Distributed Cognition: Understanding Complex Sociotechnical Informatics
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Applications of Digital Image Processing in Real Time World
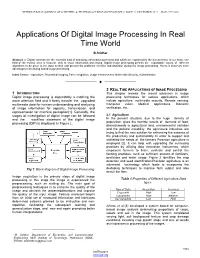
INTERNATIONAL JOURNAL OF SCIENTIFIC & TECHNOLOGY RESEARCH VOLUME 8, ISSUE 12, DECEMBER 2019 ISSN 2277-8616 Applications Of Digital Image Processing In Real Time World B.Sridhar Abstract :-- Digital contents are the essential kind of analyzing, information perceived and which are explained by the human brain. In our brain, one third of the cortical area is focused only to visual information processing. Digital image processing permits the expandable values of different algorithms to be given to the input section and prevent the problems of noise and distortion during the image processing. Hence it deserves more advantages than analog based image processing. Index Terms:-- Agriculture, Biomedical imaging, Face recognition, image enhancement, Multimedia Security, Authentication —————————— —————————— 2 REAL TIME APPLICATIONS OF IMAGE PROCESSING 1 INTRODUCTION This chapter reviews the recent advances in image Digital image processing is dependably a catching the processing techniques for various applications, which more attention field and it freely transfer the upgraded include agriculture, multimedia security, Remote sensing, multimedia data for human understanding and analyzing Computer vision, Medical applications, Biometric of image information for capacity, transmission, and verification, etc,. representation for machine perception[1]. Generally, the stages of investigation of digital image can be followed 2.1 Agriculture and the workflow statement of the digital image In the present situation, due to the huge density of population, gives the horrible results of demand of food, processing (DIP) is displayed in Figure 1. diminishments in agricultural land, environmental variation and the political instability, the agriculture industries are trying to find the new solution for enhancing the essence of the productivity and sustainability.―In order to support and satifisfied the needs of the farmers Precision agriculture is employed [2]. -
Health Informatics Principles
Health Informatics Principles Foundational Curriculum: Cluster 4: Informatics Module 7: The Informatics Process and Principles of Health Informatics Unit 2: Health Informatics Principles FC-C4M7U2 Curriculum Developers: Angelique Blake, Rachelle Blake, Pauliina Hulkkonen, Sonja Huotari, Milla Jauhiainen, Johanna Tolonen, and Alpo Vӓrri This work is produced by the EU*US eHealth Work Project. This project has received funding from the European Union’s Horizon 2020 research and 21/60 innovation programme under Grant Agreement No. 727552 1 EUUSEHEALTHWORK Unit Objectives • Describe the evolution of informatics • Explain the benefits and challenges of informatics • Differentiate between information technology and informatics • Identify the three dimensions of health informatics • State the main principles of health informatics in each dimension This work is produced by the EU*US eHealth Work Project. This project has received funding from the European Union’s Horizon 2020 research and FC-C4M7U2 innovation programme under Grant Agreement No. 727552 2 EUUSEHEALTHWORK The Evolution of Health Informatics (1940s-1950s) • In 1940, the first modern computer was built called the ENIAC. It was 24.5 metric tonnes (27 tons) in volume and took up 63 m2 (680 sq. ft.) of space • In 1950 health informatics began to take off with the rise of computers and microchips. The earliest use was in dental projects during late 50s in the US. • Worldwide use of computer technology in healthcare began in the early 1950s with the rise of mainframe computers This work is produced by the EU*US eHealth Work Project. This project has received funding from the European Union’s Horizon 2020 research and FC-C4M7U2 innovation programme under Grant Agreement No. -

Draft Common Framework for Earth-Observation Data
THE U.S. GROUP ON EARTH OBSERVATIONS DRAFT COMMON FRAMEWORK FOR EARTH-OBSERVATION DATA Table of Contents Background ..................................................................................................................................... 2 Purpose of the Common Framework ........................................................................................... 2 Target User of the Common Framework ................................................................................. 4 Scope of the Common Framework........................................................................................... 5 Structure of the Common Framework ...................................................................................... 6 Data Search and Discovery Services .............................................................................................. 7 Introduction ................................................................................................................................. 7 Standards and Protocols............................................................................................................... 8 Methods and Practices ............................................................................................................... 10 Implementations ........................................................................................................................ 11 Software ................................................................................................................................ -

Information- Processing Conceptualizations of Human Cognition: Past, Present, and Future
13 Information- Processing Conceptualizations of Human Cognition: Past, Present, and Future Elizabeth E Loftus and Jonathan w: Schooler Historically, scholars have used contemporary machines as models of the mind. Today, much of what we know about human cognition is guided by a three-stage computer model. Sensory memory is attributed with the qualities of a computer buffer store in which individual inputs are briefly maintained until a meaningful entry is recognized. Short-term memory is equivalent to the working memory of a computer, being highly flexible yet having only a limited capacity. Finally, long-term memory resembles the auxiliary store of a computer, with a virtually unlimited capacity for a variety of information. Although the computer analogy provides a useful framework for describing much of the present research on human cogni- tion, it is insufficient in several respects. For example, it does not ade- quately represent the distinction between conscious and non-conscious thought. As an alternative. a corporate metaphor of the mind is suggested as a possible vehiclefor guiding future research. Depicting the mind as a corporation accommodates many aspects of cognition including con- sciousness. In addition, by offering a more familiar framework, a corpo- rate model is easily applied to subjective psychological experience as well as other real world phenomena. Currently, the most influential approach in cognitive psychology is based on analogies derived from the digital computer. The information processing approach has been an important source of models and ideas but the fate of its predecessors should serve to keep us humble concerning its eventual success. In 30 years, the computer-based information processing approach that cur- rently reigns may seem as invalid to the humlln mind liSthe wax-tablet or tl'kphOlIl' switchhoard mmkls do todoy. -

Augmented Cognition for Bioinformatics Problem Solving
Augmented Cognition for Bioinformatics Problem Solving Olga Anna Kuchar and Jorge Reyes-Spindola Michel Benaroch Pacific Northwest National Laboratory Center for Creation and Management of Digital P.O. Box 999, 902 Battelle Blvd. Ventures Richland, WA, 99352 Martin J. Whitman School of Management Syracuse {olga.kuchar, jorge.reyes.spindola}@pnl.gov University, Syracuse, NY, 13244 [email protected] Abstract We describe a new computational cognitive model that has been developed for solving complex problems in bioinformatics. This model addresses bottlenecks in the information processing stages inherent in the bioinformatics domain due to the complex nature of both the volume and type of data and the knowledge required in solving these problems. There is a restriction on the amount of mental tasks a bioinformatician can handle when solving biology problems. Bioinformaticians are overwhelmed at the amount of fluctuating knowledge, data, and tools available in solving problems, but to create an intelligent system to aid in this problem-solving task is difficult because of the constant flux of data and knowledge; thus, bioinformatics poses challenges to intelligent systems and a new model needs to be created to handle such problem-solving issues. To create a problem-solving system for such an environment, one needs to consider the scientists and their environment, in order to determine how humans can function in such conditions. This paper describes our experiences in developing a complex cognitive system to aid biologists in knowledge discovery. We describe the problem domain, evolution of our cognitive model, the model itself, how this model relates to current literature, and summarize our ongoing research efforts. -
(IMIA) on Education in Health and Medical Informatics
This document has been published in Methods of Information in Medicine 39(2000), 267-277. Updated version October 2000, with corrections in footnote of section 4.2 Recommendations of the International Medical Informatics Association (IMIA) on Education in Health and Medical Informatics International Medical Informatics Association, Working Group 1: Health and Medical Informatics Education Abstract: The International Medical Informatics Association (IMIA) agreed on international recommendations in health informatics / medical informatics education. These should help to establish courses, course tracks or even complete programs in this field, to further develop existing educational activities in the various nations and to support international initiatives concerning education in health and medical informatics (HMI), particularly international activities in educating HMI specialists and the sharing of courseware. The IMIA recommendations centre on educational needs for health care professionals to acquire knowledge and skills in information processing and information and communication technology. The educational needs are described as a three-dimensional framework. The dimensions are: 1) professionals in health care (physicians, nurses, HMI professionals, ...), 2) type of specialisation in health and medical informatics (IT users, HMI specialists) and 3) stage of career progression (bachelor, master, ...). Learning outcomes are defined in terms of knowledge and practical skills for health care professionals in their role (a) as IT user and (b) as HMI specialist. Recommendations are given for courses/course tracks in HMI as part of educational programs in medicine, nursing, health care management, dentistry, pharmacy, public health, health record administration, and informatics/computer science as well as for dedicated programs in HMI (with bachelor, master or doctor degree). -

Is It Time for Cognitive Bioinformatics?
g in Geno nin m i ic M s ta & a P Lisitsa et al., J Data Mining Genomics Proteomics 2015, 6:2 D r f o Journal of o t e l DOI: 10.4172/2153-0602.1000173 o a m n r i c u s o J ISSN: 2153-0602 Data Mining in Genomics & Proteomics Review Article Open Access Is it Time for Cognitive Bioinformatics? Andrey Lisitsa1,2*, Elizabeth Stewart2,3, Eugene Kolker2-5 1The Russian Human Proteome Organization (RHUPO), Institute of Biomedical Chemistry, Moscow, Russian Federation 2Data Enabled Life Sciences Alliance (DELSA Global), Moscow, Russian Federation 3Bioinformatics and High-Throughput Data Analysis Laboratory, Seattle Children’s Research Institute, Seattle, WA, USA 4Predictive Analytics, Seattle Children’s Hospital, Seattle, WA, USA 5Departments of Biomedical Informatics & Medical Education and Pediatrics, University of Washington, Seattle, WA, USA Abstract The concept of cognitive bioinformatics has been proposed for structuring of knowledge in the field of molecular biology. While cognitive science is considered as “thinking about the process of thinking”, cognitive bioinformatics strives to capture the process of thought and analysis as applied to the challenging intersection of diverse fields such as biology, informatics, and computer science collectively known as bioinformatics. Ten years ago cognitive bioinformatics was introduced as a model of the analysis performed by scientists working with molecular biology and biomedical web resources. At present, the concept of cognitive bioinformatics can be examined in the context of the opportunities represented by the information “data deluge” of life sciences technologies. The unbalanced nature of accumulating information along with some challenges poses currently intractable problems for researchers. -

Information Processing & Technology Senior Syllabus
Information Processing & Technology Senior Syllabus 2004 To be studied with Year 11 students for the first time in 2005 Information Processing & Technology Senior Syllabus © The State of Queensland (Queensland Studies Authority) 2004 Copyright protects this work. Please read the Copyright notice at the end of this work. Queensland Studies Authority, PO Box 307, Spring Hill, Queensland 4004, Australia Phone: (07) 3864 0299 Fax: (07) 3221 2553 Email: [email protected] Website: www.qsa.qld.edu.au job 1545 CONTENTS 1 RATIONALE ..................................................................................................................... 1 2 GLOBAL AIMS................................................................................................................. 2 3 GENERAL OBJECTIVES................................................................................................. 3 Knowledge.................................................................................................................3 Research & development ...........................................................................................3 Attitudes and values...................................................................................................3 4 LANGUAGE EDUCATION STATEMENT..................................................................... 4 5 COURSE ORGANISATION ............................................................................................. 5 5.1 Time allocation........................................................................................................ -

Computation Vs. Information Processing: How They Are Different and Why It Matters
Studies in History and Philosophy of Science 41 (2010) 237–246 Contents lists available at ScienceDirect Studies in History and Philosophy of Science journal homepage: www.elsevier.com/locate/shpsa Computation vs. information processing: why their difference matters to cognitive science Gualtiero Piccinini a, Andrea Scarantino b a Department of Philosophy, University of Missouri St. Louis, 599 Lucas Hall (MC 73), One University Boulevard, St. Louis, MO 63121-4499, USA b Department of Philosophy, Neuroscience Institute, Georgia State University, PO Box 4089, Atlanta, GA 30302-4089, USA article info abstract Keywords: Since the cognitive revolution, it has become commonplace that cognition involves both computation and Computation information processing. Is this one claim or two? Is computation the same as information processing? The Information processing two terms are often used interchangeably, but this usage masks important differences. In this paper, we Computationalism distinguish information processing from computation and examine some of their mutual relations, shed- Computational theory of mind ding light on the role each can play in a theory of cognition. We recommend that theorists of cognition be Cognitivism explicit and careful in choosing notions of computation and information and connecting them together. Ó 2010 Elsevier Ltd. All rights reserved. When citing this paper, please use the full journal title Studies in History and Philosophy of Science 1. Introduction cessing, and the manipulation of representations does more -

What Are Computational Neuroscience and Neuroinformatics? Computational Neuroscience
Department of Mathematical Sciences B12412: Computational Neuroscience and Neuroinformatics What are Computational Neuroscience and Neuroinformatics? Computational Neuroscience Computational Neuroscience1 is an interdisciplinary science that links the diverse fields of neu- roscience, computer science, physics and applied mathematics together. It serves as the primary theoretical method for investigating the function and mechanism of the nervous system. Com- putational neuroscience traces its historical roots to the the work of people such as Andrew Huxley, Alan Hodgkin, and David Marr. Hodgkin and Huxley's developed the voltage clamp and created the first mathematical model of the action potential. David Marr's work focused on the interactions between neurons, suggesting computational approaches to the study of how functional groups of neurons within the hippocampus and neocortex interact, store, process, and transmit information. Computational modeling of biophysically realistic neurons and dendrites began with the work of Wilfrid Rall, with the first multicompartmental model using cable theory. Computational neuroscience is distinct from psychological connectionism and theories of learning from disciplines such as machine learning,neural networks and statistical learning theory in that it emphasizes descriptions of functional and biologically realistic neurons and their physiology and dynamics. These models capture the essential features of the biological system at multiple spatial-temporal scales, from membrane currents, protein and chemical coupling to network os- cillations and learning and memory. These computational models are used to test hypotheses that can be directly verified by current or future biological experiments. Currently, the field is undergoing a rapid expansion. There are many software packages, such as NEURON, that allow rapid and systematic in silico modeling of realistic neurons. -
Informatics: History, Theory, Concepts and Competencies
Informatics: History, Theory, Concepts and Competencies Charlotte Seckman, PhD, RN-BC Assistant Professor, Course Director Nursing Informatics Specialist University of Maryland School of Nursing Objectives • Review informatics history, definitions, theory and concepts as it relates to the healthcare environment and role of the professional nurse. • Discuss the role of nurses as knowledge workers. • Differentiate between computer literacy versus information literacy. • Compare and contrast the informatics competencies for each level of nursing education. What is Informatics? • The term informatics was derived from the French term informatique, which means to refer to the computer milieu (Saba, 2001). • Some trace this back to a Russian document published in 1968 • Europeans first coined the term in the 1980’s • Application to various disciplines What is Informatics? • Information Science • discipline that studies information processing • Information System • hardware and software • Information • general term for Technology information processing with computers • Information • Process of turning data into Management information and knowledge • Informatics • combines the study of information processing and computers What is Nursing Informatics? Classic Definition • Nursing Informatics is a combination of computer science, information science and nursing science designed to assist in the management and processing of nursing data, information, and knowledge to support the practice of nursing and the delivery of nursing care (Graves & Corcoran, -
Step-By-Step Guide to Vulnerability Hotspots Mapping: Implementing the Spatial Index Approach
Step-by-Step Guide to Vulnerability Hotspots Mapping: Implementing the Spatial Index Approach Developed by the Center for International Earth Science Information Network (CIESIN), The Earth Institute, Columbia University Under contract with TetraTech/ARD for the US Agency for International Development (USAID) Planning for Resilience in East Africa through Policy, Adaptation, Research, and Economic Development (PREPARED) Project November 2015 1 Authors: Malanding S Jaiteh, PhD Tricia Chai-Onn Valentina Mara Alex de Sherbinin, PhD Acknowledgements This work was performed under contract with TetraTech/ARD for the US Agency for International Development (USAID) Planning for Resilience in East Africa through Policy, Adaptation, Research, and Economic Development (PREPARED) project. The work also benefited greatly from vulnerability mapping efforts under the USAID-funded African and Latin American Resilience to Climate Change (ARCC) project. Slides on Installing and configuring R adapted from R-Cran available at: http://cran.r-project.org/bin/windows/base/rw-FAQ.html We wish to acknowledge the contributions of Dr. idris Bexi Wasama, University of Djibouti, who reviewed the draft manual while visiting CIESIN as a Hubert H. Humphrey Fellow through the University of California, Davis. Cover image by Jeremy Chevrier, USAID Sahel Regional Office. Citing this Guide CIESIN (Center for International Earth Science Information Network), Columbia University. (2015). A Step-by-Step Guide to Vulnerability Hotspots Mapping: Implementing the Spatial Index