Leg Length Inequality
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ankylosing Spondylitis
Page 1 of 4 Ankylosing Spondylitis Ankylosing spondylitis (AS) is a form of arthritis. It mainly affects the lower back. Other joints and other parts of the body are sometimes affected. Treatment includes regular exercise and anti-inflammatory drugs. The severity of AS varies from mild to severe. It is mild or moderate in most cases. What is ankylosing spondylitis? Spondylitis means inflammation of the spine. Ankylosing is a word that describes bones that tend to join together (fuse) across a joint. In ankylosing spondylitis (AS), the discs and ligaments of the lower spine become inflamed. The discs and ligaments are the strong tissues that connect the spinal bones (vertebrae) together. The joints between the lower spine and the pelvis (the sacro-iliac joints), and the small facet joints between the vertebrae are also commonly affected. Inflammation around the lower spine that persists long-term can cause scarring. This may, over time, cause some of the vertebrae in the spine to fuse together. In some cases, inflammation occurs in other joints and in other parts of the body outside of the spine (detailed below). Who gets ankylosing spondylitis? AS usually develops in teenagers or young adults. It rarely first develops after the age of 40. It is three times more common in men than women. There may be a family history with two or more members of a family being affected. About 1 in 1000 people in the UK have AS. What causes ankylosing spondylitis? The cause of AS is not known. There is a strong genetic (hereditary) part. Something may 'trigger' AS to develop in people who have an inherited tendency to have it. -

Ataxic Gait in Essential Tremor: a Disease-Associated Feature?
Freely available online Reviews Ataxic Gait in Essential Tremor: A Disease-Associated Feature? Ashwini K. Rao1* & Elan D. Louis2 1Department of Rehabilitation & Regenerative Medicine (Program in Physical Therapy), G.H. Sergievsky Center, Huntington's Disease Center of Excellence, Center of Excellence in Alzheimer's Disease, Columbia University, New York, NY, USA, 2Department of Neurology and Epidemiology (Chronic Diseases); Chief, Division of Movement Disorders, Co-Director- Center for Neuroepidemiology and Clinical Neurology Research, New Haven, CT, USA Abstract Background: While accumulating evidence suggests that balance and gait impairments are commonly seen in patients with essential tremor (ET), questions remain regarding their prevalence, their relationship with normal aging, whether they are similar to the impairments seen in spinocerebellar ataxias, their functional consequences, and whether some ET patients carry greater susceptibility. Methods: We conducted a literature search (until December 2018) on this topic. Results: We identified 23 articles on gait or balance impairments in ET. The prevalence of balance impairment (missteps on tandem walk test) was seven times higher in ET patients than controls. Gait impairments in ET included reduced speed, increased asymmetry, and impaired dynamic balance. While balance and gait problems worsened with age, ET patients were more impaired than controls, independent of age. The pattern of impairments seen in ET was qualitatively similar to that seen in spinocerebellar ataxias. Balance and gait impairments resulted in greater number of near falls in ET patients. Factors associated with balance and gait impairments in ET included age, presence of tremor in midline structures, and cognitive dysfunction. Discussion: Accumulating evidence suggests that balance and gait impairments are common in ET patients and occur to a greater extent in controls. -

Clinical and Radiographic Features of Spondylitic Hip Disease J
Ann Rheum Dis: first published as 10.1136/ard.38.4.332 on 1 August 1979. Downloaded from Annals of the Rheumatic Diseases, 1979, 38, 332-336 Clinical and radiographic features of spondylitic hip disease J. S. MARKS AND K. HARDINGE From the Rheumatology Unit and the Centre for Hip Surgery, Wrightington Hospital, Wigan, Lancs SUMMARY The clinical and radiographic features of hip disease in 76 patients with definite anky- losing spondylitis have been studied. Symptomatic hip involvement occurred late in the course of the disease, with a mean delay after the onset of 12 years in males and 7 years in females. Patients with disease onset before the age of 20 developed hip symptoms at an earlier stage. Associated diseases included uveitis (13 %), colitis (4 %), and psoriasis (4 %). Bilateral concentric loss of hip joint space with a relatively undeformed femoral head was the commonest radiological change (61 %). Localised loss ofjoint space at the upper pole (16 %) was associated with femoral head destruction and a greater degree of osteophytosis, suggesting coincidental or secondary osteoarthrosis. Bony ankylosis of the hips (10%) was present only in women, and the absence of osteophytes, cysts, and bone lesions of the iliac crests and ischial rami suggests that it is a distinct radiographic manifestation of female ankylosing spondylitis. copyright. Ankylosing spondylitis characteristically affects Clinical details obtained from the medical records the sacroiliac joints and the spine, but peripheral included age at onset of disease, site(s) of initial joint involvement occurs in at least 50% of patients symptoms, age at initial hip symptoms, associated during the course of their disease (Polley and diseases, previous medical and surgical treatment, Slocumb, 1947; Wilkinson and Bywaters, 1958; and details of hip surgery during admission. -

Hallux Valgus
MedicalContinuing Education Building Your FOOTWEAR PRACTICE Objectives 1) To be able to identify and evaluate the hallux abductovalgus deformity and associated pedal conditions 2) To know the current theory of etiology and pathomechanics of hallux valgus. 3) To know the results of recent Hallux Valgus empirical studies of the manage- ment of hallux valgus. Assessment and 4) To be aware of the role of conservative management, faulty footwear in the develop- ment of hallux valgus deformity. and the role of faulty footwear. 5) To know the pedorthic man- agement of hallux valgus and to be cognizant of the 10 rules for proper shoe fit. 6) To be familiar with all aspects of non-surgical management of hallux valgus and associated de- formities. Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Continu- ing Medical Education by the Council on Podiatric Medical Education. You may enroll: 1) on a per issue basis (at $15 per topic) or 2) per year, for the special introductory rate of $99 (you save $51). You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. In the near future, you may be able to submit via the Internet. If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earned credits. You will also receive a record of any incorrectly answered questions. If you score less than 70%, you can retake the test at no additional cost. A list of states currently honoring CPME approved credits is listed on pg. -

Bates' Pocket Guide to Physical Examination and History Taking
Lynn S. Bickley, MD, FACP Clinical Professor of Internal Medicine School of Medicine University of New Mexico Albuquerque, New Mexico Peter G. Szilagyi, MD, MPH Professor of Pediatrics Chief, Division of General Pediatrics University of Rochester School of Medicine and Dentistry Rochester, New York Acquisitions Editor: Elizabeth Nieginski/Susan Rhyner Product Manager: Annette Ferran Editorial Assistant: Ashley Fischer Design Coordinator: Joan Wendt Art Director, Illustration: Brett MacNaughton Manufacturing Coordinator: Karin Duffield Indexer: Angie Allen Prepress Vendor: Aptara, Inc. 7th Edition Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins. Copyright © 2009 by Wolters Kluwer Health | Lippincott Williams & Wilkins. Copyright © 2007, 2004, 2000 by Lippincott Williams & Wilkins. Copyright © 1995, 1991 by J. B. Lippincott Company. All rights reserved. This book is protected by copyright. No part of this book may be reproduced or transmitted in any form or by any means, including as photocopies or scanned-in or other electronic copies, or utilized by any information storage and retrieval system without written permission from the copyright owner, except for brief quotations embodied in critical articles and reviews. Materials appear- ing in this book prepared by individuals as part of their official duties as U.S. government employees are not covered by the above-mentioned copyright. To request permission, please contact Lippincott Williams & Wilkins at Two Commerce Square, 2001 Market Street, Philadelphia PA 19103, via email at [email protected] or via website at lww.com (products and services). 9 8 7 6 5 4 3 2 1 Printed in China Library of Congress Cataloging-in-Publication Data Bickley, Lynn S. Bates’ pocket guide to physical examination and history taking / Lynn S. -

Adult Still's Disease
44 y/o male who reports severe knee pain with daily fevers and rash. High ESR, CRP add negative RF and ANA on labs. Edward Gillis, DO ? Adult Still’s Disease Frontal view of the hands shows severe radiocarpal and intercarpal joint space narrowing without significant bony productive changes. Joint space narrowing also present at the CMC, MCP and PIP joint spaces. Diffuse osteopenia is also evident. Spot views of the hands after Tc99m-MDP injection correlate with radiographs, showing significantly increased radiotracer uptake in the wrists, CMC, PIP, and to a lesser extent, the DIP joints bilaterally. Tc99m-MDP bone scan shows increased uptake in the right greater than left shoulders, as well as bilaterally symmetric increased radiotracer uptake in the elbows, hands, knees, ankles, and first MTP joints. Note the absence of radiotracer uptake in the hips. Patient had bilateral total hip arthroplasties. Not clearly evident are bilateral shoulder hemiarthroplasties. The increased periprosthetic uptake could signify prosthesis loosening. Adult Stills Disease Imaging Features • Radiographs – Distinctive pattern of diffuse radiocarpal, intercarpal, and carpometacarpal joint space narrowing without productive bony changes. Osseous ankylosis in the wrists common late in the disease. – Joint space narrowing is uniform – May see bony erosions. • Tc99m-MDP Bone Scan – Bilaterally symmetric increased uptake in the small and large joints of the axial and appendicular skeleton. Adult Still’s Disease General Features • Rare systemic inflammatory disease of unknown etiology • 75% have onset between 16 and 35 years • No gender, race, or ethnic predominance • Considered adult continuum of JIA • Triad of high spiking daily fevers with a skin rash and polyarthralgia • Prodromal sore throat is common • Negative RF and ANA Adult Still’s Disease General Features • Most commonly involved joint is the knee • Wrist involved in 74% of cases • In the hands, interphalangeal joints are more commonly affected than the MCP joints. -

Arthritis in Myasthenia Gravis
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.38.11.1048 on 1 November 1975. Downloaded from Journal ofNeurology, Neurosurgery, and Psychiatry, 1975, 38, 1048-1055 Arthritis in myasthenia gravis J. A. AARLI1, E.-J. MILDE, AND S. THUNOLD From the Departments of Neurology and Pathology, School of Medicine, University of Bergen, and the Rheumatic Disease Unit, The Deaconesses' Hospital, Bergen, Norway SYNOPSIS Seven patients with myasthenia gravis developed clinical signs of arthropathy. In two patients, the symptoms were due to a deforming rheumatoid arthritis and the myasthenic symptoms appeared as a transitory phase during the course of the disease. Muscle antibodies of IgG class were demonstrated with sera from both patients. Autoreactivity between muscle antibodies and rheuma- toid factor was detected in one patient. Both patients died from sudden cardiac failure. Necropsy was performed in one and revealed a spotty myocardial necrosis. One patient had juvenile rheumatoid arthritis. Two patients had mild articular symptoms with indices of multivisceral disease and sero- logical findings indicating a systemic lupus erythematosus. One patient had classical ankylosing spondylitis, and one, unspecified arthropathy. guest. Protected by copyright. The concept of myasthenia gravis as a pure cate a clinical overlap (Oosterhuis and de Haas, disorder of the neuromuscular transmission has 1968). The aim of the present paper is a re- probably been an obstacle to the full delineation appraisal ofthe relationship between myasthenia of the clinical picture of this disease. Thus, care- gravis and arthritis. Seven patients are described ful clinical examination has revealed a series of and the data compared with relevant literature. -
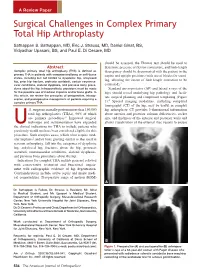
Surgical Challenges in Complex Primary Total Hip Arthroplasty
A Review Paper Surgical Challenges in Complex Primary Total Hip Arthroplasty Sathappan S. Sathappan, MD, Eric J. Strauss, MD, Daniel Ginat, BS, Vidyadhar Upasani, BS, and Paul E. Di Cesare, MD should be assessed, the Thomas test should be used to Abstract determine presence of flexion contracture, and limb-length Complex primary total hip arthroplasty (THA) is defined as discrepancy should be documented with the patient in the primary THA in patients with compromised bony or soft-tissue supine and upright positions (with use of blocks for stand- states, including but not limited to dysplastic hip, ankylosed hip, prior hip fracture, protrusio acetabuli, certain neuromus- ing, allowing the extent of limb-length correction to be 3 cular conditions, skeletal dysplasia, and previous bony proce- estimated). dures about the hip. Intraoperatively, provisions must be made Standard anteroposterior (AP) and lateral x-rays of the for the possible use of modular implants and/or bone grafts. In hips should reveal underlying hip pathology and facili- this article, we review the principles of preoperative, intraop- tate surgical planning and component templating (Figure erative, and postoperative management of patients requiring a 4 complex primary THA. 1). Special imaging modalities, including computed tomography (CT) of the hip, may be useful in complex .S. surgeons annually perform more than 150,000 hip arthroplasty. CT provides 3-dimensional information total hip arthroplasties (THAs), 90% of which about anterior and posterior column deficiencies, socket are primary procedures.1 Improved surgical size, and thickness of the anterior and posterior walls and technique and instrumentation have expanded allows visualization of the external iliac vessels to ensure Uthe clinical indications for THA to include patients who previously would not have been considered eligible for this procedure. -
Depression Prevalence in Postgraduate Students and Its Association with Gait Abnormality
SPECIAL SECTION ON DATA-ENABLED INTELLIGENCE FOR DIGITAL HEALTH Received November 7, 2019, accepted November 21, 2019, date of publication December 2, 2019, date of current version December 16, 2019. Digital Object Identifier 10.1109/ACCESS.2019.2957179 Depression Prevalence in Postgraduate Students and Its Association With Gait Abnormality JING FANG 1, TAO WANG 2, (Student Member, IEEE), CANCHENG LI 2, XIPING HU 1,2, (Member, IEEE), EDITH NGAI 3, (Senior Member, IEEE), BOON-CHONG SEET 4, (Senior Member, IEEE), JUN CHENG 1, YI GUO 5, AND XIN JIANG 6 1Shenzhen Institutes of Advanced Technology, Chinese Academy of Sciences, Shenzhen 518055, China 2School of Information Science and Engineering, Lanzhou University, Gansu 730000, China 3Department of Information Technology, Uppsala University, Uppsala 75105, Sweden 4Department of Electrical and Electronic Engineering, Auckland University of Technology, Auckland 1010, New Zealand 5Department of Neurology, Shenzhen People's Hospital, Second Clinical Medical College of Jinan University, First Affiliated Hospital of Southern University of Science and Technology, Shenzhen 518020, China 6Department of Geriatrics, Shenzhen People's Hospital, Second Clinical Medical College of Jinan University, First Affiliated Hospital of Southern University of Science and Technology, Shenzhen 518020, China Corresponding authors: Xiping Hu ([email protected]) and Xin Jiang ([email protected]) This work was supported in part by Shenzhen Technology under Project JSGG20170413171746130, in part by the National Natural Science Foundation of China under Grant 61632014, Grant 61802159, Grant 61210010, Grant 61772508, and Grant 61402211, and in part by the Program of Beijing Municipal Science and Technology Commission under Grant Z171100000117005. ABSTRACT In recent years, an increasing number of university students are found to be at high risk of depression. -

The Role of Arthroscopic Adhesiolysis in the Treatment of the Arthrofibrosis and the Partial Ankylosis of the Knee
Acta Orthop Traumatol Turc 28, 379-383 , 1994 The role of arthroscopic adhesiolysis in the treatment of the arthrofibrosis and the partial ankylosis of the knee Metin Lütfü Saydartl), Ethem Gür1l ), Vecihi Kırdemir1 l ), Ali Saib Engin(1) Dizin parsiyel ankilozu ve artrofibrozisinin tedavisinde artroskopik adezyolizisin rolü Travma, klf/k yada distal femur cerrahi girişim ardından gelişen diz hareketi kısıtlanan 23 hastanın 27 dizi, artroskopik kontrol altında , perkutan adezyon releasei ile tedavi edildi. Diz hareketlerini kısıtlayan neden ile artroskopik adezyolizis arasındaki dönem 4 ile 24 ay (ortalama 7 ay) arasında değişiyordu. Ortalama preope ratif diz hareketi 43°, ortalama postop diz hareketi IIS°'ydi. Ortalama postoperatif hareket kaybı 17"'ydi. Takip sonunda ortalama hareket kazancı SS°'ydi. Anahtar kelimeler: Artroskopi, artrofibrozis, adezyolizis, diz, ankiloz The role of arthroscopic adhesiolysis in the treatment of the arthrofibrosis and the partial ankylosis of theknee The 27 knees of 23 patients with limited range of motion that developed after trauma, fractures or open surgical procedures of the distal femur were treated by the percutaneous release of the adhesions under art hroscopic control. The inteNal between the cause of the limited ROM and the arthroscopic adhesiolysis ran ged from 4 months to 24 months (mean: 7 months). The average preoperative ROM was 43° and the average postoperative ROM was 115°. The average loss from the postoperative ROM was 1r. At the fol/ow-up, the average final gain of ROM was 55°. Keywords: Arthroscopy, arthrofibrosis, adhesiolysis, knee, ankylosis. The pathogenesis of arthrofibrosis is not a single Another subgroup of the post-traumatic arthrofib process but there are multiple factors that play roles rosis is the Infrapatellar Contracture Syndrome in this procedure. -

Gait Disorders in Older Adults
ISSN: 2469-5858 Nnodim et al. J Geriatr Med Gerontol 2020, 6:101 DOI: 10.23937/2469-5858/1510101 Volume 6 | Issue 4 Journal of Open Access Geriatric Medicine and Gerontology STRUCTURED REVIEW Gait Disorders in Older Adults - A Structured Review and Approach to Clinical Assessment Joseph O Nnodim, MD, PhD, FACP, AGSF1*, Chinomso V Nwagwu, MD1 and Ijeoma Nnodim Opara, MD, FAAP2 1Division of Geriatric and Palliative Medicine, Department of Internal Medicine, University of Michigan Medical School, USA Check for 2Department of Internal Medicine and Pediatrics, Wayne State University School of Medicine, USA updates *Corresponding author: Joseph O Nnodim, MD, PhD, FACP, AGSF, Division of Geriatric and Palliative Medicine, Department of Internal Medicine, University of Michigan Medical School, 4260 Plymouth Road, Ann Arbor, MI 48109, USA Abstract has occurred. Gait disorders are classified on a phenom- enological scheme and their defining clinical presentations Background: Human beings propel themselves through are described. An approach to the older adult patient with a their environment primarily by walking. This activity is a gait disorder comprising standard (history and physical ex- sensitive indicator of overall health and self-efficacy. Impair- amination) and specific gait evaluations, is presented. The ments in gait lead to loss of functional independence and specific gait assessment has qualitative and quantitative are associated with increased fall risk. components. Not only is the gait disorder recognized, it en- Purpose: This structured review examines the basic biolo- ables its characterization in terms of severity and associated gy of gait in term of its kinematic properties and control. It fall risk. describes the common gait disorders in advanced age and Conclusion: Gait is the most fundamental mobility task and proposes a scheme for their recognition and evaluation in a key requirement for independence. -

Direct Anterior Total Hip Arthroplasty Gait Biomechanics at Three and Six Months Post Surgery
DIRECT ANTERIOR TOTAL HIP ARTHROPLASTY GAIT BIOMECHANICS AT THREE AND SIX MONTHS POST SURGERY A THESIS SUBMITTED TO THE GRADUATE DIVISION OF THE UNIVERSITY OF HAWAI’I IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF SCIENCE IN KINESIOLOGY AND REHABILITATION SCIENCE AUGUST 2012 By: Ryan J. Moizon Thesis Committee: Iris Kimura, Chairperson Ronald Hetzler Christopher Stickley Keywords: Total hip arthroplasty; kinematics; kinetics TABLE OF CONTENTS List of Tables ii List of Figures iii Part I Introduction 1 Methods 4 Results 7 Discussion 12 Partil Review of literature 19 Appendix A: Data Collection Forms 37 Appendix B: Health History Form 40 Appendix C: WWB THA Informed Consent Form 42 Appendix D: WRB Control Informed Consent Form 53 Appendix F: Control Flyer 62 References 64 LIST OF TABLES Table Page 1. Demographic Data: Means and Standard Deviations for DA THA and Control group 7 2. Walking Velocity: Means and Standard Deviations for DA THA and Control group $ 3. Kinematic Variables: Mean and standard deviations for DA THA and Control group 9 4. Kinetic Variables: Mean and standard deviations for DA-THA and Control groups 11 5. Maximum VGRF: Means and Standard Deviations for DA THA and Control groups 11 LIST OF FIGURES Figure Page 1. Mean Values for Walking Velocity for DA THA and Control groups at initial test, 3 and 6 months post-test 13 2. Mean Values for Hip FlexionlExtension Excursion for DA THA and Control groups at initial test, 3 and 6 months post-test 14 3. Mean Values for Maximum VGRF for DA THA and Control groups at initial test, 3 and 6 months post-test 15 4.