Executive Session
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Autism CARES Act of 2014’’
PUBLIC LAW 113–157—AUG. 8, 2014 128 STAT. 1831 Public Law 113–157 113th Congress An Act To reauthorize certain provisions of the Public Health Service Act relating to autism, Aug. 8, 2014 and for other purposes. [H.R. 4631] Be it enacted by the Senate and House of Representatives of the United States of America in Congress assembled, Autism Collaboration, SECTION 1. SHORT TITLE. Accountability, This Act may be cited as the ‘‘Autism Collaboration, Account- Research, Education, and ability, Research, Education, and Support Act of 2014’’ or the Support Act ‘‘Autism CARES Act of 2014’’. of 2014. 42 USC 201 note. SEC. 2. NATIONAL AUTISM SPECTRUM DISORDER INITIATIVE. 42 USC 280i (a) IN GENERAL.—The Secretary of Health and Human Services note. shall designate an existing official within the Department of Health Consultation. and Human Services to oversee, in consultation with the Secretaries of Defense and Education, national autism spectrum disorder research, services, and support activities. (b) DUTIES.—The official designated under subsection (a) shall— (1) implement autism spectrum disorder activities, taking into account the strategic plan developed by the Interagency Autism Coordinating Committee under section 399CC(b) of the Public Health Service Act (42 U.S.C. 280i–2(b)); and (2) ensure that autism spectrum disorder activities of the Department of Health and Human Services and of other Federal departments and agencies are not unnecessarily duplicative. SEC. 3. RESEARCH PROGRAM. Section 399AA of the Public Health Service Act (42 U.S.C. -

Entire Issue (PDF 2MB)
E PL UR UM IB N U U S Congressional Record United States th of America PROCEEDINGS AND DEBATES OF THE 116 CONGRESS, FIRST SESSION Vol. 165 WASHINGTON, WEDNESDAY, JULY 24, 2019 No. 125 House of Representatives The House met at 10 a.m. and was They grew up in families of very portunities for mentorship, profes- called to order by the Speaker pro tem- modest means. While working full sional development, and scholarships. pore (Mr. CUELLAR). time, Ralph began a one-man security The society invites members who are f business in 1963. What started as Lake dedicated to education in different Norman Security Patrol, Inc., ex- fields, both active and retired, to build DESIGNATION OF SPEAKER PRO panded into two of the most successful up future leaders at the local level. As TEMPORE businesses in North Carolina and the we all know, the local level is where The SPEAKER pro tempore laid be- country: Security Central and the best practices and policies in edu- fore the House the following commu- AlarmSouth. cation come from. nication from the Speaker: Ralph learned the importance of se- Knowing that young educators in the WASHINGTON, DC, curity while serving as a U.S. Army po- Fifth District have such talented and July 24, 2019. liceman and turned his knowledge into locally engaged women behind them I hereby appoint the Honorable HENRY security and patrol services for homes makes me very proud. These women CUELLAR to act as Speaker pro tempore on and commercial entities. are shining examples of the powerful this day. -
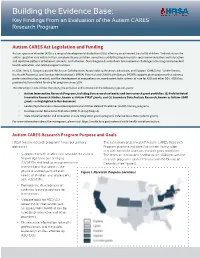
Key Findings from an Evaluation of the Autism CARES Research Program
Building the Evidence Base: Key Findings From an Evaluation of the Autism CARES Research Program Autism CARES Act Legislation and Funding Autism spectrum disorder (ASD) is a range of developmental disabilities (DDs) affecting an estimated 1 out of 59 children.1 Individuals on the autism spectrum vary widely in their symptomatic presentation, sometimes exhibiting impairments in social communication and interaction and repetitive patterns of behavior, interests, and activities. Once diagnosed, individuals face numerous challenges accessing recommended health, education, and related support services. In 2014, the U.S. Congress passed the Autism Collaboration, Accountability, Research, Education, and Support (CARES) Act.2 Under the act, the Health Resources and Services Administration’s (HRSA) Maternal and Child Health Bureau (MCHB) supports grant programs that advance professional training, research, and the development of comprehensive, coordinated State systems of care for ASD and other DDs. HRSA has provided autism-related funding for programs since 2008. This document is one of four describing the activities and successes of the following types of grants: Autism Intervention Research Programs, including five research networks and two research grant portfolios: (1) Field-Initiated Innovative Research Studies, known as Autism-FIRST grants; and (2) Secondary Data Analysis Research, known as Autism-SDAR grants—as highlighted in this document Leadership Education in Neurodevelopmental and Other Related Disabilities (LEND) training programs -

GAO-17-352, YOUTH with AUTISM: Federal Agencies Should Take
United States Government Accountability Office Report to Congressional Requesters May 2017 YOUTH WITH AUTISM Federal Agencies Should Take Additional Action to Support Transition- Age Youth GAO-17-352 May 2017 YOUTH WITH AUTISM Federal Agencies Should Take Additional Action to Support Transition-Age Youth Highlights of GAO-17-352, a report to congressional requesters Why GAO Did This Study What GAO Found Research suggests that youth with According to GAO’s nationwide survey of school district special education ASD are less likely than youth with directors, GAO estimates that about 85 percent of districts in school year 2015- other disabilities to be successful in 16, provided youth with Autism Spectrum Disorder (ASD) services such as transitioning to work and instruction on life, social, and behavioral skills, as they transition from high postsecondary education and school to adulthood. ASD is a group of complex developmental disorders therefore, they may face a lifetime of characterized by difficulties with social interactions, communication, and reliance on public assistance. GAO repetitive behaviors. Districts provided these services as part of the planning for was asked to examine services the transition to adulthood required by the Individuals with Disabilities Education provided under IDEA to assist youth Act (IDEA). Fewer, though still a majority of, districts reported providing certain with ASD in transitioning to adulthood. types of employment-related supports. For example, GAO estimates that 69 For this report, GAO examined (1) services and supports provided to percent provided work experiences and 63 percent provided job coaching. While assist youth with ASD in transitioning the majority of districts reported providing transition services to students with to adulthood, (2) key challenges in ASD, the services provided varied by factors such as the size and poverty level successfully transitioning, and (3) the of the district, according to GAO’s analysis of survey responses. -

Young Adults and Transitioning Youth with Autism Spectrum Disorder
2017 REPORT TO CONGRESS Young Adults and Transitioning Youth with Autism Spectrum Disorder Prepared by the: Department of Health and Human Services Submitted by the: National Autism Coordinator U.S. Department of Health and Human Services Cover Design Medical Arts Branch, Office of Research Services, National Institutes of Health Copyright Information All material appearing in this report is in the public domain and may be reproduced or copied. A suggested citation follows. Suggested Citation U.S. Department of Health and Human Services. Report to Congress: Young Adults and Transitioning Youth with Autism Spectrum Disorder. October 2017. Retrieved from the U.S. Department of Health and Human Services website: https://www.hhs.gov/sites/default/files/2017AutismReport.pdf Young Adults and Transitioning Youth with Autism Spectrum Disorder The Autism Collaboration, Accountability, Research, Education and Support Act (Autism CARES Act) of 2014 REPORT TO CONGRESS Submitted by the National Autism Coordinator of the U.S. Department of Health and Human Services August 3, 2017 Table of Contents Interagency Workgroup on Young Adults and Youth with Autism Spectrum Disorder Transitioning to Adulthood ................................................................................................ iv Steering Committee .................................................................................................... iv Members .................................................................................................................. iv OASH Stakeholder -

Insurance Mandates for Diagnosis and Treatment of Children and Adolescents with Autism and Evaluative Data Sources: a Case Study of Two U.S
Georgia State University ScholarWorks @ Georgia State University Public Health Capstone Projects School of Public Health Spring 4-23-2015 Insurance Mandates for Diagnosis and Treatment of Children and Adolescents with Autism and Evaluative Data Sources: A Case Study of Two U.S. States Sofia Campos Vidal Pires Follow this and additional works at: https://scholarworks.gsu.edu/iph_capstone Recommended Citation Campos Vidal Pires, Sofia, "Insurance Mandates for Diagnosis and Treatment of Children and Adolescents with Autism and Evaluative Data Sources: A Case Study of Two U.S. States." , Georgia State University, 2015. https://scholarworks.gsu.edu/iph_capstone/5 This Capstone Project is brought to you for free and open access by the School of Public Health at ScholarWorks @ Georgia State University. It has been accepted for inclusion in Public Health Capstone Projects by an authorized administrator of ScholarWorks @ Georgia State University. For more information, please contact [email protected]. INSURANCE MANDATES FOR DIAGNOSIS AND TREATMENT OF CHILDREN AND ADOLESCENTS WITH AUTISM AND EVALUATIVE DATA SOURCES: A CASE STUDY OF TWO U.S. STATES by SOFIA CAMPOS VIDAL PIRES B.S.N., UNIVERSIDADE FEDERAL DE PERNAMBUCO, BRAZIL A Capstone Submitted to the Graduate Faculty of Georgia State University in Partial Fulfillment of the Requirements for the Degree MASTER OF PUBLIC HEALTH ATLANTA, GEORGIA 30303 2015 APPROVAL PAGE INSURANCE MANDATES FOR DIAGNOSIS AND TREATMENT OF CHILDREN AND ADOLESCENTS WITH AUTISM AND EVALUATIVE DATA SOURCES: A CASE STUDY OF TWO U.S. STATES by SOFIA CAMPOS VIDAL PIRES Approved: Committee Chair Committee Member ____/____/________ Date ACKNOWLEDGEMENTS First, I would like to express my sincere gratitude to my committee chair, Dr. -

MEMORANDUM June 21, 2019 To: Subcommittee on Health Majority
MEMORANDUM June 21, 2019 To: Subcommittee on Health Majority Members and Staff Fr: Committee on Energy and Commerce Majority Staff Re: Hearing on “Reauthorizing Vital Health Programs for American Families” On Tuesday, June 25, 2019, at 10 a.m. in the John D. Dingell Room, 2123 of the Rayburn House Office Building, the Subcommittee will hold a legislative hearing titled “Reauthorizing Vital Health Programs for American Families.” I. H.R. 1058, THE “AUTISM COLLABORATION, ACCOUNTABILITY, RESEARCH, EDUCATION, AND SUPPORT ACT OF 2019” or THE “AUTISM CARES ACT OF 2019” A. Background Autism Spectrum Disorder (ASD) is a neurodevelopmental disorder that is defined by persistent and characteristic patterns of behavior and difficulties in social communication and interaction.1 As its name suggests, ASD represents a spectrum of neurodevelopmental conditions; while those diagnosed with ASD share similar characteristics, individuals may have different strengths, severity of conditions, and challenges associated with those conditions.2 The number of children diagnosed with ASD has risen dramatically over the years. For children born in 1992, approximately one in every 150 children was diagnosed with ASD.3 That number grew to one in every 59 children for children born in 2006.4 It is unclear how much of the increase is due to broader diagnostic criteria for ASD, increased efforts to diagnose, or a 1 National Institutes of Health, Autism Spectrum Disorder Fact Sheet (May 14, 2019) (www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Autism-Spectrum- Disorder-Fact-Sheet). 2 Id. 3 Centers for Disease Control and Prevention, Data & Statistics on Autism Spectrum Disorder (Apr. -

The Autism Biosolids Conundrum*
The Autism Biosolids Conundrum* *Despite overwhelming evidence that certain heavy metals, toxic organic chemicals and infectious agents play an important role in triggering autism and other environmental health problems, the U.S. Environmental Protection Agency supports land application of largely unmonitored concentrations of these contaminants in biosolids. David L. Lewis, Ph.D. Retired, U.S. EPA Office of Research and Development, National Exposure Research Laboratory (1968-2003), Athens, Georgia USA [email protected] ABSTRACT Before Congress passed the Clean Water Act of 1972, municipalities throughout the United States discharged hazardous municipal and industrial wastes directly into rivers and other waterways. Every chemical and biological agent linked to neurodevelopmental disorders, including those linked to “autism spectrum disorders” (ASDs), spilled into coastal waters and settled on the bottoms of the oceans. The solution to pollution was dilution. To comply with the Clean Water Act of 1972, President Carter created wastewater treatment plants throughout the United States to extract heavy metals and toxic organic chemicals from water and concentrate them in sewage sludges that were dumped offshore and buried in landfills. In 1988, Congress banned ocean dumping of sewage sludges because of their potential for causing vaccine-derived polio epidemics. Suddenly, high concentrations of every heavy metal, toxic organic chemical and vaccine-derived viruses linked to autism, including rubella and cytomegalovirus, had no place to go but land. The solution to pollution shifted from diluting pollutants in water to concentrating them on land at hundreds of thousands to millions of times higher concentrations, including on commercial farms that produce our nation’s food supplies. -

Strategic Framework Progress Report 2014
STRATEGIC FRAMEWORK PROGRESS REPORT 2014 Goal I: Infants, children and youth with I/DD have access to the supports and services they need to live in their family homes, to succeed in school and to partake in all of the experiences of childhood. Generally () () Strategy 1: Increase the availability of early intervention services that are provided in naturally occurring environments. Convention ● Multiple sessions on early intervention during The Arc's 2014 National Convention: Engaging Young Families: Diversity and Early Intervention & Providing Early Intervention Using a Primary Provider Model Federal Policy Advocacy ● Advocated for funding for domestic programs and tax policy to support adequate FY 2014 funding for both entitlement and discretionary programs benefitting children and adults with I/DD. ● Organized and led disability, faith, and child welfare organizations in meeting with Hill staff on strategy to engage others in advocacy on revenues and, in order to adequately fund critical disability programs, urged Congress to end the practice of treating corporations as foreign companies which results in lower taxes. ● Supported IDEA Fairness restoration to increase funding for IDEA. ● Urged Congress to enact legislation extending funding for national maternal, infant/early childhood program. State Office Operations - The Arc DC ● Coordinated 27 community-based instruction events for 388 students from 6 DC high schools Strategy 2: Increase the inclusion, participation and integration of students with proper accommodations in their neighBorhood schools, as well as in other puBlic and puBlicly general educational settings. Federal Policy Advocacy ● Developed recommendations for improving access to higher education for students with disabilities. ● Met with multiple senior White House officials on disability issues in higher education. -

(CFRI) Financing Focus: September 15, 2014
SAMHSA’s Center for Financing Reform & Innovations (CFRI) Financing Focus: September 15, 2014 National News 2 President Obama announces executive actions to improve military & veteran behavioral health services 2 Court to rehear federal Marketplace subsidy case 2 HHS awards $142.4 million in ACA expansion of care grants 2 CBO reduces federal Medicaid spending projection; CMS finds health care cost growth remains slow 2 Bill authorizes $1.3 billion for autism research and services through FY2019 3 HHS extends Healthcare.gov IT and administration contract 3 CDC awards $6 million for prescription drug overdose prevention 3 CVS ends tobacco sales 3 SAMHSA creates Office of Tribal Affairs and Policy 3 State News 4 HHS approves PA’s premium assistance waiver, AR releases draft waiver for health savings accounts 4 CMS approves MA’s new Marketplace, IL renews marketing contract, VT finalizes contractor shift 4 Oregon, Washington, and Wisconsin’s Marketplaces launch special enrollment periods 4 California audit recommends Medicaid substance abuse program improve fraud oversight 5 California: San Francisco launches mental health warm line 5 Florida: CMS approves Medicaid managed care renewal, continues overpayment review 5 Kentucky awards $19 million for juvenile substance abuse treatment 6 Washington allocates $30 million to end “psychiatric boarding,” requests Supreme Court stay 6 West Virginia: Court approves state plan to address staffing shortages at psychiatric hospitals 6 Financing Reports 6 The Center for Financing Reform and Innovations (CFRI) provides information, analysis, products, and technical assistance to address changes in the organization and financing of behavioral health care, and to guide Federal officials, States, Territories, Tribes, communities, and private payers on the most effective and efficient use of available resources to meet the prevention, treatment, and recovery support needs of the American public. -
Full Report — Applied Behavior Analysis Services in Kansas
KHI.ORG Informing Policy. Improving Health. APPLIED BEHAVIOR ANALYSIS SERVICES IN KANSAS KHI/19-21 MARCH 2019 Informing Policy. Improving Health. Copyright© Kansas Health Institute 2019. Materials may be reprinted with written permission Reference publication number KHI/19-21. 212 SW 8th Avenue | Suite 300 Topeka, Kansas | 66603-3936 785.233.5443 khi.org /KHIorg @KHIorg KHIorg APPLIED BEHAVIOR ANALYSIS SERVICES IN KANSAS MARCH 2019 Authors Sydney McClendon Madison Hoover, M.S. Steve Corbett, Ph.D. Wen-Chieh Lin, Ph.D. Acknowledgments The project team would like to thank Sandy Crawford from Easterseals Capper Foundation and Mike Wasmer from Autism Speaks for the expertise and guidance they contributed to this report. The project team also would like to thank Sharon Johnson and Kasey Sorrell from the Kansas Department of Health and Environment (KDHE) and Sam Philbern, previously of the Kansas Department for Aging and Disability Services (KDADS), for the assistance and background information they provided. For their assistance in disseminating the survey described in this report, the project team would like to thank the Kansas Association for Behavior Analysis (KansABA) and the Kansas Center for Autism Research and Training (K-CART). The project team also would like to thank Kari Bruffett from the Kansas Health Institute (KHI) for providing feedback and input in the development of this report. This project was funded in part by Easterseals Capper Foundation through an award from the Kansas Health Foundation. Easterseals Capper Foundation has been delivering high quality, individualized therapies, services and supports to children, teens and adults with disabilities across Kansas communities for 98 years. -

School Nurses Role in Managing Autism Spectrum Disorder in the School Setting
MICHIGAN ASSOCIATION OF SCHOOL NURSES – SCHOOL NURSES ROLE IN MANAGING AUTISM SPECTRUM DISORDER IN THE SCHOOL SETTING School Nurse’s Role in Managing Autism Spectrum Disorder in the School Setting MICHIGAN SCHOOL NURSE GUIDELINES AND RESOURCES Original Date of Issue: 2016 MICHIGAN ASSOCIATION OF SCHOOL NURSES – SCHOOL NURSES ROLE IN MANAGING AUTISM SPECTRUM DISORDER IN THE SCHOOL SETTING Foreword These guidelines contain recommendations for current best practices for the health service topic addressed. They have been reviewed by the School Nurse Practice Subcommittee of the Michigan Statewide School Nurse Task Force as a means to provide consistent and safe care to the students. Specific laws and regulations that direct school nursing practice or other health services are identified in the guidelines. There is no guarantee that the use of guidance in this document will lead to any particular result or outcome. The information in this document was researched in May, 2016. Purpose This document will provide guidelines and resources for the school nurse’s role in managing autism spectrum disorder (ASD) in the school setting. Overview Autism spectrum disorder (ASD) is a group of developmental disabilities that can cause significant social, communication and behavioral challenges as well as place substantial strain on family members (Siu & the U.S. Preventive Services Task Force, 2016). The Centers for Disease Control and Prevention (CDC) (2016a) provides information about the new standardized criteria from the American Psychiatric Association's Diagnostic and Statistical Manual, Fifth Edition (DSM-5) to help diagnose ASD. The new criteria have eliminated the previously separated categories of Asperger Syndrome, Child Disintegrative Disorder and Pervasive Developmental Disorder now consolidated under the term Autism Spectrum Disorder.