Disputed Dimensions of Risk: a Public School Controversy Over AIDS
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Gerald R. Ford Administration White House Press Releases
MARCq 24, 1976 '-. Office of the White House Press Secretary ~ NOTICE TO THE PRESS Participants in the 3:30 p. m. ~eeting with Secretary Mathews and the President: Eugene W. Fowinkle, H.D., Commissioner of Public Health, Tennessee Department of Public Health, Nashville. George Hardy, M.D., Health Officer, Jefferson County Health Department, Birmingham, Alabama. Albert G. Randell, M.D., Director of Public Health, City of Houston, Texas. Charles Hall, M.D., Charleston, West Virginia. Merritt B. Lowe, M.D., Greenfield, Massachusetts. Raymond Holden, M.D., Washington, D.C., chairman, A.M.A. Morton S. Hilbert, MPH, CE, Chairman, Department of Enviro,nmental and Industrial Health, School of Public Health, University of Michigan, Ann Arbor. Maurice R. Hilleman, Ph.D., Vice President, Merck, Sharp and Dohme Research Laboratories, West Point, PAD John F. Lawlis, Ph.D., Vice President of Biological Operations, Menell-National Laboratories, Swiftwater, PAD Eugene A. Timm, Ph.D., Asst. Division Director, Quality Control and Government Regulations, Parke, Davis and Company, Detroit, Michigan. Alan Gray, Ph.D., Director of Biologics, Merck, Sharp and Dohme, West Point, PAD Alan Bernstein, Ph.D., Managing Director, Wyeth Laboratories, Inc., Marietta, Pennsylvania. Dr. Fred M. Davenport, Department of Epidemiology, University of Michigan School of Public Health, Ann Arbor. Reul A. Stallones, M.D., Dean, University of Texas School of Public Health, Houston. Dr. Floyd Denny, University of North Carolina Department of Pediatrics, Chapel Hill. Edwin Kilbourne, M.D., Chairman, Department of Microbiology, Mt. Sinai School of Medicine, City University of New York. Saul Krugman, M.D., Department of Pediatrics, New York University School of Medicine. -
![In Memoriam: David Judson Sencer, a Public Health Giant [Announcer] This Program Is Presented by the Centers for Disease Control and Prevention](https://docslib.b-cdn.net/cover/0411/in-memoriam-david-judson-sencer-a-public-health-giant-announcer-this-program-is-presented-by-the-centers-for-disease-control-and-prevention-1310411.webp)
In Memoriam: David Judson Sencer, a Public Health Giant [Announcer] This Program Is Presented by the Centers for Disease Control and Prevention
In Memoriam: David Judson Sencer, A Public Health Giant [Announcer] This program is presented by the Centers for Disease Control and Prevention. [Dr. Peter Drotman] Hi, I’m Dr. Peter Drotman, Editor-in-Chief of Emerging Infectious Diseases. Today, I’m talking with Dr. Jeffrey Koplan, Director of the Emory Global Health Institute at Emory University. He was Director of CDC in 2001, the time that I became the Editor-in-Chief of EID. Dr. Koplan’s In Memoriam piece appears in CDC’S journal, Emerging Infectious Diseases, and he discusses the life and career of Dr. David Sencer, former Director of CDC and a public health giant whom we both knew. Jeff, welcome. [Dr. Jeffrey Koplan] Thank you; it’s great to be here. [Dr. Peter Drotman] How and when did you initially meet and get to know David Sencer? [Dr. Jeffrey Koplan] Well, it’s hard to believe, but as an EIS Officer, Epidemic Intelligence Service Officer, coming to CDC in 1972, I served in the small pox eradication program and the then director of that program, Bill Fagey, was a good friend of Dr. Sencer’s, and Dr. Sencer, as many folks know, was a huge advocate and supporter of small pox eradication, so I kind of was a kid on the sidelines, but Dr. Sencer was very good at nurturing and recognizing young people and so, from my EIS years, I was aware of and knew Dr. David Sencer. [Dr. Peter Drotman] Now, getting behind that program to begin with was actually a more courageous act then we appreciate nowadays. -

Opening the Schoolhouse Door to the Aids Virus: Policymaking, Politics, and Personality in a Queens County Courtroom, 1985-86
OPENING THE SCHOOLHOUSE DOOR TO THE AIDS VIRUS: POLICYMAKING, POLITICS, AND PERSONALITY IN A QUEENS COUNTY COURTROOM, 1985-86 R. KYLE ALAGOOD Public health policy operates in a democratic paradox. The police power exists to protect individuals from harms they cannot themselves fend off, but every restriction of individual freedom in the name of public health runs against constitutionally protected individual rights. Public health officials are damned if they do, damned if they don’t. But policymakers can take steps to avoid litigation by partnering with the public in contentious public health decisions. District 27 Community School Board v. Board of Education and events leading to the lawsuit exemplify the democratic paradox. A largely overlooked case, District 27 is one of the most important early AIDS cases. It was the first to consider the disease in depth. The case established the dearth of evidence that AIDS could be transmitted casually. And District 27 signaled that AIDS did not demand and law did not permit discrimination. This article dusts off District 27 and uses New York City’s policy-making process as a case study for public health policymaking in an epidemic. It suggests ways lawyers and policymakers can balance secrecy and transparency against democratic ideals, as well as how valuing the public and allowing public input enhances policy decisions. INTRODUCTION ......................................................................................................................................... 260 I. DISTRICT 27 IN CONTEXT: -

Protecting Public Health in New York City: 200 Years of Leadership
PROTECTING PUBLIC HEALTH IN NEW YORK CITY: 200 YEARS OF LEADERSHIP 1805-2005 T HE N EW Y ORK C ITY D EPARTMENT OF H EALTH AND M ENTAL H YGIENE Protecting Public Health in New York City: 200 Years of Leadership ~ 1805-2005 Michael R. Bloomberg Mayor Thomas R. Frieden, MD, MPH Commissioner April 2005 marks the bicentennial of the New York City Board of Health, the predecessor of the New York City Department of Health and Mental Hygiene. New York City’s illustrious history of public health leadership began in the early 1800s, when the city controlled epidemics of Yellow Fever and cholera. In the early 1900s, the Department opened the first public health laboratory that applied bacteriological knowledge to prevent and control disease. In the late 1900s, the Department implemented model programs to fight new and re-emerging infectious diseases. And in the century just begun, we have launched programs to prevent and control major chronic diseases. The Board’s 200th anniversary is an appropriate time for us to review the many public health challenges that the Board and the Department have met over the years, and to reflect on the lessons these experiences hold for our future. ~ Thomas R. Frieden, MD, MPH Commissioner New York City Department of Health and Mental Hygiene { 1805 – 2005} T ABLE OF C ONTENTS 1805-1865: Fighting Yellow Fever and Cholera 3 1866-1885: The Birth of the New York City Department of Health 11 1886-1913: Immigration, the Bacteriological Revolution, and Hermann Biggs 17 1914-1922: The Health Department Modernizes 25 1923-1930: -
An Analysis of Competing Images and Arguments in the AIDS Controversy
DOCUMENT RESUME ED 289 189 CS 505 785 AUTHOR Gilder, Eric TITLE A Clash of Symbols: An Analysis of Competing Images and Arguments in the AIDS Controversy. PUB DATE Nov 87 NOTE 38p.; Paper presented at the Annual Meeting of the Speech Communication Association (73rd, Boston, MA, November 5-8, 1987). PUB TYPE Viewpoints (120) Speeches/Conference Papers (150) EDRS PRICE MF01/PCO2 Plus Postage. DESCRIPTORS *Acquired Immune Deficiency Syndrome; Communicable Diseases; Conflict; Current Events; Medicine; *Models; Moral Issues; Political Issues; Problem Solving; Religious Conflict; Scientific Research; Social Change; Social Discrimination; *Social Problems; *Symbolic Language; Traditionalism; Values ABSTRACT Efforts to contain the spread of Acquired Immune Deficiency Syndrome (AIDS) have been slowed by numerous arguing factions, political, religious, and medical, all of which perceive the AIDS epidemic through a different set of symbols. The images can be more easily understood using Kenneth Boulding's Threat, Integry, and Exchange (or TIE) model. The triangular model suggests that interactions based on threat images are destructive, founded on one group subjugating another. Groups who base their actions on threat images include Christian fundamentalists, who conclude that the disease is an act of divine retribution; the medical community, which sees AIDS as a threat to its authority and ability to cure disease, and some gay groups, who see AIDS as a threat to their political autonomy and sexual freedom. Action based on exchange images are more productive, including spending tax dollars on AIDS research, while action based on integrative images is the most productive, encompassing the acknowledgement of identity in relation to others. Churches that have welcomed gays into their membership and groups that have been formed to deal specifically with the AIDS issue fall into this category. -

OBITUARIES for the Full Versions of Articles in This Section See Bmj.Com
OBITUARIES For the full versions of articles in this section see bmj.com David Sencer Guided and built the US public health agency David Sencer, who served as head of the US Centers of Sencer’s name being veterans in differ- for Disease Control and Prevention (CDC) for 11 linked with his achieve- ent cities became ill years from 1966 to 1977, was “a giant in public ments in building CDC with a pneumonia health” who lost the job he loved for doing the right into an international that didn’t respond thing—trying to immunise the American public scientific powerhouse to powerful antibiot- against an epidemic. and in providing the ics, and 29 died. The “My dad’s best accomplishment was not a sin- administrative, finan- press and the public gle achievement but building the CDC commu- cial, and personnel complained that it nity, which reaches around the world. He always support for the eradi- was taking too long put people first, and he knew what was going on cation of smallpox, to find the cause. everywhere. He’d drop in on people and ask what too often it is linked to CDC officers dis- they were doing—and he’d remember,” said his CDC’s response to two covered that the vet- son Stephen, general counsel and vice president unusual disease out- erans had attended of Emory University, Atlanta, Georgia. breaks. an American Legion In January and Feb- convention at a hotel Eradication of smallpox ruary of 1976 about in Philadelphia. They Thomas Frieden, the current head of CDC, called 200 recruits at the Fort Dix army base in New Jer- found that the pneumonia was caused by a newly Sencer a public health giant and said that two sey developed respiratory infections. -
David Sencer, the Well-Being of Others Came First
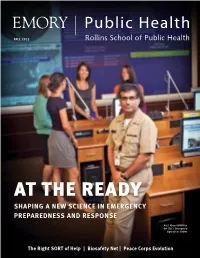
FALL 2011 AT THE READY SHAPING A NEW SCIENCE IN EMERGENCY PREPAREDNESS AND RESPONSE Ali S. Khan 00MPH in the CDC’s Emergency Operations Center The Right SORT of Help | Biosafety Net | Peace Corps Evolution Editor Pam Auchmutey Art Director Erica Endicott Director of Photography Bryan Meltz Photo Contributors Ann Borden Kay Hinton Jack Kearse Caroline Rumley Editorial Contributors Patrick Adams 09MPH Jennifer Johnson Carol Pinto Tarvis E. Thompson Kay Torrance Robin Tricoles Circulation and Finance Manager Carol Pinto Print Production Manager Stuart Turner Executive Director, Health Sciences Publications Karon Schindler Peace Be With You In 1961, President John F. Kennedy established the Peace Corps to promote peace and friendship Associate Dean for Development and External Relations, Rollins around the world. Fifty years later, Rollins’ Master International (MI) Program, which prepares School of Public Health students for Peace Corps service, is the only program in the nation that matches MI students Kathryn H. Graves, MEd, with Returned Peace Corps Volunteers (RPCVs) to work with refugee populations. Pictured above 93MPH are several RPCVs, who comprise a sizable portion of the student body and exemplify the Peace Dean, Rollins School of Corps’ goal to increase collaboration. Among the RPCVs are the Paul D. Coverdell Fellows, who Public Health manage the MI program. To learn more about Rollins and the Peace Corps, turn to page 18. James W. Curran, MD, MPH On the Cover Ali S. Khan 00MPH relies on Rollins students The iPad edition of Emory to help staff the CDC’s Emergency Operations Center Public Health is available by during disease outbreaks. -

Highlights in Public Health Landmark Articles from the MMWR 1961–1996
Highlights in Public Health Landmark Articles from the HighlightsHighlights inin PublicPublic HealthHealth MMWR 1961–1996 Landmark Articles from theMMWR 1961–1996 First issue of MMWR published by CDC Highlights in Public Health Landmark Articles from the MMWR 1961–1996 Editors Richard A. Goodman, M.D., M.P.H. Karen L. Foster, M.A. Michael B. Gregg, M.D. with a Foreword by George D. Lundberg, M.D. Editor, Journal of the American Medical Association U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention Atlanta, Georgia 30333 ii Layout and Desktop Publishing Peter M. Jenkins Cover Design Caran R. Wilbanks and Peter M. Jenkins Editing and Production Morie M. Higgins Peter M. Jenkins David C. Johnson Darlene D. Rumph-Person Teresa F. Rutledge Caran R. Wilbanks The name of and logo for MMWR are trademarked by the Centers for Disease Control and Prevention. Use of trade names and commercial sources is for identification only and does not constitute endorsement by the Centers for Disease Control and Prevention or the U.S. Department of Health and Human Services. Because MMWR is a publication of the U.S. government, its articles are in the public domain and may be reprinted without permission; proper credit, however, should be acknowledged. Citations should be to the originally published article OR to the reprinted article/new editorial note combination. The MMWR series is available free of charge on the World-Wide Web at <http://www.cdc.gov/epo/mmwr/mmwr.html>. Paid paper-copy subscriptions are available from the Superintendent of Documents, U.S. -

1976/03/24 - Swine Influenza Immunization Program Meeting” of the James M
The original documents are located in Box 57, folder “1976/03/24 - Swine Influenza Immunization Program Meeting” of the James M. Cannon Files at the Gerald R. Ford Presidential Library. Copyright Notice The copyright law of the United States (Title 17, United States Code) governs the making of photocopies or other reproductions of copyrighted material. Gerald Ford donated to the United States of America his copyrights in all of his unpublished writings in National Archives collections. Works prepared by U.S. Government employees as part of their official duties are in the public domain. The copyrights to materials written by other individuals or organizations are presumed to remain with them. If you think any of the information displayed in the PDF is subject to a valid copyright claim, please contact the Gerald R. Ford Presidential Library. Digitized from Box 57 of the James M. Cannon Files at the Gerald R. Ford Presidential Library INFLUENZA MEETING WITH THE PRESIDENT Wednesday, ~1arch 24, 1976 3:30 p.m. Roosevelt Room THE WHITE HOUSE WASHINGTON March 24, 1976 MEETING ON SWINE INFLUENZA IMMUNIZATION PROGRAM Wednesday, March 24, 1976 3:30p.m. (one hour) The Cabinet Room \. From: Jim Cannon\ \'r.."" ! ·~;.'! . ""'\. \i I. PURPOSE To discuss with influenza experts, medical professionals, public health officers, pharmaceutical executives, and public officials plans for a Federal initiative to immunize all Americans against swine influenza. II. BACKGROUND, PARTICIPANTS & PRESS PLAN A. Background: On Monday, you met with Secretary Mathews, Dr. Ted Cooper, Jim Lynn, Paul O'Neill, Jim Cavanaugh and me about a possible outbreak of swine influenza this coming winter. -

Ebola and COVID-19: Lessons from and for the Faith Community
Public Health, Religion, and Spirituality Bulletin 13 Spring/Summer 2020, Issue 2, pp. 13–14 [Online 27 May 2020, Article A011 ISSN 2689-7024] https://publichealthrs.org/a011/ Ebola and COVID-19: Lessons from and for the Faith Community Ellen Idler,[1] John Blevins,[2] and Mimi Kiser[3] not-so-distant mirror of the current pandemic is provided by the 2014-2015 A West African Ebola outbreak. We the public now have an easy way to inspect this Ebola mirror and ponder its lessons. As of Thursday February 6, 2020, the Centers for Disease Control and Prevention (CDC) has launched an online digital version of its acclaimed Ebola outbreak exhibit, previously on physical display in the CDC’s David Sencer Museum in Atlanta during 2017 and 2018. The digital project, a joint effort of the CDC with students, faculty, and staff of Georgia State University and Emory University, has catalogued every object and installation in the original exhibit, and includes additional materials such as interviews with actors in the medical, public health, and faith communities of Liberia, Sierra Leone, and Guinea. You can access the digital exhibit here: http://cdcmuseum.org/ At the February digital launch event, one of the CDC scientists who led the Ebola response spoke about her pride in the museum’s exhibit, and how much she had enjoyed giving occasional tours for CDC Museum exhibit showing annotated visitors. She also mentioned that one of her Bible and Quran used at Focus 1000 meeting favorite parts of the exhibit was the section about of faith leaders, Sierra Leone. -

Recalibrating Vaccination Laws
RECALIBRATING VACCINATION LAWS EFTHIMIOS PARASIDIS INTRODUCTION ............................................................................................. 2154 I. PLACING THE VACCINE ACT IN HISTORICAL CONTEXT ..................... 2166 A. Manufacturer’s Liability for Vaccine-Related Injuries ............. 2167 1. The Cutter Incident and Vaccine-Induced Polio ................. 2167 2. Cancer and SV40 Contaminated Polio Vaccines ................. 2172 3. Products Liability Claims for Vaccine-Related Injuries ...... 2178 4. Vaccine-Related Injuries and Market Share Liability ......... 2186 B. The 1976 Swine Flu Vaccine: Industry Demands Government Indemnification for Vaccine-Related Injuries ........................... 2192 C. 1980s Public Health Politics: Portraying the FDA as a Bureaucratic Hindrance to Health and Safety .......................... 2200 II. THE VACCINE ACT FRAMEWORK ...................................................... 2208 A. National Vaccine Program: Goals, Funding, and Administration ........................................................................... 2209 B. The National Vaccine Injury Compensation Program .............. 2211 C. The Vaccine Act’s Limits on Tort Claims Against Vaccine Manufacturers ........................................................................... 2219 III. MODERNIZING THE VACCINE ACT ..................................................... 2221 A. Adjusting the Requirements for Adverse Event Reporting and Post-Market Analysis of Vaccine Safety and Efficacy ............... 2222 B. Predicating -

Evans 1977-79 004.Pdf
.• ! NOV 1,3 1919 I , i TO: ~~ FROM' . A••S E'vans . M .'f) ~~~0J~ ~4- ~1A t, ~~~~~~ ~I~.t. N5~ ~~/k~iJ., ;.O~ ~, ~ t, c.» c.. ,(. r 1j~~-~ . ~.~~- ~~~ #e ../ YaleUniversity NewHaven,Connecticttto65IO SCHOOL OF MEDICINE Department of Epidemiology and Public Health 60 College Street November 7, 1979 Mr. Mike Wallace "60 Minutes Program," CBS News Columbia Broadcasting System 524 W. 57th Street New York City, New York 10019 Dear Mr. Wallace: If the bias, lack of scientific objectivity, sensationalism, and search for a guilty culprit characterize ot~er presentations as it did your report on "Swine Influenza," then I can place little trust in anything "60 Hinutes" reports. In fact, I am keenly disappointed in you and your network for irresponsible journalism. Your report has undermined the confidence of the public in influenza immunization as well as in other immunization programs. You have implied that the decision to give swine flu vaccine was unwarranted whereas there was, and is, sound scientific grounds for that decision. You have undermined the public's confidence in an outstanding organization, the Center for Disease Control and made Dr. David Sencer, its former Director ( a guilty culprit. The facts of the case are: 1. There were 293 cases of Guil1ain-BarreSyndrome (GBS) in persons re- ceiving influenza immunization and 264 in unvaccinated persons in the period October 1, 1976-January 18, 1977 and 10 deaths in each group (Morbidity and Mortality Report, CDC, January 21, 1977). This is not to say that there was not an increased risk of GBS in the first 8 weeks after immunization as compared to unimmunized persons, but the overall number of cases and deaths were very similar.