Capital Market Day 2018
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Market Notice Date: 14 November 2019 Market Notice Number: 112/2019
Market Notice Date: 14 November 2019 Market Notice Number: 112/2019 Equiduct Universe Change Please see today's changes below effective 18 November 2019: Trading Reporting MIC Settlement Trading Settlement Tick Size Change/ Security Name ISIN Home Market Symbol Country Currency Currency table Action ABB LTD ABBNz CH0012221716 XSWX EQTB CH CHF CHF ESMA_E Deletion ABB ABBs CH0012221716 XSTO EQTB SE SEK SEK ESMA_E Deletion ADECCO SA ADENz CH0012138605 XSWX EQTC CH CHF CHF ESMA_E Deletion AMS AG AMSz AT0000A18XM4 XSWX EQTC CH CHF CHF ESMA_E Deletion ARYZTA AG ARYNz CH0043238366 XSWX EQTB CH CHF CHF ESMA_E Deletion JULIUS BAER GRUPPE AG BAERz CH0102484968 XSWX EQTC CH CHF CHF ESMA_E Deletion BALOISE-HLDGS BALNz CH0012410517 XSWX EQTC CH CHF CHF ESMA_D Deletion BARRY CALLEBAUT AG BARNz CH0009002962 XSWX EQTC CH CHF CHF ESMA_D Deletion BB BIOTECH BBZAd CH0038389992 XETR EQTB DE EUR EUR ESMA_D Deletion BB BIOTECH BIONz CH0038389992 XSWX EQTB CH CHF CHF ESMA_D Deletion BASILEA PHARMACEUTICA AG BSLNz CH0011432447 XSWX EQTC CH CHF CHF ESMA_D Deletion BUCHER INDUSTRIES BUCNz CH0002432174 XSWX EQTC CH CHF CHF ESMA_D Deletion COMPAGNIE FINANCIERE RICHEMONT CFRz CH0210483332 XSWX EQTC CH CHF CHF ESMA_E Deletion CLARIANT CLNz CH0012142631 XSWX EQTC CH CHF CHF ESMA_E Deletion CEMBRA MONEY BANK AG CMBNz CH0225173167 XSWX EQTC CH CHF CHF ESMA_D Deletion CREDIT SUISSE GROUP AG CSGNz CH0012138530 XSWX EQTC CH CHF CHF ESMA_E Deletion DKSH HOLDING DKSHz CH0126673539 XSWX EQTC CH CHF CHF ESMA_D Deletion DORMA+KABA HOLDING AG DOKAz CH0011795959 XSWX EQTC CH CHF -

Remuneration
REMUNERATION 124 Vifor Pharma Ltd. Annual Report 2020 HIGHLIGHTS PEOPLE 126 Chairwoman’s overview 128 Philosophy and approach to remuneration 130 Governance 134 Board and Executive remuneration 139 Remuneration awarded in 2020 and 2019 146 Overview of executive remuneration in 2020 and 2019 147 Outlook: changes in remuneration model for 2021 148 Statutory auditor’s report PORTFOLIO RESPONSIBILITY GOVERNANCE REMUNERATION FINANCE Vifor Pharma Ltd. Annual Report 2020 125 REMUNERATION CHAIRWOMAN’S OVERVIEW The remuneration “programs of Vifor Pharma are designed to support our corporate strategy and to ensure a sustainable performance towards our future objectives.” SUE MAHONY CHAIRWOMAN OF THE REMUNERATION COMMITTEE 126 Vifor Pharma Ltd. Annual Report 2020 HIGHLIGHTS “ We reward entrepreneurial Vifor Pharma’s remuneration philosophy aims to attract and retain highly talented and behaviour that ethical individuals who help us ensure the drives sustainable long-term competitiveness and success of our PEOPLE business, to meet the needs of patients, to performance and look after the interests of our stakeholders and the environment in order to deliver on the long-term value strategy and to sustain profitable growth. This report sets out the remuneration policies for creation.” the Board of Directors and Executive Commit- tee which are designed to help them achieve these goals. A year of unprecedented challenges for Chief Medical Officer and Gregory Oakes as countries and companies around the world President North America. PORTFOLIO has underlined the importance of a strong and transparent remuneration framework. The Remuneration Committee considers Vifor Notwithstanding, as in previous years, Vifor Pharma appropriately positioned to enable it Pharma’s philosophy and approach to remu- to compete successfully with its peers and to neration has remained stable: we reward support its ambitious growth plans. -

Switzerland Fund A-CHF for Investment Professionals Only FIDELITY FUNDS MONTHLY PROFESSIONAL FACTSHEET SWITZERLAND FUND A-CHF 31 AUGUST 2021
pro.en.xx.20210831.LU0054754816.pdf Switzerland Fund A-CHF For Investment Professionals Only FIDELITY FUNDS MONTHLY PROFESSIONAL FACTSHEET SWITZERLAND FUND A-CHF 31 AUGUST 2021 Strategy Fund Facts The Portfolio Managers are bottom-up investors who believe share prices are Launch date: 13.02.95 correlated to earnings, and that strong earners will therefore outperform. They look to Portfolio manager: Andrea Fornoni, Alberto Chiandetti invest in companies where the market underestimates earnings because their Appointed to fund: 01.03.18, 01.08.11 sustainability is not fully appreciated. They also look for situations where the impact Years at Fidelity: 7, 15 company changes will have on earnings has not been fully recognised by the market. Fund size: CHF366m They aim to achieve a balance of different types of companies, so they can deliver Number of positions in fund*: 36 performance without adding undue risk. Fund reference currency: Swiss Franc (CHF) Fund domicile: Luxembourg Fund legal structure: SICAV Management company: FIL Investment Management (Luxembourg) S.A. Capital guarantee: No Portfolio Turnover Cost (PTC): 0.01% Portfolio Turnover Rate (PTR): 28.92% *A definition of positions can be found on page 3 of this factsheet in the section titled “How data is calculated and presented.” Objectives & Investment Policy Share Class Facts • The fund aims to provide long-term capital growth with the level of income expected Other share classes may be available. Please refer to the prospectus for more details. to be low. • The fund will invest at least 70% in Swiss company shares. Launch date: 13.02.95 • The fund has the freedom to invest outside its principal geographies, market sectors, industries or asset classes. -

FTSE Publications
2 FTSE Russell Publications FTSE Developed Europe SMID Cap 19 August 2021 Tradable Plus Indicative Index Weight Data as at Closing on 30 June 2021 Index weight Index weight Index weight Constituent Country Constituent Country Constituent Country (%) (%) (%) 3i Group 0.72 UNITED Bureau Veritas S.A. 0.42 FRANCE Gjensidige Forsikring ASA 0.17 NORWAY KINGDOM Campari 0.31 ITALY Gn Store Nordic 0.53 DENMARK AAK 0.18 SWEDEN Carl Zeiss Meditec 0.33 GERMANY Halma 0.66 UNITED Aalberts NV 0.24 NETHERLANDS Castellum 0.32 SWEDEN KINGDOM ABN AMRO Bank NV 0.23 NETHERLANDS Centrica 0.2 UNITED Hargreaves Lansdown 0.39 UNITED Acciona S.A. 0.16 SPAIN KINGDOM KINGDOM Accor 0.32 FRANCE Chr. Hansen Holding A/S 0.43 DENMARK Hays 0.16 UNITED ACS Actividades Cons y Serv 0.3 SPAIN Clariant 0.21 SWITZERLAND KINGDOM Adecco Group AG 0.49 SWITZERLAND Coca-Cola HBC AG 0.33 UNITED HeidelbergCement AG 0.6 GERMANY Adevinta 0.21 NORWAY KINGDOM HelloFresh SE 0.67 GERMANY Admiral Group 0.43 UNITED Cofinimmo 0.21 BELGIUM Helvetia Holding AG 0.18 SWITZERLAND KINGDOM Commerzbank 0.35 GERMANY Hikma Pharmaceuticals 0.27 UNITED Aedifica 0.22 BELGIUM ConvaTec Group 0.25 UNITED KINGDOM Aegon NV 0.34 NETHERLANDS KINGDOM Hiscox 0.18 UNITED KINGDOM Aeroports de Paris 0.17 FRANCE Countryside Properties 0.16 UNITED Holmen AB 0.2 SWEDEN Ageas 0.46 BELGIUM KINGDOM Homeserve 0.17 UNITED Aker BP ASA 0.16 NORWAY Covestro AG 0.54 GERMANY KINGDOM Alfa Laval 0.52 SWEDEN Covivio 0.2 FRANCE Howden Joinery Group 0.3 UNITED Alstom 0.7 FRANCE Croda International 0.64 UNITED KINGDOM KINGDOM Alten 0.18 -

Portfolio of Investments
PORTFOLIO OF INVESTMENTS Variable Portfolio – Partners International Value Fund, September 30, 2020 (Unaudited) (Percentages represent value of investments compared to net assets) Investments in securities Common Stocks 97.9% Common Stocks (continued) Issuer Shares Value ($) Issuer Shares Value ($) Australia 4.2% UCB SA 3,232 367,070 AMP Ltd. 247,119 232,705 Total 13,350,657 Aurizon Holdings Ltd. 64,744 199,177 China 0.6% Australia & New Zealand Banking Group Ltd. 340,950 4,253,691 Baidu, Inc., ADR(a) 15,000 1,898,850 Bendigo & Adelaide Bank Ltd. 30,812 134,198 China Mobile Ltd. 658,000 4,223,890 BlueScope Steel Ltd. 132,090 1,217,053 Total 6,122,740 Boral Ltd. 177,752 587,387 Denmark 1.9% Challenger Ltd. 802,400 2,232,907 AP Moller - Maersk A/S, Class A 160 234,206 Cleanaway Waste Management Ltd. 273,032 412,273 AP Moller - Maersk A/S, Class B 3,945 6,236,577 Crown Resorts Ltd. 31,489 200,032 Carlsberg A/S, Class B 12,199 1,643,476 Fortescue Metals Group Ltd. 194,057 2,279,787 Danske Bank A/S(a) 35,892 485,479 Harvey Norman Holdings Ltd. 144,797 471,278 Demant A/S(a) 8,210 257,475 Incitec Pivot Ltd. 377,247 552,746 Drilling Co. of 1972 A/S (The)(a) 40,700 879,052 LendLease Group 485,961 3,882,083 DSV PANALPINA A/S 15,851 2,571,083 Macquarie Group Ltd. 65,800 5,703,825 Genmab A/S(a) 1,071 388,672 National Australia Bank Ltd. -
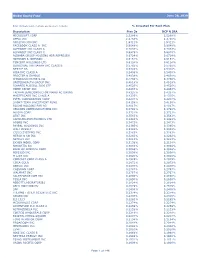
Global Equity Fund Description Plan 3S DCP & JRA MICROSOFT CORP
Global Equity Fund June 30, 2020 Note: Numbers may not always add up due to rounding. % Invested For Each Plan Description Plan 3s DCP & JRA MICROSOFT CORP 2.5289% 2.5289% APPLE INC 2.4756% 2.4756% AMAZON COM INC 1.9411% 1.9411% FACEBOOK CLASS A INC 0.9048% 0.9048% ALPHABET INC CLASS A 0.7033% 0.7033% ALPHABET INC CLASS C 0.6978% 0.6978% ALIBABA GROUP HOLDING ADR REPRESEN 0.6724% 0.6724% JOHNSON & JOHNSON 0.6151% 0.6151% TENCENT HOLDINGS LTD 0.6124% 0.6124% BERKSHIRE HATHAWAY INC CLASS B 0.5765% 0.5765% NESTLE SA 0.5428% 0.5428% VISA INC CLASS A 0.5408% 0.5408% PROCTER & GAMBLE 0.4838% 0.4838% JPMORGAN CHASE & CO 0.4730% 0.4730% UNITEDHEALTH GROUP INC 0.4619% 0.4619% ISHARES RUSSELL 3000 ETF 0.4525% 0.4525% HOME DEPOT INC 0.4463% 0.4463% TAIWAN SEMICONDUCTOR MANUFACTURING 0.4337% 0.4337% MASTERCARD INC CLASS A 0.4325% 0.4325% INTEL CORPORATION CORP 0.4207% 0.4207% SHORT-TERM INVESTMENT FUND 0.4158% 0.4158% ROCHE HOLDING PAR AG 0.4017% 0.4017% VERIZON COMMUNICATIONS INC 0.3792% 0.3792% NVIDIA CORP 0.3721% 0.3721% AT&T INC 0.3583% 0.3583% SAMSUNG ELECTRONICS LTD 0.3483% 0.3483% ADOBE INC 0.3473% 0.3473% PAYPAL HOLDINGS INC 0.3395% 0.3395% WALT DISNEY 0.3342% 0.3342% CISCO SYSTEMS INC 0.3283% 0.3283% MERCK & CO INC 0.3242% 0.3242% NETFLIX INC 0.3213% 0.3213% EXXON MOBIL CORP 0.3138% 0.3138% NOVARTIS AG 0.3084% 0.3084% BANK OF AMERICA CORP 0.3046% 0.3046% PEPSICO INC 0.3036% 0.3036% PFIZER INC 0.3020% 0.3020% COMCAST CORP CLASS A 0.2929% 0.2929% COCA-COLA 0.2872% 0.2872% ABBVIE INC 0.2870% 0.2870% CHEVRON CORP 0.2767% 0.2767% WALMART INC 0.2767% -
Swiss Small and Mid-Cap Equities – Consistent Value Creation
Swiss Small and Mid-Cap Equities – Consistent value creation White Paper For professional investors in Switzerland or professional investors as defined by the relevant laws Asset Management | November 2020 Performance of major equity markets (%) Key points 100 ■ The Swiss economy has once again proven its 80 resilience during the Covid-19 pandemic, as 60 reflected by year-to-date outperformance in the 40 Swiss equity market and also its small and mid- 20 cap segment. 0 ■ Several Swiss companies across all market-cap -20 segments have benefited from the disruption -40 caused by the pandemic, since they have CHF CHF USD USD USD EUR EUR EUR GBP exposure to underlying long-term trends that SPI SPI MSCI S&P S&P MSCI MSCI DAX FTSE Extra AC 500 MidcapEurope Europe Mid 250 have been accelerated by the crisis. World 400 Small Cap ■ However, the strongest argument for exposure to Cap Swiss equities within a diversified equity YTD 5Y portfolio remains the consistent long-term Sources: UBP and, Bloomberg Finance LP. Data as of September 2020. Past performance is not a guide to current or outperformance of Swiss equities, driven by their future results. superior value-creation and ESG profiles. ■ An active investment approach, driven by The 2020 EPS growth estimate for global equities has fundamentals and supported by extensive remained steady at around -19% over the past few expertise and knowledge of the market, has led months, while the 2021 estimate now stands at almost to an impressive track record and substantial +30%. Expected regional earnings growth rates for 2020 AuM growth for UBP’s Swiss equity franchise range from +0% for China to -39% for the UK and the over the last 14 years. -

Calvert VP EAFE International Index Portfolio 1St Quarter Holdings
Calvert VP EAFE International Index Portfolio March 31, 2020 Schedule of Investments (Unaudited) Common Stocks — 98.5% Security Shares Value Australia (continued) Security Shares Value Australia — 5.8% Ramsay Health Care, Ltd. 1,442 $ 50,704 REA Group, Ltd. 537 25,155 AGL Energy, Ltd. 6,090 $ 63,734 Rio Tinto, Ltd. 3,172 163,420 Alumina, Ltd.(1) 14,501 12,996 Santos Ltd., 13,517 27,761 AMP,Ltd.(1)(2) 22,416 18,306 Scentre Group 45,895 43,959 APA Group(1) 11,361 72,094 Seek, Ltd.(1) 3,323 30,366 Aristocrat Leisure, Ltd. 4,773 61,847 Sonic Healthcare, Ltd. 4,020 60,420 ASX, Ltd. 1,623 76,185 South32, Ltd. 48,353 53,377 Aurizon Holdings, Ltd. 16,477 42,701 Stockland 19,317 29,704 AusNet Services(1) 27,031 28,383 Suncorp Group, Ltd.(1) 11,330 62,918 Australia & New Zealand Banking Group, Ltd. 24,210 253,900 Sydney Airport 8,748 30,225 Bendigo & Adelaide Bank, Ltd. 4,706 18,080 Tabcorp Holdings, Ltd.(1) 15,814 24,474 BGP Holdings PLC(2)(3) 77,172 — Telstra Corp., Ltd. 37,215 69,858 BHP Group, Ltd. 26,250 476,209 TPG Telecom, Ltd.(1) 3,460 14,735 BlueScope Steel, Ltd. 4,388 22,973 Transurban Group(1) 24,274 180,808 Boral, Ltd. 10,917 13,712 Treasury Wine Estates, Ltd. 6,449 40,039 Brambles, Ltd. 14,024 90,648 Vicinity Centres 25,959 16,238 Caltex Australia, Ltd. 1,867 25,210 Washington H. -

Letter to Investors
The Way of Pricing Leonardo Da Vinci has been credited with designing the first helicopter in 1493. The future is never clear. CONTENTS Cristal ball - page 3 When is the Euro crisis over? Attractive situations - page 7 January 2012 Meyer Burger N°1 Interview with an Entrepreneur - page 8 Author Etienne Jornod - Executive Chairman of the Alexandre R. Kaufmann Board of Directors of Galenica Ltd Noise from the street - page 14 Price Kuehne + Nagel & China CHF 20.- Kaufmann Kapital AG for Incrementum advisors AG Introduction The idea of this Letter is not to provide you with investment tips. The idea is to remind, present and promote the Way of Pricing, as opposed to the widely spread market timing tendency, that can be practiced alone without the help of any "investment professional". If you invest with the attitude of a businessman, then this Letter is for you. If the share of a listed company represents merely a piece of paper that can be traded in the hopes of making money tomorrow, then this Letter did not land in the right place. Where to find it? www.kaufmann-kapital.ch section Letter to Investors. Disclaimer The information presented in this document are provided for your personal information only, and are not to be used or considered as an offer or solicitation to buy, sell or subscribe to any securities. The price of and revenues from any of the securities or financial instrument mentioned in this document can go up as well as down. This document does merely constitute the different assumptions, views and analytical methods of the author who prepared it, and might not necessarily constitute the assumptions, views, and analytical methods of the other partners working at Incrementum advisors AG. -

Unterschleißheim, 27
Program BAADER HELVEA SWISS EQUITIES CONFERENCE 10 – 11 January 2019 Grand Resort Bad Ragaz, Switzerland CONTACTS @ BAADER HELVEA Lukas Burkart, Head of Equity Sales T +49 89 5150 1858, [email protected] Andreas von Arx, Head of Equity Research Switzerland T +41 43 388 9257, [email protected] Reto Amstalden, Equity Research T +41 43 388 9261, [email protected] www.baaderbank.com Enable Change in Banking. Baader Helvea Swiss Equities Conference 10 – 11 January 2019 PRESENTING COMPANIES 67 companies have agreed to participate in the Swiss Equities Conference 2019: Bloomberg Reuters Company name ticker ticker Sector Addex Therapeutics ADXN SE ADXN.S Pharma & Healthcare Adecco Group ADEN SE ADEN.S Business Services & Logistics ARBONIA ARBN SE ARBNO.S Construction Ascom ASCN SE ASCN.S Technology Baloise BALN SE BALN.S Banks & Insurance Basilea (one-on-one only) BSLN SE BSLN.S Pharma & Healthcare BB Biotech (one-on-one only) BION SW BION.S Pharma & Healthcare BKW AG BKW SE BKWB.S Utilities Bossard BOSN SE BOS.S Industrials Bucher Industries BUCN SE BUCN.S Industrials Cembra Money Bank CMBN SE CMBN.S Banks & Insurance Clariant CLN SE CLN.S Chemicals COLTENE CLTN SE CLTN.S Pharma & Healthcare Compagnie Financière Tradition (one-on-one only) CFT SE CFT.S Banks & Insurance Conzzeta CON SE CONC.S Industrials Dätwyler Holding Inc. DAE SE DAE.S Technology dormakaba DOKA SE DOKA.S Industrials Dufry DUFN SE DUFN.S Consumer & Retail EFG International EFGN SE EFGN.S Banks & Insurance Evolva (one-on-one only) EVE SE EVE.S Chemicals Galenica -

Barry Callebaut Annual Report 2019/20
abrina Key figures 2019/20 Sales volume EBIT recurring Net profit recurring Free cash flow Proposed dividend –2.0% –13.8%1 in local currencies –13.3%1 in local currencies 39% payout ratio 2.1 491.0 319.3 317 22.00 million tonnes CHF million CHF million CHF per share CHF million 1 Operating profit (EBIT) recurring and Net profit recurring exclude the cost of CHF –7.8 million for the closure of the Makassar, Indonesia, cocoa factory. Prior-year comparatives have been calculated on a pro-forma basis to reflect the estimated impact of IFRS 16 had it been adopted at the time. Sales volume Sales revenue In tonnes In CHF million 2,400,000 9,000 2,000,000 7,500 1,600,000 6,000 1,200,000 4,500 800,000 3,000 400,000 1,500 0 0 2015/16 2016/17 2017/18 2018/19 2019/20 2015/16 2016/17 2017/18 2018/19 2019/20 EBIT Net profit for the year In CHF million In CHF million 700 400 600 500 300 400 300 200 200 100 100 0 2015/16 2016/17 2017/18 2018/19 2019/20 0 2015/16 2016/17 2017/18 2018/19 2019/20 Sales volume by Region Sales volume by Product Group 10% In tonnes 22% In tonnes EMEA 945,640 Food Manufacturers 1,429,178 22% Americas 565,650 45% Cocoa Products 457,386 Asia Pacific 127,306 Gourmet & Specialties 209,418 Global Cocoa 457,386 6% 68% 27% Barry Callebaut | Annual Report / Fiscal year 2019/20 in brief • Sales volume down –2.0%, progressive volume recovery in fourth quarter • Sales revenue of CHF 6.9 billion, down –0.4% in local currencies (–5.7% in CHF) • Operating profit (EBIT) recurring1 of CHF 491.0 million, down –13.8%2 in local currencies (–18.5%2 in CHF) • Net profit recurring1 of CHF 319.3 million, down –13.3%2 in local currencies (–18.5%2 in CHF) • Strong Free cash flow of CHF 317 million • Confident on mid-term guidance3 • Board member Suja Chandrasekaran will not stand for reelection. -

Remuneration Report
Letter to Shareholders Overview Business Highlights Sustainability Our People Financial Reports Governance Remuneration Report Remuneration Report Dear Shareholders, Committee members, the determination of the remuneration of the members of Executive Committee, as well as the On behalf of the Nomination and Compensation Committee, preparation of the Remuneration Report and of the say-on- I am pleased to share with you the Remuneration Report for pay vote at the Annual General Meeting. the fiscal year 2018/19. This Remuneration Report has been You will find further information on the activities of the prepared in accordance with the “Ordinance against NCC and on Barry Callebaut’s remuneration programs on Excessive Compensation in listed Companies” (OaEC), the following pages. Art. 663c paragraph 3 of the Swiss Code of Obligations and the Corporate Governance Directive issued by SIX At the 2019 General Meeting, we will request your approval Exchange Regulation. of the total remuneration amount to be awarded to the Board In the fiscal year 2018/19, the Group achieved strong of Directors for the period until the following General results with profitable growth and good cash generation Meeting, the maximum aggregate amount of fixed driven by a consistent execution of its ‘smart growth’ remuneration to be awarded to the Executive Committee in strategy. fiscal year 2020/21, and the maximum aggregate amount of This reports explains how the performance in the variable remuneration awarded to the Executive Committee reporting year impacted the compensation paid to the in fiscal year 2018/19. Additionally, you will have the Executive Committee under the incentive plans. opportunity to express your opinion on this Remuneration During the reporting year, the Nomination and Report in a consultative vote.