Download Article (PDF)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

308-316/ 30 April, 2016 ISSN 2322-4134 ©2016 IJFAS
International Journal of Farming and Allied Sciences Available online at www.ijfas.com ©2016 IJFAS Journal-2016-5-4/308-316/ 30 April, 2016 ISSN 2322-4134 ©2016 IJFAS Identification of Gaeumannomyces Graminis Varities by Specific Primers and Morphological Characteristics Mariam Yosefvand1*, Saeid Abbasi1, Kianoosh Chagha-Mirza2, Sohbat Bahram- Nezhad2 1. Department of plant protection, university of Razi, Kermanshah, Iran. 2. Department of Agronomy and Plant Breeding, university of Razi, Kermanshah, Iran Corresponding author: Mariam yosefvand ABSTRACT: Take-all disease caused by the fungus Gaeumannomyces graminis (Sacc.) Arx & Oliver var. tritici Walker is the most devastating root disease of cereals throughout the world. it has been also reported from different areas across Iran such as Kermanshah Province. During 2010-2011, three thousand four hudred twenty six diseased samples showing white head were collected from more than 300 wheat and barley fields visited in various parts of Kermanshah province. Pathogencity test of isoliated on wheat and oat was evaluated which all isolates causes disease on wheat. Based on morphological methods, all of isolates identified as G. graminis.var. tritici. Specific primers was used for identification of G. graminis . Two sets of primer pairs (NS5: GGT-RP and NS5: GGA-RP) were used to confirm identification and differentiation of the varities. This stage of testing showed that all isolates are G. g. var. tritici. The result also showed that G. g. var. avena wasn’t in collected isolates Keywords: Take all, Gaeomanomyces graminis, bio diversity, RAPD INTRODUCTION Caused by Gaeumannomyces graminis var. tritici, take-all disease is a fungal disease which starts as a root rot, causing stunting and nutrient-deficiency symptoms in the tops, and progresses upward into the bases of the stems where it can then disrupt the flow of water to the tops, causing premature death of the plant (Cook, 2003; Elliott and Landschoot, 1991). -

Documenta Praehistorica XLVI
UNIVERSITY OF LJUBLJANA FACULTY OF ARTS DEPARTMENT OF ARCHAEOLOGY DocumentaDocumenta PraehistPraehistoricaorica XLVIXLVI Documenta Praehistorica XLVI EDITOR Mihael Budja ISSN 1408–967X (Print) ISSN 1854–2492 (Online) LJUBLJANA 2019 DOCUMENTA PRAEHISTORICA XLVI (2019) Urednika/Editors: Prof. Dr. Mihael Budja, urednik/editor, [email protected] Bojan Kambič, tehnični urednik/technical editor, [email protected] Uredniški odbor/Editorial board: Maja Andrič, Institute of Archaeology, ZRC SAZU, Ljubljana, Slovenia Mihael Budja, University of Ljubljana, Faculty of Arts, Slovenia Canan Çakirlar, University of Groningen, Faculty of Arts, Netherlands Ekaterina Dolbunova, The State Hermitage Museum, The department of archaeology of Eastern Europe and Siberia, Saint-Petersburg, Russian Federation Ya-Mei Hou, Institute of Vertebrate Paleontology and Paleoanthropolgy, Chinese Academy of Sciences, Beijing, China Dimitrij Mlekuž Vrhovnik, University of Ljubljana, Faculty of Arts, Slovenia; Institute for the protection of the cultural heritage of Slovenia, Ljubljana, Slovenia Simona Petru, University of Ljubljana, Faculty of Arts, Slovenia Žiga Šmit, University of Ljubljana, Faculty of mathematics and physics, Slovenia Katherine Willis, University of Oxford, United Kingdom Andreja Žibrat Gašparič, University of Ljubljana, Faculty of Arts, Slovenia To delo je ponujeno pod licenco Creative Commons Priznanje avtorstva-Deljenje pod enakimi pogoji 4.0 Mednarodna licenca/This work is licensed under a Creative Commons Attribution- ShareAlike 4.0 International License. Založila in izdala/Published by: Znanstvena založba Filozofske fakultete, Univerza v Ljubljani/ Ljubljana University Press, Faculty of Arts ([email protected]; www.ff.uni-lj.si) Za založbo/For the publisher: Prof. Dr. Roman Kuhar, dekan Filozofske fakultete Naslov uredništva/Address of Editorial Board: Oddelek za arheologijo, Filozofska fakulteta, Univerza v Ljubljani, Aškerčeva 2, 1001 Ljubljana, p.p. -

Quake Hits Iran-Iraq Border Region 11 December 2017
Quake hits Iran-Iraq border region 11 December 2017 The Kermanshah quake left more than 12,000 people injured and thousands homeless, and came at the start of the cold season in the mountainous region. The area has seen some 1,200 aftershocks since last month, most of them below magnitude 4, Mehr news agency reported on Saturday. Monday's tremor sparked panic among the population of Kermanshah, causing heavy traffic in the city as citizens rushed to the street, local media reported. The epicentre of a 5.4-strength earthquake December Iran sits on top of two major tectonic plates and 11, 2017 was in Iraq's Halabja, some 20 kilometres (12.5 sees frequent seismic activity. miles) north of the Iranian town of Ezgeleh in Kermanshah province On December 1, a magnitude 6.0 earthquake hit Iran's eastern province of Kerman, with no casualties. A tremor shook Kermanshah province in western © 2017 AFP Iran near Iraq's border Monday, causing panic a month after a major quake killed hundreds of people there, state media and officials said. Two hours after the tremor the state broadcaster, quoting the head of the crisis management cell in Kermanshah province, said there were no reports of damage or deaths. The University of Tehran's seismology centre said a 6.0-magnitude quake shook the area while the US Geological Survey put it at 5.4. The epicentre was in Iraq's Halabja, some 20 kilometres (12.5 miles) north of the Iranian town of Ezgeleh in Kermanshah province. On November 12 a major 7.3-magnitude quake killed 620 people in Kermanshah province, according to the latest death toll provided Monday by Tasnim news agency. -

Spatial Epidemiology of Rabies in Iran
Aus dem Friedrich-Loeffler-Institut eingereicht über den Fachbereich Veterinärmedizin der Freien Universität Berlin Spatial Epidemiology of Rabies in Iran Inaugural-Dissertation zur Erlangung des Grades eines Doktors der Veterinärmedizin an der Freien Universität Berlin vorgelegt von Rouzbeh Bashar Tierarzt aus Teheran, Iran Berlin 2019 Journal-Nr.: 4015 'ĞĚƌƵĐŬƚŵŝƚ'ĞŶĞŚŵŝŐƵŶŐĚĞƐ&ĂĐŚďĞƌĞŝĐŚƐsĞƚĞƌŝŶćƌŵĞĚŝnjŝŶ ĚĞƌ&ƌĞŝĞŶhŶŝǀĞƌƐŝƚćƚĞƌůŝŶ ĞŬĂŶ͗ hŶŝǀ͘ͲWƌŽĨ͘ƌ͘:ƺƌŐĞŶĞŶƚĞŬ ƌƐƚĞƌ'ƵƚĂĐŚƚĞƌ͗ WƌŽĨ͘ƌ͘&ƌĂŶnj:͘ŽŶƌĂƚŚƐ ǁĞŝƚĞƌ'ƵƚĂĐŚƚĞƌ͗ hŶŝǀ͘ͲWƌŽĨ͘ƌ͘DĂƌĐƵƐŽŚĞƌƌ ƌŝƚƚĞƌ'ƵƚĂĐŚƚĞƌ͗ Wƌ͘<ĞƌƐƚŝŶŽƌĐŚĞƌƐ ĞƐŬƌŝƉƚŽƌĞŶ;ŶĂĐŚͲdŚĞƐĂƵƌƵƐͿ͗ ZĂďŝĞƐ͕DĂŶ͕ŶŝŵĂůƐ͕ŽŐƐ͕ƉŝĚĞŵŝŽůŽŐLJ͕ƌĂŝŶ͕/ŵŵƵŶŽĨůƵŽƌĞƐĐĞŶĐĞ͕/ƌĂŶ dĂŐĚĞƌWƌŽŵŽƚŝŽŶ͗Ϯϴ͘Ϭϯ͘ϮϬϭϵ ŝďůŝŽŐƌĂĨŝƐĐŚĞ/ŶĨŽƌŵĂƚŝŽŶĚĞƌĞƵƚƐĐŚĞŶEĂƚŝŽŶĂůďŝďůŝŽƚŚĞŬ ŝĞĞƵƚƐĐŚĞEĂƚŝŽŶĂůďŝďůŝŽƚŚĞŬǀĞƌnjĞŝĐŚŶĞƚĚŝĞƐĞWƵďůŝŬĂƚŝŽŶŝŶĚĞƌĞƵƚƐĐŚĞŶEĂƚŝŽŶĂůďŝͲ ďůŝŽŐƌĂĨŝĞ͖ ĚĞƚĂŝůůŝĞƌƚĞ ďŝďůŝŽŐƌĂĨŝƐĐŚĞ ĂƚĞŶ ƐŝŶĚ ŝŵ /ŶƚĞƌŶĞƚ ƺďĞƌ фŚƚƚƉƐ͗ͬͬĚŶď͘ĚĞх ĂďƌƵĨďĂƌ͘ /^E͗ϵϳϴͲϯͲϴϲϯϴϳͲϵϳϮͲϯ ƵŐů͗͘ĞƌůŝŶ͕&ƌĞŝĞhŶŝǀ͕͘ŝƐƐ͕͘ϮϬϭϵ ŝƐƐĞƌƚĂƚŝŽŶ͕&ƌĞŝĞhŶŝǀĞƌƐŝƚćƚĞƌůŝŶ ϭϴϴ ŝĞƐĞƐtĞƌŬŝƐƚƵƌŚĞďĞƌƌĞĐŚƚůŝĐŚŐĞƐĐŚƺƚnjƚ͘ ůůĞ ZĞĐŚƚĞ͕ ĂƵĐŚ ĚŝĞ ĚĞƌ mďĞƌƐĞƚnjƵŶŐ͕ ĚĞƐ EĂĐŚĚƌƵĐŬĞƐ ƵŶĚ ĚĞƌ sĞƌǀŝĞůĨćůƚŝŐƵŶŐ ĚĞƐ ƵĐŚĞƐ͕ ŽĚĞƌ dĞŝůĞŶ ĚĂƌĂƵƐ͕ǀŽƌďĞŚĂůƚĞŶ͘<ĞŝŶdĞŝůĚĞƐtĞƌŬĞƐĚĂƌĨŽŚŶĞƐĐŚƌŝĨƚůŝĐŚĞ'ĞŶĞŚŵŝŐƵŶŐĚĞƐsĞƌůĂŐĞƐŝŶŝƌŐĞŶĚĞŝŶĞƌ&Žƌŵ ƌĞƉƌŽĚƵnjŝĞƌƚŽĚĞƌƵŶƚĞƌsĞƌǁĞŶĚƵŶŐĞůĞŬƚƌŽŶŝƐĐŚĞƌ^LJƐƚĞŵĞǀĞƌĂƌďĞŝƚĞƚ͕ǀĞƌǀŝĞůĨćůƚŝŐƚŽĚĞƌǀĞƌďƌĞŝƚĞƚǁĞƌĚĞŶ͘ ŝĞ tŝĞĚĞƌŐĂďĞ ǀŽŶ 'ĞďƌĂƵĐŚƐŶĂŵĞŶ͕ tĂƌĞŶďĞnjĞŝĐŚŶƵŶŐĞŶ͕ ƵƐǁ͘ ŝŶ ĚŝĞƐĞŵ tĞƌŬ ďĞƌĞĐŚƚŝŐƚ ĂƵĐŚ ŽŚŶĞ ďĞƐŽŶĚĞƌĞ <ĞŶŶnjĞŝĐŚŶƵŶŐ ŶŝĐŚƚ njƵ ĚĞƌ ŶŶĂŚŵĞ͕ ĚĂƐƐ ƐŽůĐŚĞ EĂŵĞŶ ŝŵ ^ŝŶŶĞ ĚĞƌ tĂƌĞŶnjĞŝĐŚĞŶͲ -

Standard Packages
IRANPERSIAN SIMORG TOURS STANDARD PACKAGES +61 (0)410 177766 | [email protected] | ABN: 69 379 045 424 Iran Persian Simorg Tours are smaller, boutique excursions created for both the first-time and the experienced traveller who is looking for more than a standard tour holiday. As Iran is known and famous for its hospitality the theme is to encourage greater interactions with locals, rather than being hemmed into a strict itinerary. Simorg Tours are designed to give you the experiences of both being a tourist and a local by including highlight attractions as well as “off-the-beaten-track” or local haunts that would normally be overlooked or require the local knowledge. PACKAGES 12 DAY(MAMOOLI) TOUR 20 DAY BIG (BOZORG) TOUR 15 DAY(SHOMALLI) TOUR 21 DAY COMBINED TOUR TEHRAN AND THE GOLDEN CITIES: TEHRAN AND CENTRAL IRAN: TEHRAN TO TABRIZ: NORTHWEST AND CENTRAL IRAN: SHIRAZ, ISFAHAN, AND KASHAN SHIRAZ, ISFAHAN, YAZD AND KASHAN QAZVIN, ZANJAN, RASHT, ARDABIL, TEHRAN,QAZVIN, ZANJAN, RASHT, ARDABIL, (including Persepolis, Pasargadae, Nash-e Rostam (including Chaharmahal va Bakhtiari, Persepolis, Pasargadae, Nash-e ASTARA, MASHAD AND TURKMENSAHRA TABRIZ, SHIRAZ, ISFAHAN, YAZD , AND KASHAN and Abeyaneh village). Rostam and Abeyaneh village). (including Kaylebar, Kandovan, Aras River Valley and Alumut Valley). (including Kaylebar, Kandovan, Aras River Valley and Alumut Valley). $AU3450 $AU5450 $AU3750 $AU5750 p/person. p/person. p/person. p/person. Includes: all internal transportation and airport transfers, hotel Includes: all internal transportation and airport transfers, hotel Includes: all internal transportation and airport transfers, hotel Includes: all internal transportation and airport transfers, hotel accommodation, entry site fees, and 2 daily meals. -

Jnasci-2015-475-482
Journal of Novel Applied Sciences Available online at www.jnasci.org ©2015 JNAS Journal-2015-4-4/475-482 ISSN 2322-5149 ©2015 JNAS Public Parking Topology in Urban Spaces Using GIS (Case Study: Paveh City) Nashmin Mokhtarie and Leila Mousavi Daramaroudie* Department of Geography and Urban Planning, College of Literature and Humanities, Kermanshah Branch, Islamic Azad University, Kermanshah, Iran Corresponding author: Leila Mousavi Daramaroudie ABSTRACT: This study is addressing public parking topology in urban space (Paveh city) using Fuzzy logic and hierarchical analytic model (AHP) in GIS environment. This study method is applied in terms of study objective and it is analytic- descriptive in terms of study framework. Data collection was conducted through field- desk and using questionnaire with volume of 400 people and interviewing experts and seven criteria are considered that are 1.Gradient, 2. Population density, 3.Distance of available parking lots from urban passages network 5. Building quality (uncultivated lands and buildings with low quality) 6. Distance from travel absorption center (business centers and main shopping center, educational centers, administrative centers, cultural centers, health care centers and Hospitals), 7.The property value that is used as a key indicator for parking topology in the studied area. The use of weighting techniques and assigning points and combining data, analytic hierarchy AHP in fuzzy logic bed and overlap methods of indices are leading properties of this research. The findings of this study -

(Hymenoptera: Ichneumonidae) from ILAM and KERMANSHAH PROVINCES, WESTERN IRAN
Entomol. Croat. 2015, Vol. 19. Num 1–2: 55–66 doi: 10.17971/EC.2015.19.07 A FAUNISTIC STUDY OF ICHNEUMONID WASPS (HymenopteRA: Ichneumonidae) FROM ILAM AND KERMANSHAH PROVINCES, WESTERN IRAN Hassan Ghahari1 & Reijo Jussila2 1Department of Plant Protection, Yadegar – e- Imam Khomeini (RAH) Shahre Rey Branch, Islamic Azad University, Tehran, Iran; email: [email protected] 2Zoological Museum, Section of Biodiversity and Environmental Sciences, Department of Biology, FI 20014 University of Turku, Finland. E-mail: [email protected] Accepted: October 2015 This paper deals with a faunistic survey on ichneumonid wasps (Hyme- noptera, Ichneumonidae) from some regions of Ilam and Kermanshah provin- ces (western Iran). In total 19 species from the nine subfamilies Alomyinae, Cremastinae, Cryptinae, Diplazontinae, Ichneumoninae, Metopiinae, Pimpli- nae, Tersilochinae, and Tryphoninae were collected and identified. Two speci- es Probles (Microdiaparsis) microcephalus (Gravenhorst, 1829) and Tersilochus (Pectinolochus) striola (Thomson, 1889) are new records for Iran. Hymenoptera, Ichneumonidae, Ilam, Kermanshah, new record, Iran H. GHAHARI I R. JUSSILA: Faunističko istraživanje parazitskih osica (Hymenoptera: Ichneumonidae) iz provincija Ilam i Kermanshah, zapadni Iran. Entomol. Croat. Vol. 19. Num. 1–4: 55–66. U radu je prikazano faunističko istraživanje parazitskih osica (Hymenop- tera, Ichneumonidae) iz nekih područja provincija Ilam i Kermanshah (zapad- ni Iran). Ukupno je sakupljeno i determinirano 19 vrsta osica iz 9 podporodica (Alomyinae, -

Cutaneous Leishmaniasis in Qasr-E Shirin, a Border Area in the West of Iran
Veterinary World, EISSN: 2231-0916 RESEARCH ARTICLE Available at www.veterinaryworld.org/Vol.11/December-2018/8.pdf Open Access Cutaneous leishmaniasis in Qasr-e Shirin, a border area in the west of Iran Yazdan Hamzavi1, Naser Nazari1, Nahid Khademi2, Keivan Hassani3 and Arezoo Bozorgomid1 1. Department of Medical Parasitology and Mycology, Faculty of Medicine, Kermanshah University of Medical Sciences, Kermanshah, Iran; 2. Department of Disease, Kermanshah Health Center, Kermanshah University of Medical Sciences, Kermanshah, Iran; 3. Students Research Committee, Kermanshah University of Medical Sciences, Kermanshah, Iran. Corresponding author: Arezoo Bozorgomid, e-mail: [email protected] Co-authors: YH: [email protected], NN: [email protected], NK: [email protected], KH: [email protected] Received: 20-08-2018, Accepted: 31-10-2018, Published online: 17-12-2018 doi: 10.14202/vetworld.2018.1692-1697 How to cite this article: Hamzavi Y, Nazari N, Khademi N, Hassani K, Bozorgomid A (2018) Cutaneous leishmaniasis in Qasr-e Shirin, a border area in the west of Iran, Veterinary World, 11(12): 1692-1697. Abstract Aim: The prevalence of cutaneous leishmaniasis (CL) is growing in Iran, and new sources of the disease have been found in the country. The purpose of this study was to describe the epidemiology of CL in Qasr-e Shirin County, Kermanshah Province, West of Iran. Qasr-e Shirin is located near the Iran-Iraq border, and several million pilgrims pass through this area to Iraq every year. Materials and Methods: A descriptive cross-sectional study was carried out for active case detection from April 1, 2014, to March 31, 2015. -

Related Factors of Female Genital Mutilation
omens H f W ea o l l th a C Pashaei, J Women’s Health Care 2012, 1:2 n r a u r e DOI: 10.4172/2167-0420.1000108 o J Journal of Women's Health Care ISSN: 2167-0420 Research Article Open Access Related Factors of Female Genital Mutilation (FGM) in Ravansar (Iran) Pashaei T1*, Rahimi A2, Ardalan A1, Felah A3 and Majlessi F1 1Department of Health education and Promotion, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran 2Department of Epidemiology and Biostatistics, School of public health, Tehran University of Medical Sciences, Tehran, Iran 3School of Health, Kurdistan University of Medical Sciences, Tehran, Iran Abstract This study was performed to determine the prevalence and related factors of Female Genital Mutilation (FGM) in women visited at the health centers of the city of Ravansar In Kermanshah province, Iran. This cross-sectional study was conducted on 348 women who were visited at 5 health centers of the city of Ravansar. Data was collected using a structured questionnaire and women were examined about exist FGM. The prevalence of FGM was 55.7% among Ravansars’ women. It increases with age and about 54.4% were circumcised less than 7 years age. Almost all operations were performed by traditional circumcisers 85.7%. FGM was correlated with mothers’ education level (p<0.001), age (p<0.001), women’s level of education (p=0.006) and the level of knowledge and attitude toward mutilation (p<0.001). FGM is a common practice in Ravansars’ women. Improving the public knowledge regarding FGM and its consequences is extremely essential. -

Epidemiological Prevalence of Pediculosis and Its
Clinician’s corner Original Article Images in Medicine Experimental Research Case Report Miscellaneous Letter to Editor DOI: 10.7860/JCDR/2020/43085.13472 Review Article Postgraduate Education Epidemiological Prevalence of Pediculosis and Case Series its Influencing Factors in Iranian Schools: Epidemiology Section Systematic Review and Meta-analysis Short Communication MALIHE SOHRABIVAFA1, ELHAM GOODARZI2, VICTORIA MOMENABADI3, MARYAM SERAJI4, HASAN NAEMI5, ELHAM NEJADSADEGHI6, ZAHER KHAZAEI7 ABSTRACT Q-Cochran test was used at an error level of less than 10% and Introduction: Pediculosis is an endemic parasitic infestation in the quantity was estimated by I2. The Begg Rank Correlation many countries of the world. Iran is one of the countries with a Test and Eggers Regression Method were used to measure the high rate of pediculosis. publication bias. Aim: To investigate the prevalence and factors associated with Results: The results showed that 428,993 students were studied pediculosis in primary school students of Iran. in 55 papers between 2000 and 2016 and the prevalence of head louse (Pediculosis human capitis) was 6.4% (95% CI: 6-6.9). Materials and Methods: The literature search was carried The prevalence of lice (pediculosis) infestation among girls was out by two researchers on national databases including: SID, 6.1% (95% CI: 4.6-7.4) and in boys was 1.2% (95% CI: 0.8-1.7) Iranmedex, Magiran, Irandoc and international database and in rural areas prevalence was more than urban areas. including: Scopus, Pubmed and Web of Science to find relevant articles between 2000 and 2016. The search strategy Conclusion: The results of this study demonstrated a high was performed using keywords such as: “epidemiology”, incidence of pediculosis among rural school-girls. -
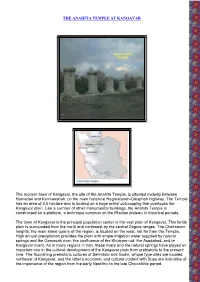
The Anahita Temple at Kangavar
THE ANAHITA TEMPLE AT KANGAVAR The modern town of Kangavar, the site of the Anahita Temple, is situated midway between Hamadan and Kermanshah, on the main historical Hegmataneh-Ctesphon highway. The Temple has an area of 4.6 hectare and is located on a huge schist outcropping that overlooks the Kangavar plain. Like a number of other monumental buildings, the Anahita Temple is constructed on a platform, a technique common on the IRanian plateau in historical periods. The town of Kangavar is the principal population center in the vast plain of Kangavar. This fertile plain is surrounded from the north and northwest by the central Zagros ranges. The Chelmaran heights, the main stone quarry of the region, is located on the west, not far from the Temple. High annual precipitation provides the plain with ample irrigation water supplied by natural springs and the Gamasab river, the confluence of the Khurram-rud, the Asadabad, and te Kangavar rivers. As in many regions in Iran, these rivers and the natural springs have played an important role in the cultural development of the Kangavar plain from prehistoric to the present time. The flourishing prehistoric cultures of Seh-Gabi and Godin, whose type sites are located northeast of Kangavar, and the latter's economic and cultural contact with Susa are indicative of the importance of the region from the early Neolithic to the late Chalcolithic period. Southern view of Anahita Temple The strategic geographical location of the plain also played an important role as the commercial highway and locus of contact between the cultural centers on the west and east streching as far as Khorasan and China. -

New Evidence on the Chronology of the “Anahita Temple”
Iranica Antiqua, vol. XLIV, 2009 doi: 10.2143/IA.44.0.2034383 NEW EVIDENCE ON THE CHRONOLOGY OF THE “ANAHITA TEMPLE” BY Massoud AZARNOUSH (Iranian Center for Archaeological Research, Tehran) Abstract: Partly standing-partly excavated remains of a monument in Kangavar, a town in western Iran between Hamadan and Kermanshah, have been dated to the Seleucid and/or Parthian periods. In an article published in 1981, nevertheless, M. Azarnoush argues in favour of a late Sasanian date for this site. The discovery of a brick under the massive masonry of the western platform of the monument in the course of later excavations provided the possibility for thermoluminescence dating of this sample. The TL reading of the brick confi rms the Sasanian date of the monument. The present article intends to assess this and some other new information about the site. Keywords: W-Iran, Kangavar, Anahita Temple, Sasanian, chronology I- Introduction In an article published in 1981, I argued in favour of a late Sasanian date for the monument of Kangavar, frequently labelled the “Anahita Temple” (Azarnoush 1981: 69-94, Pl. 12-19). By that time I had completed two seasons of excavations on this site, following fi ve seasons of work headed by Seyfollâh-e Kâmbakhsh-e Fard, another Iranian archaeologist of whose expeditions I am certainly honoured to have been a member. Reasons backing the new chronology may be outlined in the following: – Isidor of Charax is the oldest author who mentions the presence of an Artemis Temple in Concobar, most probably the Greek pronunciation for the Iranian Kangavar.