Rheumatology: 6
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Evaluation of the Inferior Calcaneal Spurs Influence on Plantar Fascia
Evaluation of the Inferior Calcaneal Spurs Influence on Plantar Fascia Thickness Clint Jiroux, PMS-II ; Kyle Schwickerath, PMS-II; Frank Felix, PMS-II; Chad Smith, PMS-II; Matt Greenblatt, PMS-II Arizona School of Podiatric Medicine – Midwestern University Printing: This poster is 48” wide by 36” high. It’s STATEMENT OF PURPOSE ANALYSIS & DISCUSSION designed to be printed on a large • Plantar fasciitis is a common pathology associated with plantar heel pain. It is Through ultrasound, our research revealed the spur does not show a reported that in the United States, two million patients are treated for plantar relationship to the thickness of the plantar fascia. Thus, based on our data, printer. fasciitis annually, and accounts for 15% of all foot disorders (1). A frequent diagnostic measurements of the fascia band thickness should not take into association with plantar fasciitis is the presence of an inferior calcaneal heel consideration the presence of a heel spur. This data is supportive to the spur. Often debated by medical professionals; Is the heel spur an incidental or consensus of 4mm being the diagnostic value for plantar fasciitis. Additionally, causation of plantar fasciitis (2-4)? Using ultrasound imaging, the plantar fascia this strengthens support of the heel spur being an incidental finding with plantar Figure 1. Type A inferior calcaneal spur that extends above the plantar fascia. (A) Type B inferior calcaneal Figure 2. Longitudinal ultrasound of the plantar fascia with the presence of an inferior calcaneal spur. (A) A fasciitis. thickness can be quantifiably measured to determine plantar fasciitis. An spur that extends into the plantar fascia. -

Rotator Cuff Tendon Ruptures and Degeneration As the First Manifestation of Polymyalgia Rheumatica Disease - a Case Report
Open Access Austin Journal of Clinical Case Reports Case Report Rotator Cuff Tendon Ruptures and Degeneration as the First Manifestation of Polymyalgia Rheumatica Disease - A Case Report Bazoukis G1*, Michelongona P2, Papadatos SS1, Pagkalidou E1, Grigoropoulou P1, Fragkou A1 and Abstract Yalouris A1 Polymyalgia Rheumatica (PMR) is a common rheumatic disease of the 1Department of Internal Medicine, General Hospital of elderly. Although it is a well-established disease, its causes and pathophysiology Athens “Elpis”, Greece remain unclear. In our case report we present an 83-year-old female presented 2Department of Internal Medicine, General Hospital of at the emergency department because of fever and diarrhea. Her medical Korinthos, Greece history included a recent orthopedic surgery because of tendons rupture of the *Corresponding author: George Bazoukis, rotator cuff. Her blood exams showed increased inflammatory markers and a Department of Internal Medicine, General Hospital of three-digit ESR. The diagnosis of PMR was set after the exclusion of infectious Athens “Elpis”, Greece and other diseases that mimic PMR symptoms. To the best of our knowledge, it is the first time that rotator cuff tendons rupture and degeneration is the first Received: June 05, 2016; Accepted: August 02, 2016; manifestation of PMR disease. Clinicians should be aware of the degeneration Published: September 08, 2016 of the shoulder and hip extra-articular structures in PMR and they should keep in mind that it can be the first manifestation of the disease. Keywords: Polymyalgia rheumatica; Rotator cuff denegeration; Tendon rupture Introduction and infraspinatus muscles as well as significant tendinopathy of the subscapularis and long head of biceps muscles. -

Juvenile Spondyloarthropathies: Inflammation in Disguise
PP.qxd:06/15-2 Ped Perspectives 7/25/08 10:49 AM Page 2 APEDIATRIC Volume 17, Number 2 2008 Juvenile Spondyloarthropathieserspective Inflammation in DisguiseP by Evren Akin, M.D. The spondyloarthropathies are a group of inflammatory conditions that involve the spine (sacroiliitis and spondylitis), joints (asymmetric peripheral Case Study arthropathy) and tendons (enthesopathy). The clinical subsets of spondyloarthropathies constitute a wide spectrum, including: • Ankylosing spondylitis What does spondyloarthropathy • Psoriatic arthritis look like in a child? • Reactive arthritis • Inflammatory bowel disease associated with arthritis A 12-year-old boy is actively involved in sports. • Undifferentiated sacroiliitis When his right toe starts to hurt, overuse injury is Depending on the subtype, extra-articular manifestations might involve the eyes, thought to be the cause. The right toe eventually skin, lungs, gastrointestinal tract and heart. The most commonly accepted swells up, and he is referred to a rheumatologist to classification criteria for spondyloarthropathies are from the European evaluate for possible gout. Over the next few Spondyloarthropathy Study Group (ESSG). See Table 1. weeks, his right knee begins hurting as well. At the rheumatologist’s office, arthritis of the right second The juvenile spondyloarthropathies — which are the focus of this article — toe and the right knee is noted. Family history is might be defined as any spondyloarthropathy subtype that is diagnosed before remarkable for back stiffness in the father, which is age 17. It should be noted, however, that adult and juvenile spondyloar- reported as “due to sports participation.” thropathies exist on a continuum. In other words, many children diagnosed with a type of juvenile spondyloarthropathy will eventually fulfill criteria for Antinuclear antibody (ANA) and rheumatoid factor adult spondyloarthropathy. -
Olecranon Bursitis
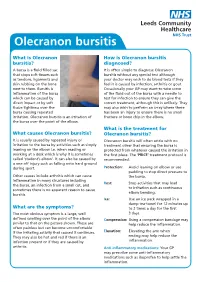
Olecranon bursitis What is Olecranon How is Olecranon bursitis bursitis? diagnosed? A bursa is a fluid filled sac It is often simple to diagnose Olecranon that stops soft tissues such bursitis without any special test although as tendons, ligaments and your doctor may wish to do blood tests if they skin rubbing on the bone feel it is caused by infection, arthritis or gout. next to them. Bursitis is Occasionally your GP may want to take some inflammation of the bursa of the fluid out of the bursa with a needle to which can be caused by test for infection to ensure they can give the direct impact or by soft correct treatment, although this is unlikely. They tissue tightness over the may also wish to perform an x-ray where there bursa causing repeated has been an injury to ensure there is no small irritation. Olecranon bursitis is an irritation of fracture or bone chip in the elbow. the bursa over the point of the elbow. What is the treatment for What causes Olecranon bursitis? Olecranon bursitis? It is usually caused by repeated injury or Olecranon bursitis will often settle with no irritation to the bursa by activities such as simply treatment other that ensuring the bursa is leaning on the elbow i.e. when reading or protected from whatever caused the irritation in working at a desk which is why it is sometimes the first place. The ‘PRICE’ treatment protocol is called ‘student’s elbow’. It can also be caused by recommended: a one off injury such as falling onto hard ground during sport. -

OES Site Color Scheme 1
Nuisance Problems You will Grow to Love Thomas V Gocke, MS, ATC, PA-C, DFAAPA President & Founder Orthopaedic Educational Services, Inc. Boone, NC [email protected] www.orthoedu.com Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. all rights reserved. Faculty Disclosures • Orthopaedic Educational Services, Inc. Financial Intellectual Property No off label product discussions American Academy of Physician Assistants Financial PA Course Director, PA’s Guide to the MSK Galaxy Urgent Care Association of America Financial Intellectual Property Faculty, MSK Workshops Ferring Pharmaceuticals Consultant Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. all rights reserved. 2 LEARNING GOALS At the end of this sessions you will be able to: • Recognize nuisance conditions in the Upper Extremity • Recognize nuisance conditions in the Lower Extremity • Recognize common Pediatric Musculoskeletal nuisance problems • Recognize Radiographic changes associates with common MSK nuisance problems • Initiate treatment plans for a variety of MSK nuisance conditions Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. all rights reserved. Inflammatory Response Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. all rights reserved. Inflammatory Response* When does the Inflammatory response occur: • occurs when injury/infection triggers a non-specific immune response • causes proliferation of leukocytes and increase in blood flow secondary to trauma • increased blood flow brings polymorph-nuclear leukocytes (which facilitate removal of the injured cells/tissues), macrophages, and plasma proteins to injured tissues *Knight KL, Pain and Pain relief during Cryotherapy: Cryotherapy: Theory, Technique and Physiology, 1st edition, Chattanooga Corporation, Chattanooga, TN 1985, p 127-137 Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. -

Single Injection May Quell Chronic Plantar Fasciitis
March 2006 • www.rheumatologynews.com Lupus/CT Diseases 27 Single Injection May Quell Chronic Plantar Fasciitis BY BRUCE JANCIN lief in nine such patients treated in open- try botulinum toxin A because of pub- greater than 4 on a 0-10 visual analog Denver Bureau label fashion. Based upon these highly en- lished reports citing its general analgesic scale. At week 2 this score was halved. At couraging results, a randomized, double- effect and inhibition of inflammatory pain. week 6 it was quartered. The same pattern V IENNA — Botulinum toxin A injection blind, and placebo-controlled clinical trial The nine patients selected for botu- of improvement was noted for maximum shows promise as a novel therapeutic op- is now planned, according to Dr. Placzek linum toxin A injection averaged age 55 pain during the previous 48 hours. tion for chronic plantar fasciitis patients of Charité Hospital, Berlin. years, with a 14-month history of plantar No muscle weakness or other adverse unresponsive to conventional treatments, Most patients with chronic plantar fasci- fasciitis refractory to all standard mea- events were observed, he noted at the Dr. Richard Placzek reported at the annual itis respond to physical therapy, cortico- sures. Follow-up evaluations were con- meeting sponsored by the European European Congress of Rheumatology. steroid injections, orthotics, acupuncture, ducted 2 weeks postinjection and every 1- League Against Rheumatism. Patients in- A single 200-unit injection into the and/or high-energy ultrasound extracor- 3 months thereafter up to 52 weeks. dicated they were satisfied with the pain painful region at the origin of the plantar poreal shock wave therapy. -

Bioarchaeological Implications of Calcaneal Spurs in the Medieval Nubian Population of Kulubnarti
Bioarchaeological Implications of Calcaneal Spurs in the Medieval Nubian Population of Kulubnarti Lindsay Marker Department of Anthropology Primary Thesis Advisor Matthew Sponheimer, Department of Anthropology Defense Committee Members Douglas Bamforth, Department of Anthropology Patricia Sullivan, Department of English University of Colorado at Boulder April 2016 1 Table of Contents List of Figures ............................................................................................................................. 4 Abstract …................................................................................................................................... 6 Chapter 1: Introduction …........................................................................................................... 8 Chapter 2: Anatomy …................................................................................................................ 11 2.1 Chapter Overview …................................................................................................. 11 2.2 Bone Composition …................................................................................................ 11 2.3 Plantar Foot Anatomy …........................................................................................... 12 2.4 Posterior Foot Anatomy …........................................................................................ 15 Chapter 3: Literature Review and Background of Calcaneal Enthesophytes ............................. 18 3.1 Chapter Overview …................................................................................................ -

Extracorporeal Shock Wave Treatment for Plantar Fasciitis and Other Musculoskeletal Conditions
Name of Blue Advantage Policy: Extracorporeal Shock Wave Treatment for Plantar Fasciitis and Other Musculoskeletal Conditions Policy #: 076 Latest Review Date: November 2020 Category: Medical Policy Grade: A BACKGROUND: Blue Advantage medical policy does not conflict with Local Coverage Determinations (LCDs), Local Medical Review Policies (LMRPs) or National Coverage Determinations (NCDs) or with coverage provisions in Medicare manuals, instructions or operational policy letters. In order to be covered by Blue Advantage the service shall be reasonable and necessary under Title XVIII of the Social Security Act, Section 1862(a)(1)(A). The service is considered reasonable and necessary if it is determined that the service is: 1. Safe and effective; 2. Not experimental or investigational*; 3. Appropriate, including duration and frequency that is considered appropriate for the service, in terms of whether it is: • Furnished in accordance with accepted standards of medical practice for the diagnosis or treatment of the patient’s condition or to improve the function of a malformed body member; • Furnished in a setting appropriate to the patient’s medical needs and condition; • Ordered and furnished by qualified personnel; • One that meets, but does not exceed, the patient’s medical need; and • At least as beneficial as an existing and available medically appropriate alternative. *Routine costs of qualifying clinical trial services with dates of service on or after September 19, 2000 which meet the requirements of the Clinical Trials NCD are considered reasonable and necessary by Medicare. Providers should bill Original Medicare for covered services that are related to clinical trials that meet Medicare requirements (Refer to Medicare National Coverage Determinations Manual, Chapter 1, Section 310 and Medicare Claims Processing Manual Chapter 32, Sections 69.0-69.11). -

The Painful Heel Comparative Study in Rheumatoid Arthritis, Ankylosing Spondylitis, Reiter's Syndrome, and Generalized Osteoarthrosis
Ann Rheum Dis: first published as 10.1136/ard.36.4.343 on 1 August 1977. Downloaded from Annals of the Rheumatic Diseases, 1977, 36, 343-348 The painful heel Comparative study in rheumatoid arthritis, ankylosing spondylitis, Reiter's syndrome, and generalized osteoarthrosis J. C. GERSTER, T. L. VISCHER, A. BENNANI, AND G. H. FALLET From the Department of Medicine, Division of Rheumatology, University Hospital, Geneva, Switzerland SUMMARY This study presents the frequency of severe and mild talalgias in unselected, consecutive patients with rheumatoid arthritis, ankylosing spondylitis, Reiter's syndrome, and generalized osteoarthosis. Achilles tendinitis and plantar fasciitis caused a severe talalgia and they were observed mainly in males with Reiter's syndrome or ankylosing spondylitis. On the other hand, sub-Achilles bursitis more frequently affected women with rheumatoid arthritis and rarely gave rise to severe talalgias. The simple calcaneal spur was associated with generalized osteoarthrosis and its frequency increased with age. This condition was not related to talalgias. Finally, clinical and radiological involvement of the subtalar and midtarsal joints were observed mainly in rheumatoid arthritis and occasionally caused apes valgoplanus. copyright. A 'painful heel' syndrome occurs at times in patients psoriasis, urethritis, conjunctivitis, or enterocolitis. with inflammatory rheumatic disease or osteo- The antigen HLA B27 was present in 29 patients arthrosis, causing significant clinical problems. Very (80%O). few studies have investigated the frequency and characteristics of this syndrome. Therefore we have RS 16 PATIENTS studied unselected groups of patients with rheuma- All of our patients had the complete triad (non- toid arthritis (RA), ankylosing spondylitis (AS), gonococcal urethritis, arthritis, and conjunctivitis). -

Sports Medicine Examination Outline
Sports Medicine Examination Content I. ROLE OF THE TEAM PHYSICIAN 1% A. Ethics B. Medical-Legal 1. Physician responsibility 2. Physician liability 3. Preparticipation clearance 4. Return to play 5. Waiver of liability C. Administrative Responsibilities II. BASIC SCIENCE OF SPORTS 16% A. Exercise Physiology 1. Training Response/Physical Conditioning a.Aerobic b. Anaerobic c. Resistance d. Flexibility 2. Environmental a. Heat b.Cold c. Altitude d.Recreational diving (scuba) 3. Muscle a. Contraction b. Lactate kinetics c. Delayed onset muscle soreness d. Fiber types 4. Neuroendocrine 5. Respiratory 6. Circulatory 7. Special populations a. Children b. Elderly c. Athletes with chronic disease d. Disabled athletes B. Anatomy 1. Head/Neck a.Bone b. Soft tissue c. Innervation d. Vascular 2. Chest/Abdomen a.Bone b. Soft tissue c. Innervation d. Vascular 3. Back a.Bone b. Soft tissue c. Innervation 1 d. Vascular 4. Shoulder/Upper arm a. Bone b. Soft tissue c. Innervation d. Vascular 5. Elbow/Forearm a. Bone b. Soft tissue c. Innervation d. Vascular 6. Hand/Wrist a. Bone b. Soft tissue c. Innervation d. Vascular 7. Hip/Pelvis/Thigh a. Bone b. Soft tissue c. Innervation d. Vascular 8. Knee a. Bone b. Soft tissue c. Innervation d. Vascular 9. Lower Leg/Foot/Ankle a. Bone b. Soft tissue c. Innervation d. Vascular 10. Immature Skeleton a. Physes b. Apophyses C. Biomechanics 1. Throwing/Overhead activities 2. Swimming 3. Gait/Running 4. Cycling 5. Jumping activities 6. Joint kinematics D. Pharmacology 1. Therapeutic Drugs a. Analgesics b. Antibiotics c. Antidiabetic agents d. Antihypertensives e. -

The Pathomechanics of Plantar Fasciitis
Sports Med 2006; 36 (7): 585-611 REVIEW ARTICLE 0112-1642/06/0007-0585/$39.95/0 2006 Adis Data Information BV. All rights reserved. The Pathomechanics of Plantar Fasciitis Scott C. Wearing,1 James E. Smeathers,1 Stephen R. Urry,1 Ewald M. Hennig2 and Andrew P. Hills1 1 Institute of Health and Biomedical Innovation, Queensland University of Technology, Kelvin Grove, Queensland, Australia 2 Biomechanik Labor, University Duisburg-Essen, Essen, Germany Contents Abstract ....................................................................................585 1. Anatomy of the Plantar Fascia ............................................................586 1.1 Gross Anatomy of the Plantar Fascia...................................................586 1.2 Histological Anatomy of the Plantar Fascia .............................................589 1.2.1 Neuroanatomy ................................................................590 1.2.2 Microcirculation ...............................................................590 1.2.3 The Enthesis ...................................................................590 2. Mechanical Properties of the Plantar Fascia ................................................592 2.1 Structural Properties ..................................................................593 2.2 Material Properties ...................................................................593 3. Mechanical Function of the Plantar Fascia .................................................594 3.1 Quasistatic Models of Plantar Fascial Function ..........................................594 -

Rotator Cuff and Subacromial Impingement Syndrome: Anatomy, Etiology, Screening, and Treatment
Rotator Cuff and Subacromial Impingement Syndrome: Anatomy, Etiology, Screening, and Treatment The glenohumeral joint is the most mobile joint in the human body, but this same characteristic also makes it the least stable joint.1-3 The rotator cuff is a group of muscles that are important in supporting the glenohumeral joint, essential in almost every type of shoulder movement.4 These muscles maintain dynamic joint stability which not only avoids mechanical obstruction but also increases the functional range of motion at the joint.1,2 However, dysfunction of these stabilizers often leads to a complex pattern of degeneration, rotator cuff tear arthropathy that often involves subacromial impingement.2,22 Rotator cuff tear arthropathy is strikingly prevalent and is the most common cause of shoulder pain and dysfunction.3,4 It appears to be age-dependent, affecting 9.7% of patients aged 20 years and younger and increasing to 62% of patients of 80 years and older ( P < .001); odds ratio, 15; 95% CI, 9.6-24; P < .001.4 Etiology for rotator cuff pathology varies but rotator cuff tears and tendinopathy are most common in athletes and the elderly.12 It can be the result of a traumatic event or activity-based deterioration such as from excessive use of arms overhead, but some argue that deterioration of these stabilizers is part of the natural aging process given the trend of increased deterioration even in individuals who do not regularly perform overhead activities.2,4 The factors affecting the rotator cuff and subsequent treatment are wide-ranging. The major objectives of this exposition are to describe rotator cuff anatomy, biomechanics, and subacromial impingement; expound upon diagnosis and assessment; and discuss surgical and conservative interventions.