionnaires were used – Maslach Burnout Inventory, Negative Questionnaire Act and SUPSO. Results: The research revealed burnout syndrome in the area of emotional exhaustion in 28.8% of nurses, of depersonalization in 15.2%, and in the area of personal accomplishment in 38.4%. 51.2% of nurses never experienced mobbing at workplace, one act of mobbing over the last six months was reported by 17.6% of respondents, two and more acts by 31.2%. Logistic regression revealed that the probability of occurrence of burnout syndrome in the area of emotional exhaustion is influenced by age, sex and by the size of an urban area, it is increased by anxiety and depression. In the area of depersonalization the probability of incidence increases with impulsiveness and dejection. In the area of personal accomplishment the probability of burnout syndrome incidence is increased by the lack of psychological wellbeing and activeness, by restlessness and impulsiveness. -

Racial and Ethnic Disparities in Health Care, Updated 2010
RACIAL AND ETHNIC DISPARITIES IN HEALTH CARE, UPDATED 2010 American College of Physicians A Position Paper 2010 Racial and Ethnic Disparities in Health Care A Summary of a Position Paper Approved by the ACP Board of Regents, April 2010 What Are the Sources of Racial and Ethnic Disparities in Health Care? The Institute of Medicine defines disparities as “racial or ethnic differences in the quality of health care that are not due to access-related factors or clinical needs, preferences, and appropriateness of intervention.” Racial and ethnic minorities tend to receive poorer quality care compared with nonminorities, even when access-related factors, such as insurance status and income, are controlled. The sources of racial and ethnic health care disparities include differences in geography, lack of access to adequate health coverage, communication difficulties between patient and provider, cultural barriers, provider stereotyping, and lack of access to providers. In addition, disparities in the health care system contribute to the overall disparities in health status that affect racial and ethnic minorities. Why is it Important to Correct These Disparities? The problem of racial and ethnic health care disparities is highlighted in various statistics: • Minorities have less access to health care than whites. The level of uninsurance for Hispanics is 34% compared with 13% among whites. • Native Americans and Native Alaskans more often lack prenatal care in the first trimester. • Nationally, minority women are more likely to avoid a doctor’s visit due to cost. • Racial and ethnic minority Medicare beneficiaries diagnosed with dementia are 30% less likely than whites to use antidementia medications. -

June 2015 Broadside
T H E A T L A N T A E A R L Y M U S I C ALLIANCE B R O A D S I D E Volume XV # 4 June, 2015 President’s Message Are we living in the Renaissance? Well, according to the British journalist, Stephen Masty, we are still witnessing new inventions in musical instruments that link us back to the Renaissance figuratively and literally. His article “The 21st Century Renaissance Inventor” [of musical instruments], in the journal “The Imaginative Conservative” received worldwide attention recently regard- ing George Kelischek’s invention of the “KELHORN”. a reinvention of Renaissance capped double-reed instruments, such as Cornamuse, Crumhorn, Rauschpfeiff. To read the article, please visit: AEMA MISSION http://www.theimaginativeconservative.org/2015/05/the-21st-centurys-great-renaissance-inventor.html. It is the mission of the Atlanta Early Music Alli- Some early music lovers play new replicas of the ance to foster enjoyment and awareness of the histor- Renaissance instruments and are also interested in playing ically informed perfor- the KELHORNs. The latter have a sinuous bore which mance of music, with spe- cial emphasis on music makes even bass instruments “handy” to play, since they written before 1800. Its have finger hole arrangements similar to Recorders. mission will be accom- plished through dissemina- tion and coordination of Yet the sound of all these instruments is quite unlike that information, education and financial support. of the Recorder: The double-reed presents a haunting raspy other-worldly tone. (Renaissance? or Jurassic?) In this issue: George Kelischek just told me that he has initiated The Capped Reed Society Forum for Players and Makers of the Crumhorn, President ’ s Message page 1 Cornamuse, Kelhorn & Rauschpfeiff. -

Participatory Design of Integrated Safety and Health Interventions in the Workplace: a Case Study Using the Intervention Design and Analysis Scorecard (IDEAS) Tool
HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author Int J Hum Manuscript Author Factors Ergon Manuscript Author . Author manuscript; available in PMC 2021 April 23. Published in final edited form as: Int J Hum Factors Ergon. 2015 November 11; 3(3-4): 303–326. doi:10.1504/ijhfe.2015.073008. Participatory design of integrated safety and health interventions in the workplace: a case study using the Intervention Design and Analysis Scorecard (IDEAS) Tool Michelle M. Robertson, Center for Behavioral Sciences, Liberty Mutual Research Institute for Safety, 71 Frankland Road, Hopkinton, MA 01748, USA Center for the Promotion of Health in the New England Workplace (CPH-NEW), University of Connecticut, Storrs, CT, USA University of Massachusetts Lowell, Lowell, MA, USA Robert A. Henning, Department of Psychological Sciences, University of Connecticut, 406 Babbidge Road, Unit 1020, Storrs, CT 06269-1020, USA Center for the Promotion of Health in the New England Workplace (CPH-NEW), University of Connecticut, Storrs, CT, USA University of Massachusetts Lowell, Lowell, MA, USA Nicholas Warren, Center for Promotion of Health in the New England Workplace (CPH-NEW), University of Connecticut Health Center, 263 Farmington Avenue, Farmington, CT 06030-8077, USA Center for the Promotion of Health in the New England Workplace (CPH-NEW), University of Connecticut, Storrs, CT, USA University of Massachusetts Lowell, Lowell, MA, USA Suzanne Nobrega, Center for Promotion of Health in the New England Workplace (CPH-NEW), University of -

Role and Value of the Corporate Medical Director
ACOEM GUIDANCE STATEMENT Role and Value of the Corporate Medical Director J. Brent Pawlecki, MD, MMM, Wayne N. Burton, MD, Cherryl Christensen, DO, MS, K. Andrew Crighton, MD, Richard Heron, MB, ChB, FRCP, T. Warner Hudson, MD, Pamela A. Hymel, MD, MPH, and David Roomes, FFOM, FACOEM, ACOEM Corporate Medical Directors Section Task Force accreditation in occupational medicine or the more preferred double The role of the corporate medical director (CMD) has evolved over the last certification in occupational medicine, and another board such as 300 years since Ramazzini first identified diseases of Italian workers in the 01/04/2019 on BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3VFjldD2uL9p7SMbj5XQFggscApMlmW/UgXNoK/5MD7Gq31Q2YQqh0A== by https://journals.lww.com/joem from Downloaded Downloaded internal medicine or family medicine. Further qualifications such as a early 1700s. Since then, there has been a gradual blurring of the boundaries master of public health or masters-level degree in environmental between private and workplace health concerns. Today’s CMD must have health, business administration, or law are highly desirable, including from intimate knowledge of their corporation’s industry and the businesses that knowledge of epidemiology, biostatistics, population health manage- https://journals.lww.com/joem they support, particularly the occupational and environmental programs that ment, business management, and regulatory aspects of employee comply with all local, state, and/or national standards and regulations. health. CMDs should also remain active in their relevant professional Leading companies not only measure compliance with such standards but health organizations to demonstrate that they are remaining current in also may hold programs to their own internal corporate global standards even medicine. -

Optimalizácia Využívania Internetových Sietí V Regióne Košice
Article history: Received 20 November 2019 TRANSPORT & LOGISTICS: Accepted 31 December 2019 the International Journal Available online 09 January 2020 ISSN 2406-1069 ––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––– Article citation info: Pacaiova, H., Galtz, J., Darvaši, P., Habala, I. The requirements on machinery safety and their influence on OHS effectiveness. Transport & Logistics: the International Journal, 2019; Volume 19, Issue 47, December 2019, ISSN 2406-1069 THE REQUIREMENTS ON MACHINERY SAFETY AND THEIR INFLUENCE ON OHS EFFECTIVENESS Hana Pacaiova 1, Juraj Glatz 1, Peter Darvaši 1, Ivan Habala 1 1 Technical University of Kosice, Faculty of Mechanical Engineering, Letna 9, 04200 Kosice, Slovakia, tel: +4210556022290, e-mail: [email protected]; [email protected]; [email protected]; [email protected] Abstract: A legislative requirement that specifies the scope for occupational health and safety (OHS) and machinery safety has been implemented in the EU for 30 years. Basic condition for maintaining OHS is safely constructed and operated machinery / equipment. The obligation of constructors (producer, representative) is to launch only such machinery equipment which does not threaten health and safety of persons, domestic animals or property. The criterion for meeting these regulations is risk assessment. For maintenance activities, there are, in the EU directive on machinery safety (2006/42/ES), set requirements for the isolation of hazardous energy, which may threaten life or health of maintenance workers when performing the required activity. Identification process of this energy must be a part of risk assessment, the result of which is such a construction solution that enables disconnecting from all energy sources in a safe and convenient way together with its lockout. -

Different Perspectives for Assigning Weights to Determinants of Health
COUNTY HEALTH RANKINGS WORKING PAPER DIFFERENT PERSPECTIVES FOR ASSIGNING WEIGHTS TO DETERMINANTS OF HEALTH Bridget C. Booske Jessica K. Athens David A. Kindig Hyojun Park Patrick L. Remington FEBRUARY 2010 Table of Contents Summary .............................................................................................................................................................. 1 Historical Perspective ........................................................................................................................................ 2 Review of the Literature ................................................................................................................................... 4 Weighting Schemes Used by Other Rankings ............................................................................................... 5 Analytic Approach ............................................................................................................................................. 6 Pragmatic Approach .......................................................................................................................................... 8 References ........................................................................................................................................................... 9 Appendix 1: Weighting in Other Rankings .................................................................................................. 11 Appendix 2: Analysis of 2010 County Health Rankings Dataset ............................................................ -

ISO 45001- Safety Management System Discussion Abstract May 2016
Aon Risk Solutions Aon Global Risk Consulting ISO 45001- Safety Management System Discussion Abstract May 2016 Risk. Reinsurance. Human Resources. Aon Risk Solutions Aon Global Risk Consulting Summary of Safety Management Standards Safety management is a topic of significant concern for many organizations. When you consider how many activities must be undertaken and overseen to execute and implement a successful organization- wide safety process, results demonstrate the investment provides clear and measurable value. Although different organizations and industries face unique risks and have distinct safety requirements, there remains a commonality in safety practices that can be managed within certain tolerances. Additionally, fundamental practices, such as risk identification and assessment, incident investigation, employee engagement, and auditing, have universal application among organizations worldwide. To this end, a number of consensus standards have been established that provide guidance to help organizations establish internal safety management protocols. These standards provide the foundation and framework that enable organizations to model safety practices and activities. These standards provide guidance for the development, implementation, execution, and sustainment of safety management practices. These standards are often specific to the country or environment where the organization conducts its operations and in turn allows firms to address region- or country-specific regulatory expectations enabling them to tailor the standard’s expectations to meet those regulations. However, this has also resulted in a plethora of standards which vary in some notable ways. In an attempt to expand the degree of standardization of safety practices, the International Standards Organization (ISO) began working on unifying safety standards. This effort traces its roots back to the mid-2000’s; however, the first formal ISO 45001 committee was not convened until 2010 and then required four years to develop the first draft standard. -
Balancing Function Unit 4
BALANCING FUNCTION UNIT 4 Dr. P.V. S LAKSHMI JAGADAMBA Professor, Department of CSE, GVP College of Engineering for Women INTRODUCTION User experiences play a critical role in influencing software acceptance Conversational messages have their limits Design needs to be comprehensible, predictable, and controllable Information layout is important Multi window coordination Large, fast, high-resolution color displays have potential Recognition of the creative challenge of balancing function and fashion may lead to designers even working even harder. 2 INTRODUCTION “This chapter deals with six design matters that are functional issues with varying styles/solutions to suite a variety of users.” Error messages Non-anthropomorphic design Display design Web page design Window design Colour 3 ERROR MESSAGES Overview User experience with computer-system prompts, explanations, error diagnostics, and warnings is crucial in influencing acceptance of SW systems Why do errors occur? Lack of knowledge, incorrect understanding, inadequate slips What is the consequence? Users are likely to be confused, are anxious or feel inadequate What is a solution? Make error messages as user-friendly as possible; this is especially important for novice users as they commonly have a lack of knowledge, confidence, and are sometimes easily frustrated or discouraged 4 ERROR MESSAGES Improving Error Messages Measure where errors occur frequently, focus on these issues Improve messages but also revise error handling procedures, improve documentation