Facility Based Assessment for Reproductive
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Code Under Name Girls Boys Total Girls Boys Total 010290001
P|D|LL|S G8 G10 Code Under Name Girls Boys Total Girls Boys Total 010290001 Maiwakhola Gaunpalika Patidanda Ma Vi 15 22 37 25 17 42 010360002 Meringden Gaunpalika Singha Devi Adharbhut Vidyalaya 8 2 10 0 0 0 010370001 Mikwakhola Gaunpalika Sanwa Ma V 27 26 53 50 19 69 010160009 Phaktanglung Rural Municipality Saraswati Chyaribook Ma V 28 10 38 33 22 55 010060001 Phungling Nagarpalika Siddhakali Ma V 11 14 25 23 8 31 010320004 Phungling Nagarpalika Bhanu Jana Ma V 88 77 165 120 130 250 010320012 Phungling Nagarpalika Birendra Ma V 19 18 37 18 30 48 010020003 Sidingba Gaunpalika Angepa Adharbhut Vidyalaya 5 6 11 0 0 0 030410009 Deumai Nagarpalika Janta Adharbhut Vidyalaya 19 13 32 0 0 0 030100003 Phakphokthum Gaunpalika Janaki Ma V 13 5 18 23 9 32 030230002 Phakphokthum Gaunpalika Singhadevi Adharbhut Vidyalaya 7 7 14 0 0 0 030230004 Phakphokthum Gaunpalika Jalpa Ma V 17 25 42 25 23 48 030330008 Phakphokthum Gaunpalika Khambang Ma V 5 4 9 1 2 3 030030001 Ilam Municipality Amar Secondary School 26 14 40 62 48 110 030030005 Ilam Municipality Barbote Basic School 9 9 18 0 0 0 030030011 Ilam Municipality Shree Saptamai Gurukul Sanskrit Vidyashram Secondary School 0 17 17 1 12 13 030130001 Ilam Municipality Purna Smarak Secondary School 16 15 31 22 20 42 030150001 Ilam Municipality Adarsha Secondary School 50 60 110 57 41 98 030460003 Ilam Municipality Bal Kanya Ma V 30 20 50 23 17 40 030460006 Ilam Municipality Maheshwor Adharbhut Vidyalaya 12 15 27 0 0 0 030070014 Mai Nagarpalika Kankai Ma V 50 44 94 99 67 166 030190004 Maijogmai Gaunpalika -

Feasibility Study of Kailash Sacred Landscape
Kailash Sacred Landscape Conservation Initiative Feasability Assessment Report - Nepal Central Department of Botany Tribhuvan University, Kirtipur, Nepal June 2010 Contributors, Advisors, Consultants Core group contributors • Chaudhary, Ram P., Professor, Central Department of Botany, Tribhuvan University; National Coordinator, KSLCI-Nepal • Shrestha, Krishna K., Head, Central Department of Botany • Jha, Pramod K., Professor, Central Department of Botany • Bhatta, Kuber P., Consultant, Kailash Sacred Landscape Project, Nepal Contributors • Acharya, M., Department of Forest, Ministry of Forests and Soil Conservation (MFSC) • Bajracharya, B., International Centre for Integrated Mountain Development (ICIMOD) • Basnet, G., Independent Consultant, Environmental Anthropologist • Basnet, T., Tribhuvan University • Belbase, N., Legal expert • Bhatta, S., Department of National Park and Wildlife Conservation • Bhusal, Y. R. Secretary, Ministry of Forest and Soil Conservation • Das, A. N., Ministry of Forest and Soil Conservation • Ghimire, S. K., Tribhuvan University • Joshi, S. P., Ministry of Forest and Soil Conservation • Khanal, S., Independent Contributor • Maharjan, R., Department of Forest • Paudel, K. C., Department of Plant Resources • Rajbhandari, K.R., Expert, Plant Biodiversity • Rimal, S., Ministry of Forest and Soil Conservation • Sah, R.N., Department of Forest • Sharma, K., Department of Hydrology • Shrestha, S. M., Department of Forest • Siwakoti, M., Tribhuvan University • Upadhyaya, M.P., National Agricultural Research Council -

Nepal Earthquake District Profile - Gorkha OSOCC Assessment Cell 09.05.2015
Nepal Earthquake District Profile - Gorkha OSOCC Assessment Cell 09.05.2015 This report is produced by the OSOCC Assessment Cell based on secondary data from multiple sources, including the Government of Nepal, UNDAC, United Nations Agencies, non-governmental organisation and media sources. I. Situation Overview Gorkha, with a population of more than 271,000, is one of the worst-affected districts.1 The epicenter of the earthquake was in Brapok, 15km from Gorkha town. As of 6 May, 412 people have been reported killed and 1,034 injured. In the southern part of the district, food has been provided, but field observations indicate that the food supplied might not be enough for the actual population in the area. Several VDCs in the mountainous areas of Gorkha are yet to be reached by humanitarian assistance. There are no roads in these northern areas, only footpaths. The level of destruction within the district and even within VDCs varies widely, as does the availability of food. A humanitarian hub has been set up at the Chief District Officer’s (CDO) premises in Gorkha town. Reported number of people in need (multiple sources) The figures featured in this map have been collected via multiple sources (district authorities, Red Cross, local NGO, media). Where multiple figures for the same location have been reported the highest one was taken. These figures are indicative and do not represent the overall number of people in need. 1 This is an updated version of the Gorkha District Profile that was published by ACAPS on 1 May 2015. As with other mountain areas of Nepal, Gorkha contains popular locations for foreign trekkers. -

Food Insecurity and Undernutrition in Nepal
SMALL AREA ESTIMATION OF FOOD INSECURITY AND UNDERNUTRITION IN NEPAL GOVERNMENT OF NEPAL National Planning Commission Secretariat Central Bureau of Statistics SMALL AREA ESTIMATION OF FOOD INSECURITY AND UNDERNUTRITION IN NEPAL GOVERNMENT OF NEPAL National Planning Commission Secretariat Central Bureau of Statistics Acknowledgements The completion of both this and the earlier feasibility report follows extensive consultation with the National Planning Commission, Central Bureau of Statistics (CBS), World Food Programme (WFP), UNICEF, World Bank, and New ERA, together with members of the Statistics and Evidence for Policy, Planning and Results (SEPPR) working group from the International Development Partners Group (IDPG) and made up of people from Asian Development Bank (ADB), Department for International Development (DFID), United Nations Development Programme (UNDP), UNICEF and United States Agency for International Development (USAID), WFP, and the World Bank. WFP, UNICEF and the World Bank commissioned this research. The statistical analysis has been undertaken by Professor Stephen Haslett, Systemetrics Research Associates and Institute of Fundamental Sciences, Massey University, New Zealand and Associate Prof Geoffrey Jones, Dr. Maris Isidro and Alison Sefton of the Institute of Fundamental Sciences - Statistics, Massey University, New Zealand. We gratefully acknowledge the considerable assistance provided at all stages by the Central Bureau of Statistics. Special thanks to Bikash Bista, Rudra Suwal, Dilli Raj Joshi, Devendra Karanjit, Bed Dhakal, Lok Khatri and Pushpa Raj Paudel. See Appendix E for the full list of people consulted. First published: December 2014 Design and processed by: Print Communication, 4241355 ISBN: 978-9937-3000-976 Suggested citation: Haslett, S., Jones, G., Isidro, M., and Sefton, A. (2014) Small Area Estimation of Food Insecurity and Undernutrition in Nepal, Central Bureau of Statistics, National Planning Commissions Secretariat, World Food Programme, UNICEF and World Bank, Kathmandu, Nepal, December 2014. -

CARE Nepal Save the Children UNDP World Vision International
Volume III Recovery & Reconstruction Quarterly Bulletin| Gorkha September 2016 Volume III Asal Chhimekee Nepal UN Women WHO International Nepal Fellowship International Medical Corps Good Neighbors International Sajhedari Bikaas People In Need HRRP ECO- Nepal Updates United Vision Nepal Nepal Red Cross Society Oxfam Suaahara Catholic Relief Services UNICEF CARE Nepal Save the Children UNDP World Vision International Recovery & Reconstruction Quarterly Bulletin| Gorkha September 2016 Volume III July – September, 2016 Working VDC's: Shreenathkot, Aappipal, Ghairung, Bhumlichowk and Ghyalchowk, Gorkha Asal Chimekee Nepal is an organization which was registered as NGO in 2059 and was started by Pokhara Christian Community Kaski. It works in coordination with DDRC, related district government offices, like minded organizations, local communities and churches in Gorkha. The organization has been focusing on rehabilitation, reconstruction, livelihood & health support, disaster preparedness and strengthening local community together with the government bodies and local community. Some of the specific works of this organization are as follows: 1: Reconstructions of Health Post Buildings in Aappipal, Ghairung, Bhumlichowk & Ghyalchowk Except Aappipal healthpost, other health post reconstruction works has been completed and in the process on handover program to the local community within the 1st week of October, 2016 with necessary equipments and furnishing. The representatives of MoHP & DHO were also involved during the process of reconstruction. From the expert side, the technical consultant visited to healthpost construction site for monitoring and supervision of the constructional work. 2: Reconstruction of VDC building Shreentahkot VDC building reconstructions work has been started from 5th of Asoj, 2073. The reconstruction work was started formally by doing laystone foundation of the VDC building. -

NCCSP Success Story 2017.Pdf
Government of Nepal Ministry of Population & Environment Nepal Climate Change Support Programme SUCCESS STORIES ON ADAPTATION FROM THE FIELD Vol. II • December 2016 Helping Local Communities Adapt to the Effects of Climate Change in Nepal Publisher Government of Nepal Ministry of Population and Environment Nepal Climate Change Support Programme Singhadurbar, Kathmandu, Nepal Phone : (977) 1 4211894 (977) 1 4200580 Email : [email protected] Web : www.nccsp.gov.np Copyright © 2016 Government of Nepal, Ministry of Population and Environment All right reserved. Information given in this publication may be reproduced, stored in retrieval system or transmitted in any form or by any means - electronic, mechanical or otherwise - by duly acknowledging the source. Citation MoPE/NCCSP. (2016). Success Stories on Adaptation from the field. Government of Nepal. Ministry of Population and Environment, Kathmandu, Nepal. Stories & Photographs Nepal Climate Change Support Programme Design & Printed at Golden Egg Creation Pvt. Ltd. Nayabazar, Kathmandu. [email protected] Government of Nepal Ministry of Population & Environment Nepal Climate Change Support Programme SUCCESS STORIES ON ADAPTATION FROM THE FIELD Vol. II • December 2016 Foreword Nepal Climate Change Support Programme (NCCSP) is the first significant initiative by the Government of Nepal in the sector of climate change adaptation. Ministry of Population and Environment (MoPE) is a lead agency implementing the NCCSP in close collaboration with the Ministry of Federal Affairs and Local Development (MoFALD) and the Alternative Energy Promotion Center (AEPC). The overall goal of this programme is to ensure that Nepal’s poorest and most vulnerable people are able to adapt well to the negative impacts of climate change. -

Japan International Cooperation Agency (JICA)
Chapter 3 Project Evaluation and Recommendations 3-1 Project Effect It is appropriate to implement the Project under Japan's Grant Aid Assistance, because the Project will have the following effects: (1) Direct Effects 1) Improvement of Educational Environment By replacing deteriorated classrooms, which are danger in structure, with rainwater leakage, and/or insufficient natural lighting and ventilation, with new ones of better quality, the Project will contribute to improving the education environment, which will be effective for improving internal efficiency. Furthermore, provision of toilets and water-supply facilities will greatly encourage the attendance of female teachers and students. Present(※) After Project Completion Usable classrooms in Target Districts 19,177 classrooms 21,707 classrooms Number of Students accommodated in the 709,410 students 835,820 students usable classrooms ※ Including the classrooms to be constructed under BPEP-II by July 2004 2) Improvement of Teacher Training Environment By constructing exclusive facilities for Resource Centres, the Project will contribute to activating teacher training and information-sharing, which will lead to improved quality of education. (2) Indirect Effects 1) Enhancement of Community Participation to Education Community participation in overall primary school management activities will be enhanced through participation in this construction project and by receiving guidance on various educational matters from the government. 91 3-2 Recommendations For the effective implementation of the project, it is recommended that HMG of Nepal take the following actions: 1) Coordination with other donors As and when necessary for the effective implementation of the Project, the DOE should ensure effective coordination with the CIP donors in terms of the CIP components including the allocation of target districts. -
VBST Short List
1 आिेदकको दर्ा ा न륍बर नागररकर्ा न륍बर नाम थायी जि쥍ला गा.वि.स. बािुको नाम ईभेꅍट ID 10002 2632 SUMAN BHATTARAI KATHMANDU KATHMANDU M.N.P. KEDAR PRASAD BHATTARAI 136880 10003 28733 KABIN PRAJAPATI BHAKTAPUR BHAKTAPUR N.P. SITA RAM PRAJAPATI 136882 10008 271060/7240/5583 SUDESH MANANDHAR KATHMANDU KATHMANDU M.N.P. SHREE KRISHNA MANANDHAR 136890 10011 9135 SAMERRR NAKARMI KATHMANDU KATHMANDU M.N.P. BASANTA KUMAR NAKARMI 136943 10014 407/11592 NANI MAYA BASNET DOLAKHA BHIMESWOR N.P. SHREE YAGA BAHADUR BASNET136951 10015 62032/450 USHA ADHIJARI KAVRE PANCHKHAL BHOLA NATH ADHIKARI 136952 10017 411001/71853 MANASH THAPA GULMI TAMGHAS KASHER BAHADUR THAPA 136954 10018 44874 RAJ KUMAR LAMICHHANE PARBAT TILAHAR KRISHNA BAHADUR LAMICHHANE136957 10021 711034/173 KESHAB RAJ BHATTA BAJHANG BANJH JANAK LAL BHATTA 136964 10023 1581 MANDEEP SHRESTHA SIRAHA SIRAHA N.P. KUMAR MAN SHRESTHA 136969 2 आिेदकको दर्ा ा न륍बर नागररकर्ा न륍बर नाम थायी जि쥍ला गा.वि.स. बािुको नाम ईभेꅍट ID 10024 283027/3 SHREE KRISHNA GHARTI LALITPUR GODAWARI DURGA BAHADUR GHARTI 136971 10025 60-01-71-00189 CHANDRA KAMI JUMLA PATARASI JAYA LAL KAMI 136974 10026 151086/205 PRABIN YADAV DHANUSHA MARCHAIJHITAKAIYA JAYA NARAYAN YADAV 136976 10030 1012/81328 SABINA NAGARKOTI KATHMANDU DAANCHHI HARI KRISHNA NAGARKOTI 136984 10032 1039/16713 BIRENDRA PRASAD GUPTABARA KARAIYA SAMBHU SHA KANU 136988 10033 28-01-71-05846 SURESH JOSHI LALITPUR LALITPUR U.M.N.P. RAJU JOSHI 136990 10034 331071/6889 BIJAYA PRASAD YADAV BARA RAUWAHI RAM YAKWAL PRASAD YADAV 136993 10036 071024/932 DIPENDRA BHUJEL DHANKUTA TANKHUWA LOCHAN BAHADUR BHUJEL 136996 10037 28-01-067-01720 SABIN K.C. -

Sensus Information
Sensus Information Area of Municipality Drinking Water Total area:-138.95 sq.km. Distributed by consumption committee:-502 Residential Area:-30.8 hector Public tap:- Agriculture sector:-3256.58 hector Private tap:- Market area:-5 sq.km Without tap ward no:-1,3,6,7,9,10,11 Forest sector:-6597 hector Partial tap distributed ward no:-2,4,5 and 8 Boarder of Municipality Educational institution East:-Ganeshpur,ashriram VDC Primary:- West:-Bagarkot,Ajaymeru VDC Government:-21 North:-Samaiji,Koteli VDC Private:-2 South:-Gankhet VDC Secondary:- Government:-2 Private:-1 Madhyamic Bidhyalay:- Government:-3 Private:-1 Higher Secondary School:- General:-2 Private:-1 University:- General campus:-1 Computer Institute:-6 Geographical coverage Communication Coordinate:-29.13 to 29.24 north Telephone Exchange capacity:-640 Longitude:-80.18 to 80.31 Telephone line:-518 Located height:6500 ft from the District post office:-1 sealevel Climate:- Smshitoshna Courier services:-6 Tempreture:-30 degree max. and 2 Weekly paper:3 degree min. Population(2062) Daily paper:-1 Total population:-22,378 Monthly paper:-1 Women:-11490 Mun Comunication center:-not available Men:-10888 Email/Internet:Available Litracy percentage:-64.2% Total Houses:-3976 Stadium:-1 No. of family:-4038 Health facilities Main Religious places Government Hospital:-1(15 bed) Shree ugratara Bhagwati Mandir,shree Ghatal sthan,shree sahshraling mandir & shree ashigarm mandir. Community hospital:-1(43 bed) Historical places Herbo hospital:-1 Amargadhi killa,Rawaltoli Gupha Sub-hospital :-4 Administrative structure of mun Cleaners Tractor:1 1.Administration officer-1 Prog:-4 2.Nayab subba-1 Container:-37 3.Accountant-1 Cleaners labours:-7 4.Overseer-1 General Toilet:-2 5.Kharidar-3 Total dust production:-1 metric 6.Surveyor-1 ton(per day) Domping side:-Available 7.Panjikadhikari-1 Financial Institution 8.Sub-overseer Government Bank:-3 9.Office helper or computer assistance:1 Road Light 10.Asst. -
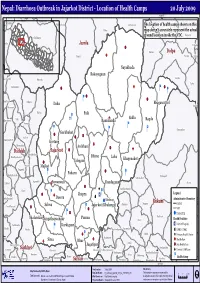
Pdf | 268.57 Kb
Nepal: Diarrhoea Outbreak in Jajarkot District - Location of Health Camps 20 July 2009 82°30'0"E Jubika Ramchuli Pakha Dah Malikathota Guthichaur The location of health camps shown on this Haku map doesn't accuratelyRIMI represent the actual ground location inside the VDC. Kaigaun Chilkhaya Gela Jumla &! Pahada Kalikot Sarmi Dolpa Tamti GF Narku Likhu Nayakbada Rokayagaun Kalika Kasikandh Odanku Laha GF ! Baluwatar &! Ý & Ý &! &! Raniban Odhari Ý Bhagawatitol Daha Suhun Bhawani Kalika Paik ; &! Sakla Kharigera Toli Ý Ramidanda Ragda Nomule Ý Ý Ý Ý Gautamkot &! Garkhakot ! Salleri &! & Narayan N.P. Kortang GF Chauratha Archhani &! GF Dailekh Jajarkot &! Moheltolee Dhime Bindhyabasini Laha Khagenakot &! Talegaun Room Majkot Pagnath ! Padaru & BadaBhairab Ý Ý Syalagadi AathbisKot Jaganath Lakuri &!Suwanauli Dandagaun Sisne ! & h AathbisDanda Katti ! Jhapra Æ Ý Legend & Ý GF × q DadaParajul Dasera Khalanga Administrative Boundary ! Rukum Jang Ghetma Magma District AwalParajul ! Salma Jajarkot (Khalanga) & Ý &! VDC Ý &! ! District HQ Thalarekar &! Punma Baflikot Jungathapachaur Duli Health Facilities Æ Pwang Lalikanda Karkigaun Pipalq District Hospital Piladi Matela Ý PurtimKanda Garayala × DPHO / DHO GF Ý Jhula ; Primary Health Centre Ratu GF Kotjahari GF GF Sima Bhur Health Post Simli ! AWALCHING Jagatipur & SubPokhara Health Post Rangsi Surkhet Syalapakha Garpan Ghoreta Chaurjahari( (Bijayashwari) h District Cold Room Kholagaun MusikotKhalanga( Ranibas Arma Chhiwang Kanda Pamka Bame Health Camp Rajena Agragaun Suikot Sankha Sobha Satakhani Kafalkot Salyan Kalagaun Nuwakot Pyaugha Bhalakacha Ý 82°30'0"E Produced on: 2 July 2009 Disclaimers: Map Produced by OCHA, Nepal Map Doc Name: D_Outbreak_Jajarkot_3W_A4_21072009_v01 The boundaries and names shown and the 02 4 Km Data Source(s): Data are collected from DPHO, UN Agencies and I/NGOs Web Resources: http://www.un.org.np designations used on this map do not imply official I Boundaries - Department of Survey, Nepal Projection/Datum: Geographic/Everest 1830 endorsement or acceptance by the United Nations.. -

Nepal Gorkha District Assessment Form
Nepal Gorkha District Assessment Form IDENTIFICATION AND LOCATION I2 DATE OF ASSESSMENT * I3 ENUMERATOR NAME * yyyymmdd I4 DISTRICT * I5 VDC/MUNICIPALITY * I5 VDC/MUNICIPALITY * Please specify Gorkha Bihi Chhaikampar Chumchet Lho Prok Samagaun Sirdibas Uhya Other (specify) I6 WARD * I7 VILLAGE NAME * 1 2 3 4 5 6 7 8 9 Do not know I8 GPS COORDINATES GPS coordinates can only be collected when outside. latitude (x.y °) longitude (x.y °) altitude (m) accuracy (m) I9 SOURCE(S) FOR THIS ASSESSMENT None 1 2 3 or more Select the number of people you spoke to for each category . * Official (administrative) . * Village representative . * Religious leader . * Army or police . * Health worker . * Social worker . * International NGO / development partner . * Teacher . * Other local person I10 HOW MANY OF THOSE KEY INFORMANTS WERE WOMEN? * COMMUNITY PROFILE » Total population P1 ENTER THE PERCENTAGE OF THE OVERALL POPULATION WHO ARE IN THE FOLLOWING CATEGORIES. Needs to add up to 100% * * * % in normal situation % requiring assistance % requiring immediate assistance » Male P2 ENTER THE PERCENTAGE OF THE MALE POPULATION WHO ARE IN THE FOLLOWING CATEGORIES. Needs to add up to 100% * * * % in normal situation % requiring assistance % requiring immediate assistance » Female P3 ENTER THE PERCENTAGE OF THE FEMALE POPULATION WHO ARE IN THE FOLLOWING CATEGORIES. Needs to add up to 100% * * * % in normal situation % requiring assistance % requiring immediate assistance » Children P4 ENTER THE PERCENTAGE OF CHILDREN WHO ARE IN THE FOLLOWING CATEGORIES. Needs -
![Uf]/Vf K'gm;J]{If0f Ug'{Kg]{ Nfeu|Fxl Ljj/0F](https://docslib.b-cdn.net/cover/5832/uf-vf-kgm-j-if0f-ug-kg-nfeu-fxl-ljj-0f-1055832.webp)
Uf]/Vf K'gm;J]{If0f Ug'{Kg]{ Nfeu|Fxl Ljj/0F
g]kfn ;/sf/ ;+3Lo dfldnf tyf :yfgLo ljsf; dGqfno s]Gb|Lo cfof]hgf sfof{Gjog OsfO{ e"sDkLo cfjf; k'glg{df{0f cfof]hgf Hjfun, nlntk'/ uf]/vf k'gM;j]{If0f ug'{kg]{ nfeu|fxL ljj/0f . S.N G_ID RV/RS Grievant Name District VDC/MUN (P) Ward(P) Tole GP/NP WARD Slip No Remarks 1 281924 RS Nettra Bahadur Thap Gorkha Aanppipal 1 bajredanda Palungtar 3 21350 2 290180 RS Sabitri Devi Bhattrai Gorkha Aanppipal 1 bajredanda Palungtar 3 212331 3 288425 RS Jit Bahadur Rana Magar Gorkha Aanppipal 1 jal jala Palungtar 3 4 290553 RS Dhan Bahadur Rana Gorkha Aanppipal 1 judi thumka Palungtar 3 5 290114 RS Rithe Sarki Gorkha Aanppipal 1 pathivara Palungtar 3 6 288914 RS Tulka Sarki Gorkha Aanppipal 1 pathivara Palungtar 3 7 288959 RS Arjun Baniya Gorkha Aanppipal 1 pathivara Palungtar 3 8 290178 RS Sanak Bahadur Bhattrai Gorkha Aanppipal 1 pathivara Palungtar 3 9 290030 RS Jibarayal Miya Gorkha Aanppipal 2 dumre danda Palungtar 3 10 290560 RS Gurungseni Sunar Gorkha Aanppipal 2 maibal Palungtar 3 215317 11 290034 RS Damar Kumari Thapa Gorkha Aanppipal 2 maibal Palungtar 3 12 288925 RS Amar Bahadur Kuwar Gorkha Aanppipal 2 pachchyan Palungtar 3 13 290556 RS Rajendra Dhakal Gorkha Aanppipal 2 raute pani Palungtar 3 215570 14 286299 RS Sarala Devkota Gorkha Aanppipal 2 raute pani Palungtar 3 423666 15 288462 RS Bijaya Raj Devkota Gorkha Aanppipal 2 raute pani Palungtar 3 16 288920 RS Shree Niwas Devkota Gorkha Aanppipal 2 raute pani Palungtar 3 17 290055 RS Uttam Kumar Shtestha Gorkha Aanppipal 2 raute pani Palungtar 3 18 290047 RS Brendra Devkota Gorkha Aanppipal