Netsforlife Malaria Prevention Programme
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Eastern Province
SIERRA LEONE EASTERN PROVINCE afi B or B a fi n Guinea Guinea KOINADUGU KAMBIA BOMBALI ! PORT LOKO KONO Fandaa TONKOLILI 5 ! Henekuma WESTERN AREA ! Dunamor ! ! Powma KAILAHUN Fintibaya ! Siakoro MOYAMBA BO ! Konkonia ! Kondewakor Kongowakor !! KENEMA ! ! Saikuya ! M!okeni K! ongoadu Bongema II ! Poteya ! ! ! T o l i ! Komandor T o l i Kombodu ! ! ! ! ! ! Kondeya Fabandu Foakor ! !! BONTHE Thomasidu Yayima Fanema ! Totor ! !! Bendu Leimaradu ! ! ! Foindu ! ! Gbolia PUJEHUN !!Feikaya Sakamadu ! ! Wasaya! Liberia Bayawaindu ! Bawadu Jongadu Sowadu ! Atlantic Ocean Norway Bettydu ! ! Kawamah Sandia! ! ! ! ! ! Kamindo ! !! ! ! Makongodu ! Sam! adu Bondondor ! ! Teiya ! ! ! ! Wonia ! Tombodu n Primary School ! ! e wordu D Wordu C Heremakonoh !! ! !! ! Yendio-Bengu ! d !! Kwafoni n ! !Dandu Bumanja !Kemodu ! ! e ! Yaryah B Yuyah Mor!ikpandidu ! ! S ! ! ! ! ! Kondeya II ! r ! ! ! ! !! Kindia o ! ! Deiyor! II Pengidu a Makadu Fosayma Bumbeh ! ! an Kabaidu ! Chimandu ! ! ! Yaryah A ! Kondeya Kongofinkor Kondeya Primary School ! Sambaia p ! ! ! F!aindu m Budu I !! Fodaydu ! ! Bongema I a !Yondadu !Kocheo ! Kwakoima ! Gbandu P Foimangadu Somoya ! ! Budu II ! ! ! Koyah ! Health Centre Kamba ! ! Kunundu Wasaya ! ! ! ! Teidu ! Seidu Kondeya 1 ! ! Kayima A ! Sandema! ! ! suma II suma I Primary School ! ! ! ! Kayima B Koidundae !!! R.C. Primary School ! ! ! !! Wokoro UMC Primary School !! Sangbandor Tankoro ! ! Mafidu ! Dugbema ! Piyamanday ! Suma I Bendu ! Kayima D ! ! Kwikuma Gbeyeah B ! Farma Bongema ! Koekuma ! Gboadah ! ! ! ! Masaia ! Gbaiima Kombasandidu -
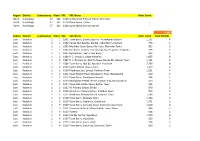
Region District Constituency Ward VRC VRC Name Voter Count North
Region District Constituency Ward VRC VRC Name Voter Count North Koinadugu 47 162 6169 Al-Harrakan Primary School, Woredala - North Koinadugu 47 162 6179 Open Space 2,Kabo - North Koinadugu 47 162 6180 Open Space, Kamayortortor - 9,493 Region District Constituency Ward VRC VRC Name Voter Count Total PS(100) East Kailahun 1 1 1001 Town Barry, Baoma, Baoma - Kunywahun Section 1,192 4 East Kailahun 1 1 1002 Palava Hut, Baoma, Baoma - Gborgborma Section 478 2 East Kailahun 1 1 1003 Mofindor Court Barry, Mofindor, Mofindor Town 835 3 East Kailahun 1 1 1004 Methodist primary school yengema, Yengama, Yengema 629 2 East Kailahun 1 1 1005 Nyanyahun Town, Town Barry 449 2 East Kailahun 1 2 1006 R. C. School 1, Upper Masanta 1,855 6 East Kailahun 1 2 1007 R. C. Primary 11, Gbomo Town, Buedu RD, Gbomo Town 1,121 4 East Kailahun 1 2 1008 Town Barry, Ngitibu, Ngitibu 1-Kailahum 2,209 8 East Kailahun 1 2 1009 KLDEC School, new London 1,259 4 East Kailahun 1 2 1010 Methodist Sec. School, Kailahun Town 1,031 4 East Kailahun 1 2 1011 Town Market Place, Bandajuma Town, Bandajuma 640 2 East Kailahun 1 2 1012 Town Barry, Bandajuma Sinneh 294 1 East Kailahun 1 2 1013 Bandajuma Health Centre, Luawa Foiya, Bandajuma Si 473 2 East Kailahun 1 2 1014 Town Hall, Borbu-Town, Borbu- Town 315 1 East Kailahun 1 2 1015 RC Primary School, Borbu 870 3 East Kailahun 1 2 1016 Amadiyya Primary School, Kailahun Town 973 3 East Kailahun 1 2 1017 Methodist Primary School, kailahun Town 1,266 4 East Kailahun 1 3 1018 Town Barry, Sandialu Town 1,260 4 East Kailahun 1 3 1019 Town -

Sierra Leone
Language: English Original: English PROJECT: REHABILITATION OF BO-BANDAJUMA ROAD COUNTRY: SIERRA LEONE ENVIRONMENTAL AND SOCIAL IMPACT ASSESSMENT SUMMARY Date: August 2015 Team Leader: : A. Mwila, Transport Engineer, OITC.1 Team Members: A. Bockarie , Transport Engineer, OITC.1/SLFO J. Aguma. Transport Economist, OITC.1 F. Koroma, Financial Management Specialist, ORPF.2 A. Abdulai, Financial Management Specialist, ORPF.2 A Nabaloga, Social Development Specialist, Consultant, ONEC.3 M. Jambawai Social Expert, OSHD S. Momoh , Procurement Officer, ORPF.1 / SLFO P. Tambah,, Transport Engineer, OITC.1/LRFO Appraisal Team N. Omagor, Environmental Specialist, Consultant, OITC.1 Sector Manager: J. Kabanguka Country Manager: Y. Baldeh Sector Director: A. Oumarou Regional Director: A. Bernoussi 1 Project Title : Rehabilitation of Bo-Bandajuma Road Project Number : P-SL-DB0-010 Country : Sierra Leone Department : Transport & ICT Department (OITC) Division : OITC.1 1. Introduction The project involves the update of feasibility studies of the road from Bo to Bandajuma in the southeast of Sierra Leone, which is part of the Freetown-Monrovia Trans-West African Coastal Highway. The rehabilitation of Bo-Bandajuma road will involve overlaying Asphalt Concrete on the existing carriage way without major realignments. However, in most trading centers, roadside businesses have encroached on the carriageway which has triggered the need for resettlement and compensation. On the state of the road, it be briefly noted that, from the Bo towards Bandajuma and for its first 3.5km, the road deterioration has ranged from loss of paved surfaces, to development of gaping pot holes, stretches of mudflats and some impassable sections. The main areas of deterioration are within 15 km from Bo with a worst portion with glaring potholes at 24+000km. -

Religion, Chieftaincy, and Post-Conflict Reintegration in Sierra Leone
University of Calgary PRISM: University of Calgary's Digital Repository Graduate Studies The Vault: Electronic Theses and Dissertations 2013-09-23 Unusual Suspects: Religion, Chieftaincy, and Post-Conflict Reintegration in Sierra Leone Berriault, Tobey Berriault, T. (2013). Unusual Suspects: Religion, Chieftaincy, and Post-Conflict Reintegration in Sierra Leone (Unpublished master's thesis). University of Calgary, Calgary, AB. doi:10.11575/PRISM/28594 http://hdl.handle.net/11023/994 master thesis University of Calgary graduate students retain copyright ownership and moral rights for their thesis. You may use this material in any way that is permitted by the Copyright Act or through licensing that has been assigned to the document. For uses that are not allowable under copyright legislation or licensing, you are required to seek permission. Downloaded from PRISM: https://prism.ucalgary.ca UNIVERSITY OF CALGARY Unusual Suspects: Religion, Chieftaincy, and Post-Conflict Reintegration in Sierra Leone by Tobey Evonne Berriault A THESIS SUBMITTED TO THE FACULTY OF GRADUATE STUDIES IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF ARTS DEPARTMENT OF POLITICAL SCIENCE CALGARY, ALBERTA SEPTEMBER, 2013 © Tobey Evonne Berriault 2013 Abstract This thesis is concerned with the long-term reintegration of Sierra Leone’s ex-combatants. Using the indicators of education, employment, inter-marriage, social stigma, and crime, this thesis argues that the long-term social, economic, and political reintegration of Sierra Leone’s ex- combatants has been widely successful. This research then identifies the initiatives of pre- existing civil society organizations (CSOs) in the form of mosques, churches, and the Inter- Religious Council of Sierra Leone as the primary facilitators of this success. -

Payment of Tuition Fees to Primary Schools in Bo District for Second Term 2019/2020 School Year
PAYMENT OF TUITION FEES TO PRIMARY SCHOOLS IN BO DISTRICT FOR SECOND TERM 2019/2020 SCHOOL YEAR Amount NO. EMIS Name Of School Region District Chiefdom Address Headcount Total to School Per Child 1 311301222 Abdul Tawab Haikal Primary School South BO District Tikonko Samie 610 10000 6,100,000 Bo Kenema 2 319103274 Agape Way Christian Primary School South BO District Kakua 380 10000 Highway 3,800,000 3 311401201 Ahmadiyya Muslim Primary South BO District Valunia Baomahun 822 10000 8,220,000 4 310702210 Ahmadiyya Muslim Primary South BO District Jaima Koribondo 341 10000 3,410,000 5 310202206 Ahmadiyya Muslim Primary South BO District Bagbo Levuma 203 10000 2,030,000 Bumpe 6 310502209 Ahmadiyya Muslim Primary South BO District Makayoni 215 10000 Ngao 2,150,000 7 311401218 Ahmadiyya Muslim Primary South BO District Valunia Mandu 221 10000 2,210,000 8 310201205 Ahmadiyya Muslim Primary South BO District Bagbo Momajoe 338 10000 3,380,000 Bumpe 9 310503217 Ahmadiyya Muslim Primary South BO District Walihun 264 10000 Ngao 2,640,000 Baoma 10 310403210 Ahmadiyya Muslim Primary School South BO District Baoma 122 10000 Gbandi 1,220,000 Kenema 11 311401209 Ahmadiyya Muslim Primary School South BO District Valunia 330 10000 Blango 3,300,000 12 311001208 Ahmadiyya Muslim Primary School South BO District Lugbu Kpatobu 244 10000 2,440,000 13 310702215 Ahmadiyya Muslim Primary School South BO District Jaiama Kpetema 212 10000 2,120,000 14 310402205 Ahmadiyya Muslim Primary School South BO District Baoma Ndogbogoma 297 10000 2,970,000 15 310201211 Ahmadiyya -

World Bank Document
SMALLHOLDER COMMERCIALIZATION AND AGRIBUSINESS DEVELOPMENT PROJECT (SCADeP) JOB NUMBER SIE4023 RFP No.: MAFFS/PCU/SCADeP/QCBS/01/02/2017 Public Disclosure Authorized REPORT TITLE: ENVIRONMENTAL, SOCIAL AND HEALTH IMPACT ASSESSMENT FOR THE REHABILITATION OF 500KM OF FEEDER ROADS IN 13 DISTRICTS, IN SIERRA LEONE - ESHIA REPORT DATE: JUNE 2018 This report is own by the Government of Sierra Leone for the project Prioritization and Assessment Study to Improve Selected Feeder Roads (500km) including Preparation of Bidding Documents using Output and Performance Based Contract (OPRC) and Traditional Contract in Sierra Leone Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized CERTIFICATION REPORT TITLE: ENVIRONMENTAL, SOCIAL AND HEALTH IMPACT ASSESSMENT FOR THE PROPOSED 500KM FEEDER ROADS IMPROVEMENT IN 13 DISTRICTS IN SIERRA LEONE Signed: _____________________________ Date: ____25/09/2018____________ For: RIL/ICS Disclaimer: This ESIA Report is strictly confidential to the Proponent and any use of the materials thereof should be strictly in accordance with agreement between the Proponent and the GoSL. It is, however, subject to conditions in the Environmental (Impact Assessment) Regulations, EPA-SL Act of 2008 and amended in 2010. Acronym ABC Agri-Business Centres CDAP Community Development Action Plan CHP Community Health Post EIA Environmental Impact Assessment ESMMP Environmental and Social Management and Monitoring Plan EIS Environmental Impact Statement ESMP Environmental and Social Management Plan EPA-SL -
Local Council Ward Boundary Delimitation Report
April 2008 NATIONAL ELECTORAL COMMISSION Sierra Leone Local Council Ward Boundary Delimitation Report Volume One February 2008 This page is intentionally left blank TABLE OF CONTENTS Foreword 1 Executive Summary 3 Introduction 5 Stages in the Ward Boundary Delimitation Process 7 Stage One: Establishment of methodology including drafting of regulations 7 Stage Two: Allocation of Local Councils seats to localities 13 Stage Three: Drawing of Boundaries 15 Stage Four: Sensitization of Stakeholders and General Public 16 Stage Five: Implement Ward Boundaries 17 Conclusion 18 APPENDICES A. Database for delimiting wards for the 2008 Local Council Elections 20 B. Methodology for delimiting ward boundaries using GIS technology 21 B1. Brief Explanation of Projection Methodology 22 C. Highest remainder allocation formula for apportioning seats to localities for the Local Council Elections 23 D. List of Tables Allocation of 475 Seats to 19 Local Councils using the highest remainder method 24 25% Population Deviation Range 26 Ward Numbering format 27 Summary Information on Wards 28 E. Local Council Ward Delimitation Maps showing: 81 (i) Wards and Population i (ii) Wards, Chiefdoms and sections EASTERN REGION 1. Kailahun District Council 81 2. Kenema City Council 83 3. Kenema District Council 85 4. Koidu/New Sembehun City Council 87 5. Kono District Council 89 NORTHERN REGION 6. Makeni City Council 91 7. Bombali District Council 93 8. Kambia District Council 95 9. Koinadugu District Council 97 10. Port Loko District Council 99 11. Tonkolili District Council 101 SOUTHERN REGION 12. Bo City Council 103 13. Bo District Council 105 14. Bonthe Municipal Council 107 15. -
Appeal Tel: 41 22 791 6033 Fax: 41 22 791 6506 E-Mail: [email protected]
150 route de Ferney, P.O. Box 2100 1211 Geneva 2, Switzerland Appeal Tel: 41 22 791 6033 Fax: 41 22 791 6506 e-mail: [email protected] Sierra Leone Coordinating Office Relief & Rehabilitation – AFSL-21 Appeal Target: US$ 5,373,216 Balance Requested from ACT Network: US$ 5,171,502 Geneva, 11 December 2001 Dear Colleagues, Good progress is being made in the disarmament programme with the third phase of disarmament and demobilisation of 25,000 combatants having been expected to be completed by the end of November 2001. UNAMISIL has been deployed since May 2001, most recently entering the diamond-rich eastern area of Sierra Leone. The British trained government army, SLA, is also being deployed in other RUF areas such as Kambia in the North and vicinities to the East of Kenema. The concern however, is whether the SL government has capacity to deliver public services in newly disarmed areas as these services would be key to building confidence and sustainable peace in the communities. Humanitarian needs in the country are very high as the war has decimated the basic infrastructure and the levels of psychological trauma amongst the population is high. As previously rebel-held areas open up, displaced populations are returning to their original communities. Most lack the basics such as clothing, medication and shelter. In addition, there are tens of thousands of returnees from neighbouring countries increasing the challenges in the humanitarian sector. The returnees are living in temporary camps and congested urban areas, where local authorities cannot meet basic needs. There is a tremendous challenge for the international community to work with these communities to re-establish access to basic services such as healthcare, education and sanitation and to revitalise local economies. -

U N I T E D N a T I O
U N I T E D N A T I O N S Office for the Coordination of Humanitarian Affairs SIERRA LEONE HUMANITARIAN SITUATION REPORT SEPTEMBER 2003 KEY EVENTS district. A concern raised in Kono is that none of the Watsan implementing partners had the facilities or machines for testing water • Yellow Fever outbreak samples. This has been reported to the MOHS. • Security Council extends UNAMSIL’s mandate • UN Agencies and GoSL celebrate World Peace Day SECURITY HIGHLIGHTS • Nigerian lawmakers call on UNAMSIL Overall security UNAMSIL (United Nations Mission in Sierra Leone) reports the overall security situation in HUMANITARIAN HIGHLIGHTS the country to be calm. However there have been some concerns about security along the Yellow Fever outbreak border regions, particularly along the Mano The Ministry of Health and Sanitation (MOHS) River Union Bridge in the south. Similarly the has reported a total of 90 cases of Yellow Sierra Leone Police (SLP) are concerned Fever, from eight districts in the country: about the porous nature of the border in the Tonkolili, Bombali, Kenema, Koinadugu, Port Kamakwie, Tambakha and Koinadugu areas, Loko, Kambia and Kono. Of the 90 reported in the Northern Province that have resulted in cases (as of 29 September) four laboratory increased smuggling of goods across the cases were confirmed, all from the Tonkolili borders. The police have also reported hunters District, where majority of the suspected cases from Guinea, coming across, poaching and emanate from. Earlier, the MOHS gave out crossing back into Guinea. 100,000 doses of vaccine in four chiefdoms in the district. They have now finally secured UNAMSIL’s mandate extended funds to carry out mass immunization The UN Security Council has extended campaign in the remaining seven chiefdoms of UNAMSIL’s mandate, which was to expire on the district. -

(Smes) As Agent of National Development in Sierra Leone
International Journal of Science and Research (IJSR) ISSN (Online): 2319-7064 Index Copernicus Value (2015): 78.96 | Impact Factor (2015): 6.391 Small and Medium Scale Enterprises (SMEs) as Agent of National Development in Sierra Leone Momodu Sahid Kanu, Bob Karankay Conteh School Of Agriculture, Njala University, Njala Campus, Private Mail Bag, Freetown, Sierra Leone, West Africa University of Makeni Abstract: This study, Small and Medium Enterprises (SMEs) as agent of national development was undertaken in Bo district. In all, 470 small and medium business enterprise owners were selected randomly and interviewed using questionnaires. Other methods of data collection were desk survey and observation; Data collected were analyzed using Statistical Package for Social Sciences (SPSS 16 and 23) applied on the data. A number of results, indices, frequency distributions, chi-square correlation, contingency tables, p-values, tests statistics etc., were generated with several interactions. The overall objective of this study is to identify the effect of SMEs as agents of national development and based on the findings make recommendations for the improvement of the performances of the business. The findings showed that most of the small and medium business owners were Sierra Leoneans (91.7%) and the rest were Guineans (8.2%) and Lebanese (8.2%).The majority of the respondents were in their productive age. Most of them were not educated; those educated had primary and/or secondary education. The respondents were fairly spread across a wide range of sectors, less than three-fourths of the sectors.(71.1%) in the economy, majority of them came from; Export 8(2.0%), services 187(38.9%), manufacturing 72(15.3%) and Trading 70(14.9%) and the others (28.4%). -

World Bank Document
wkjjk Public Disclosure Authorized Public Disclosure Authorized A Simplified Handbook on the Government of Sierra Leone’s Public Disclosure Authorized New Operational Procedures and Guidelines For the Diamond Area Community Development Fund (DACDF) Public Disclosure Authorized Designed by the World Bank Justice for the Poor (J4P) in partnership with Network Movement for Justice and Development (NMJD) DACDF means Diamond Area Community Development Fund. The DACDF was set up by the government of Sierra Leone in the year 2001. Since that time every year the government puts some money into the fund for distribution among diamond mining chiefdoms in the country. Government of Sierra Leone Sets up D.A.C.D. Fund Le. Government of Sierra Leone sets up the DACDF Why did government introduce the Diamond Area Community Development Fund? There are several reasons for which the government introduced the DACDF, but the most important ones are: (1) After the civil war, government thought it necessary to give back some of the money it gets from the sale of diamonds to chiefdoms in the country where diamonds are mined so that these chiefdoms will use that money to carry out development projects in their towns and villages. (2) Government also wanted to encourage the chiefs and other local leaders in mining chiefdoms in the country to help reduce, or put stop to bad mining practices like diamond smuggling, mining without license, and other forms of illegal mining. Does government give the DACDF money to districts or chiefdoms that do not have diamonds? No. As the name goes “Diamond Area Community Development Fund”. -

Copyright © and Moral Rights for This Thesis Are Retained by the Author And/Or Other Copyright Owners
R Tarawallie, Idrissa Mamoud (2018) Public services and social cohesion at risk? : the political economy of democratic decentralisation in post‐war Sierra Leone (2004‐2014). PhD thesis. SOAS University of London. http://eprints.soas.ac.uk/26185 Copyright © and Moral Rights for this thesis are retained by the author and/or other copyright owners. A copy can be downloaded for personal non‐commercial research or study, without prior permission or charge. This thesis cannot be reproduced or quoted extensively from without first obtaining permission in writing from the copyright holder/s. The content must not be changed in any way or sold commercially in any format or medium without the formal permission of the copyright holders. When referring to this thesis, full bibliographic details including the author, title, awarding institution and date of the thesis must be given e.g. AUTHOR (year of submission) "Full thesis title", name of the School or Department, PhD Thesis, pagination. Public Services and Social Cohesion at Risk? The Political Economy of Democratic Decentralisation in Post-War Sierra Leone (2004 – 2014) Idrissa Mamoud Tarawallie Thesis submitted for the degree of PhD Department of Development Studies SOAS – University of London February 2017 1 Abstract On account of the many failures of the centralised state, decentralisation has become the preferred mode of governance in many countries in the developing world. Widely supported by international development agencies, it promises efficiency and equity in public service delivery and social cohesion in post-war societies by bringing government closer to the people. Crucial in the decentralisation promise, is resource diversion through clientelistic networks at the local level to consolidate political strongholds.