Cameroon Operational Plan (COP)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Monitoring of HIV Viral Load, CD4 Cell Count, and Clinical Assessment
Articles Monitoring of HIV viral load, CD4 cell count, and clinical assessment versus clinical monitoring alone for antiretroviral therapy in low-resource settings (Stratall ANRS 12110/ESTHER): a cost-eff ectiveness analysis Sylvie Boyer, Laura March, Charles Kouanfack, Gabrièle Laborde-Balen, Patricia Marino, Avelin Fobang Aghokeng, Eitel Mpoudi-Ngole, Sinata Koulla-Shiro, Eric Delaporte, Maria Patrizia Carrieri, Bruno Spire, Christian Laurent, Jean-Paul Moatti, on behalf of the Stratall ANRS 12110/ESTHER Study Group* Summary Background In low-income countries, the use of laboratory monitoring of patients taking antiretroviral therapy Lancet Infect Dis 2013; (ART) remains controversial in view of persistent resource constraints. The Stratall trial did not show that clinical 13: 577–86 monitoring alone was non-inferior to laboratory and clinical monitoring in terms of immunological recovery. We Published Online aimed to evaluate the costs and cost-eff ectiveness of the ART monitoring approaches assessed in the Stratall trial. April 18, 2013 http://dx.doi.org/10.1016/ S1473-3099(13)70073-2 Methods The randomised, controlled, non-inferiority Stratall trial was done in a decentralised setting in Cameroon. See Comment page 560 Between May 23, 2006, and Jan 31, 2008, ART-naive adults were randomly assigned (1:1) to clinical monitoring *Members listed at end of paper (CLIN) or viral load and CD4 cell count plus clinical monitoring (LAB) and followed up for 24 months. We INSERM, UMR912 (SESSTIM), calculated costs, number of life-years saved (LYS), and incremental cost-eff ectiveness ratios (ICERs) with data Marseille, France (S Boyer PhD, from patients who had been followed up for at least 6 months. -

Shelter Cluster Dashboard NWSW052021
Shelter Cluster NW/SW Cameroon Key Figures Individuals Partners Subdivisions Cameroon 03 23,143 assisted 05 Individual Reached Trend Nigeria Furu Awa Ako Misaje Fungom DONGA MANTUNG MENCHUM Nkambe Bum NORD-OUEST Menchum Nwa Valley Wum Ndu Fundong Noni 11% BOYO Nkum Bafut Njinikom Oku Kumbo Belo BUI Mbven of yearly Target Njikwa Akwaya Jakiri MEZAM Babessi Tubah Reached MOMO Mbeggwi Ngie Bamenda 2 Bamenda 3 Ndop Widikum Bamenda 1 Menka NGO KETUNJIA Bali Balikumbat MANYU Santa Batibo Wabane Eyumodjock Upper Bayang LEBIALEM Mamfé Alou OUEST Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Fontem Nguti KOUPÉ HNO/HRP 2021 (NW/SW Regions) Toko MANENGOUBA Bangem Mundemba SUD-OUEST NDIAN Konye Tombel 1,351,318 Isangele Dikome value Kumba 2 Ekondo Titi Kombo Kombo PEOPLE OF CONCERN Abedimo Etindi MEME Number of PoC Reached per Subdivision Idabato Kumba 1 Bamuso 1 - 100 Kumba 3 101 - 2,000 LITTORAL 2,001 - 13,000 785,091 Mbongé Muyuka PEOPLE IN NEED West Coast Buéa FAKO Tiko Limbé 2 Limbé 1 221,642 Limbé 3 [ Kilometers PEOPLE TARGETED 0 15 30 *Note : Sources: HNO 2021 PiN includes IDP, Returnees and Host Communi�es The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations Key Achievement Indicators PoC Reached - AGD Breakdouwn 296 # of Households assisted with Children 27% 26% emergency shelter 1,480 Adults 21% 22% # of households assisted with core 3,769 Elderly 2% 2% relief items including prevention of COVID-19 21,618 female male 41 # of households assisted with cash for rental subsidies 41 Households Reached Individuals Reached Cartegories of beneficiaries reported People Reached by region Distribution of Shelter NFI kits integrated with COVID 19 KITS in Matoh town. -

Dictionnaire Des Villages Du Mbam P
OFFICE DE LA RECHERCHE REPUBliQUE FEDERALE SCIENTIFIQUE ET TECHNIQUE DU OUT,RE·MER CAMEROUN CENTRE OR5TOM DE YAOUNDE DICTIONNAIRE DES _VILLAGES DU MBAM D'après la documentation réunie par ~la Section de Géographie de l'I.R.CAM.3 REPERTQIRE GEOGRAPHIQUE DU CAMEROUN FASCICULE n° 1 1 rR-GAM 8. P. '9J SH. n° 31 YAOUNDÉ Mai 1966 REPERTOIRE GEOGRAPHIQUE DU CAMEROUN Fasc. Tableau de la population du Cameroun, 68 p. Fév. 1965 SH, N° 17 Fasc. 2 Dictionnaire des villages du Dia et Lobo, 89 p. Juin 1965 SH. N° 22 Fasc. 3 Dictionnaire des villages de la Haute-Sanaga, 53 p. Août 1965 SH. N° 23 Fasc. 4 Dictionnaire des villages du Nyong et Mfoumou, 49 p. Octobre 1965 SH. N° 24 Fasc. 5 Dictionnaire des villages du Nyong et Soo 45 p. Novembre 1965 SH. N° 25 Fasc. 6 Dictionnaire des villages du Ntem 126 p. Décembre 1965 SH. N° 26 Fasc. 7 Dictionnaire- des villages de la Mefou 108 p. Janvier 1966 SH. N° 27 Fasc. 8 Dictionnaire des villages du Nyong et Kellé 51 p. Février 1966 SH. N° 28 Fasc. 9 Dictionnaire des villages de la Lékié 71 p. Mars 1966 SH. N° 29 Fasc. 10 Dictionnaire des villages de Kribi P. Mars 1966 SH. N° 30 Fasc. 11 Dictionnaire des villages du Mbam P. 60 Mai 1966 SH. N° 31 Fasc. 12 Dictionnaire des villages de Boumba Ngoko (en préparation) Fasc. 13 ùictionnaire des villages de Lom-et-Diérem (en préparation! omCE DE LA RECHERCHE SCIENTIFIQUE RERJBLlQUE FEDERALE ET TECHNI~E OUmE-MER ID CAMEROUN _ • _cee- -- - CENTRE ORSTOM DE YAOUNDE DICTIONNAIRE ~ VILLAGES DU ...........M B A M MAI 1!66 S.R. -

Ouest Uest E
quête d’assurance quête en transfrontaliers clients Les le Maire et son adjoint et son le Maire Kwemo Pierre fait enfermer ErnestOuandié honorent Patient etNdom Walla Kah Basile, Louka Adamou, Koupit Ouest Echos N° 1171 du 20 du 1171 N° Echos Ouest AFRILAND QUITTE GUINÉE LA EQUATO, LES PRODUCTEURS DE L’OUEST INQUIETS... Récipissé N°341 / RDDJ / C19 / BAPP DEVOIR DE MÉMOIRE : MÉMOIRE DE DEVOIR Since 1994 (vingt troisième année) O O COMMUNE DEBANWA COMMUNE PremierJournal national d’informations Régionales uest uest au 26 Janvier 2021 2021 Janvier 26 au l’arbitrage du Premier Ministre choix dusite et demandent Les populations s’opposent au première chaire Pierre Castel du pays L’Université deDschang hôte de la PARTENARIAT PRIVÉAU CAMEROUN PUBLIC PARTENARIAT CONSTRUCTION DU PEAGE AUTOMATIQUE DEBANDJA AUTOMATIQUE PEAGE DU CONSTRUCTION Tomaïno Ndam Njoya à Foumban à Njoya Ndam Tomaïno Awa se Fonka brûle au contact de E E INSTALLATION DU PRÉFET DU PRÉFET DU NOUN INSTALLATION Michel Eclador PEKOUA Eclador Michel publication de Directeur Les Monts d’Or 2020 2020 d’Or Monts Les Prix : 400 F. CFA F. 400 : Prix LA RÉGION DEL’OUEST RÉGION LA CÉLÈBRE SES AWARDS SES CÉLÈBRE c’est bientôt !!! bientôt c’est Actualités INSTALLATION DU NOUVEAU PRÉFET DU NOUN : Le gouverneur Awa Fonka perd sa sérénité à Foumban La scène a médusé les milliers de populations venus accueillir à la place des fêtes de Foumban, le nouveau préfet du département du Noun, Um Donacien, nommé le 18 décembre 2020 en remplacement de monsieur Boyomo Donatien, muté. l'occasion de la cérémonie de gramme de la plus leur temps à afficher leur mul- Njoya. -
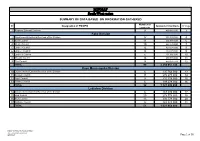
MINMAP South-West Region
MINMAP South-West region SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of N° Designation of PO/DPO Amount of Contracts N° Page contracts 1 Regional External Services 9 490 982 000 3 Fako Division 2 Départemental External Services of the Division 17 352 391 000 4 3 Buea Council 11 204 778 000 6 4 Idenau Council 10 224 778 000 7 5 Limbe I Council 12 303 778 000 8 6 Limbe II Council 13 299 279 000 9 7 Limbe III Council 6 151 900 000 10 8 Muyuka Council 16 250 778 000 11 9 Tiko Council 14 450 375 748 12 TOTAL 99 2 238 057 748 Kupe Muanenguba Division 10 Départemental External Services of the Division 6 135 764 000 13 11 Bangem Council 11 572 278 000 14 12 Nguti Council 9 215 278 000 15 13 Tombel Council 6 198 278 000 16 TOTAL 32 1 121 598 000 Lebialem Division 14 Départemental External Services of the Division 6 167 474 000 17 15 Alou Council 20 278 778 000 18 16 Menji Council 13 306 778 000 20 17 Wabane Council 12 268 928 000 21 TOTAL 51 1 021 958 000 PUBLIC CONTRACTS PROGRAMMING AND MONITORING DIVISION /MINMAP Page 1 of 36 MINMAP South-West region SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of N° Designation of PO/DPO Amount of Contracts N° Page contracts Manyu Division 18 Départemental External Services of the Division 9 240 324 000 22 19 Akwaya Council 10 260 278 000 23 20 Eyumojock Council 6 195 778 000 24 21 Mamfe Council 7 271 103 000 24 22 Tinto Council 7 219 778 000 25 TOTAL 39 1 187 261 000 Meme Division 23 Départemental External Services of the Division 4 82 000 000 26 24 Konye Council 5 171 533 000 26 25 Kumba -

Assessing Cost Efficiency Among Small Scale Rice Producers in the West Region of Cameroon: a Stochastic Frontier Model Approach
International Journal of Humanities Social Sciences and Education (IJHSSE) Volume 3, Issue 6, June 2016, PP 1-7 ISSN 2349-0373 (Print) & ISSN 2349-0381 (Online) http://dx.doi.org/10.20431/2349-0381.0306001 www.arcjournals.org Assessing Cost Efficiency among Small Scale Rice Producers in the West Region of Cameroon: A Stochastic Frontier Model Approach Djomo, Raoul Fani*1, Ewung, Bethel1, Egbeadumah, Maryanne Odufa2 1Department of Agricultural Economics. University of Agriculture, Makurdi. Benue-State, Nigeria PMB 2373, Makurdi 2Department of Agricultural Economics and Extension, Federal University Wukari, PMB 1020 Wukari. Taraba State, Nigeria *[email protected] Abstract: Local farmers’ techniques and knowledge in rice cultivation being deficient and the aid system and research to support such farmers’ activities likewise insufficient, technological progress and increase in rice production are not yet assured. Therefore, this Study was undertaken to assess cost efficiency among small scale rice farmers in the West Region of Cameroon using stochastic frontier model approach. A purposive, multistage and stratified random sampling technique was used in selecting the respondents. A total of 192 small scale rice farmers were purposively selected from four (4) out of eight divisions. Data were collected using structured questionnaires and interview schedule, administered on the respondents were analyzed using descriptive statistics and stochastic frontier cost functions. The result indicates that the coefficient of cost of labour was found positive and significantly influence cost of production in small scale rice production at 1 percent level of probability, implying that increases in cost of labour by one unit will also increase cost of production in small scale rice farming by the value of it coefficient. -

Evaluating the Constraints and Opportunities of Maize Production in the West Region of Cameroon for Sustainable Development
Journal of Sustainable Development in Africa (Volume 13, No.4, 2011) ISSN: 1520-5509 Clarion University of Pennsylvania, Clarion, Pennsylvania EVALUATING THE CONSTRAINTS AND OPPORTUNITIES OF MAIZE PRODUCTION IN THE WEST REGION OF CAMEROON FOR SUSTAINABLE DEVELOPMENT Godwin Anjeinu Abu1, Raoul Fani Djomo-Choumbou1 and Stephen Adogwu Okpachu2 1. Department of Agricultural Economics, University of Agriculture PMB 2373, Makurdi Benue State- Nigeria 2. Federal College of Education (Technical), Potiskum, Yobe State, Nigeria ABSTRACT A study of Evaluating the constraints and opportunities of Maize production in the West Region of Cameroon was carried out using primary and secondary data collected. One hundred and twenty (120) maize farmers randomly selected from eight (8) villages were interviewed using structured questionnaire. Data from the study were analyzed using descriptive statistics such as frequency distribution, percentages, and inferential statistics such as multiple linear regressions. The study found that most maize farmers in the study area were small scale farmers and are full time farmers, the major maize production constraints was poor access to credit facilities. it was also found any unit increase in the quantity of any of the resources used for maize production will increase maize output by the value of their estimated coefficients respectively , however to raise maize production, the study recommend that financial institutions such as agricultural and community banks should be established in the study area with the simple procedure of securing loans. The relevant government agencies and non- governmental organization should mobilize the maize farmers to form themselves into formidable group so that they can derive maximum benefit of collective union. -

Masks on the Move Defying Genres, Styles, and Traditions in the Cameroonian Grassfields
Masks on the Move Defying Genres, Styles, and Traditions in the Cameroonian Grassfields Silvia Forni n the realm of African art, masks are some of the most This article investigates the longstanding history of commer- exemplary and iconic artworks. Whether displayed cial practices and stylistic experimentation that characterize to be admired for their shape, form, and volumes, or the production of masks and other artworks in the Grassfields presented in dialogue with ethnographic information of Western Cameroon. While I acknowledge the importance of and contextual images, masks are omnipresent in col- long-distance and international trade as an important stimulus lections and displays of African art. As aesthetic and for creativity and artistic production, my intention is to high- ethnographic objects, masks are used as gateways to the under- light the significance of contemporary artistic inventions in Istanding and appreciation of “cultural styles” as well as the for- shaping local understanding of aesthetics and material displays. mal and creative solutions adopted by artists and workshops. Yet Collections, museums, eco-museological itineraries and, more the appeal of masks also relies on their perceived irreducible dif- recently, experimentations and artistic interventions by contem- ference and mysterious spiritual aura. Even when isolated and porary artists Hervé Youmbi and Hervé Yamguen (Fig. 1) have stripped of their fiber costumes and attachments, there is always produced a complex and intriguing regional and national artistic a reference to the body of an absent wearer, thus evoking a sit- scene. Here the taxonomies distinguishing commercial produc- uated and embodied history of production, performance, and tions from “authentic artworks” have been blurred and subverted social meaning that often does not accompany the mask into the in local practices, where masks are now moving between spheres museum. -

Programmation De La Passation Et De L'exécution Des Marchés Publics
PROGRAMMATION DE LA PASSATION ET DE L’EXÉCUTION DES MARCHÉS PUBLICS EXERCICE 2021 JOURNAUX DE PROGRAMMATION DES MARCHÉS DES SERVICES DÉCONCENTRÉS ET DES COLLECTIVITÉS TERRITORIALES DÉCENTRALISÉES RÉGION DU CENTRE EXERCICE 2021 SYNTHESE DES DONNEES SUR LA BASE DES INFORMATIONS RECUEILLIES N° Désignation des MO/MOD Nbre de Marchés Montant des Marchés N°Page 1 Services déconcentrés Régionaux 17 736 645 000 3 2 Communauté Urbaine de Yaoundé 62 10 459 000 000 5 Département de la Haute Sanaga 3 Services déconcentrés départementaux 2 24 000 000 10 4 Commune de Bibey 12 389 810 000 10 5 Commune de Lembe Yezoum 17 397 610 000 11 6 Commune de Mbandjock 12 214 000 000 12 7 Commune de Minta 8 184 500 000 12 8 Commune de Nanga Ebogo 21 372 860 000 13 9 Commune de Nkoteng 12 281 550 000 14 10 Commune de Nsem 5 158 050 000 15 TOTAL 89 2 022 380 000 Département de la Lekié 11 Services déconcentrés départementaux 9 427 000 000 16 12 Commune de Batchenga 8 194 000 000 17 13 Commune d'Ebebda 10 218 150 000 18 14 Commune d'Elig-Mfomo 8 174 000 000 19 15 Commune d'Evodoula 10 242 531 952 20 16 Commune de Lobo 11 512 809 000 21 17 Commune de Monatélé 12 288 500 000 22 18 commune d'Obala 11 147 000 000 23 19 commune d'Okola 14 363 657 000 24 20 commune de Sa'a 17 319 500 000 25 TOTAL 110 2 887 147 952 Département du Mbam et Inoubou 21 Services déconcentrés départementaux 6 144 385 000 27 22 Commune Bafia 13 213 500 000 27 23 Commune de Bokito 9 167 500 000 28 24 Commune de DEUK 17 379 500 000 29 25 Commune Kiiki 10 285 000 000 30 26 Commune Konyambeta 12 295 -

Cameroon | Displacement Report, Far North Region Round 9 | 26 June – 7 July 2017 Cameroon | Displacement Report, Far North Region, Round 9 │ 26 June — 7 July 2017
Cameroon | Displacement Report, Far North Region Round 9 | 26 June – 7 July 2017 Cameroon | Displacement Report, Far North Region, Round 9 │ 26 June — 7 July 2017 The opinions expressed in the report are those of the authors and do not necessarily reflect the views of the International Organization for Migration (IOM). The designations employed and the presentation of material throughout the report do not imply the expression of any opinion whatsoever on the part of IOM concerning the legal status of any country, territory, city or area, or of its authorities, or concerning its frontiers or boundaries.1 IOM is committed to the principle that humane and orderly migration benefits migrants and society. As an intergovernmental organization, IOM acts with its partners in the international community to: assist in meeting the operational challenges of migration; advance understanding of migration issues; encourage social and economic development through migration; and uphold the human dignity and well-being of migrants. International Organization for Migration UN House Comice Maroua Far North Region Cameroon Cecilia Mann Tel.: +237 691 794 050 E-mail: [email protected] Website: www.globaldtm.info/cameroon/ © IOM 2017 All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise without the prior written permission of the publisher. 1 The maps included in this report are illustrative. The representations and the use of borders and geographic names may include errors and do not imply judgment on legal status of territories nor acknowledgement of borders by the Organization. -
Assessment of Prunus Africana Bark Exploitation Methods and Sustainable Exploitation in the South West, North-West and Adamaoua Regions of Cameroon
GCP/RAF/408/EC « MOBILISATION ET RENFORCEMENT DES CAPACITES DES PETITES ET MOYENNES ENTREPRISES IMPLIQUEES DANS LES FILIERES DES PRODUITS FORESTIERS NON LIGNEUX EN AFRIQUE CENTRALE » Assessment of Prunus africana bark exploitation methods and sustainable exploitation in the South west, North-West and Adamaoua regions of Cameroon CIFOR Philip Fonju Nkeng, Verina Ingram, Abdon Awono February 2010 Avec l‟appui financier de la Commission Européenne Contents Acknowledgements .................................................................................................... i ABBREVIATIONS ...................................................................................................... ii Abstract .................................................................................................................. iii 1: INTRODUCTION ................................................................................................... 1 1.1 Background ................................................................................................. 1 1.2 Problem statement ...................................................................................... 2 1.3 Research questions .......................................................................................... 2 1.4 Objectives ....................................................................................................... 3 1.5 Importance of the study ................................................................................... 3 2: Literature Review ................................................................................................. -
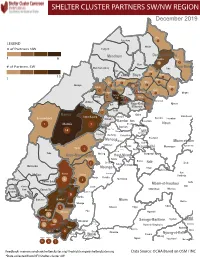
NW SW Presence Map Complete Copy
SHELTER CLUSTER PARTNERS SW/NWMap creation da tREGIONe: 06/12/2018 December 2019 Ako Furu-Awa 1 LEGEND Misaje # of Partners NW Fungom Menchum Donga-Mantung 1 6 Nkambe Nwa 3 1 Bum # of Partners SW Menchum-Valley Ndu Mayo-Banyo Wum Noni 1 Fundong Nkum 15 Boyo 1 1 Njinikom Kumbo Oku 1 Bafut 1 Belo Akwaya 1 3 1 Njikwa Bui Mbven 1 2 Mezam 2 Jakiri Mbengwi Babessi 1 Magba Bamenda Tubah 2 2 Bamenda Ndop Momo 6b 3 4 2 3 Bangourain Widikum Ngie Bamenda Bali 1 Ngo-Ketunjia Njimom Balikumbat Batibo Santa 2 Manyu Galim Upper Bayang Babadjou Malentouen Eyumodjock Wabane Koutaba Foumban Bambo7 tos Kouoptamo 1 Mamfe 7 Lebialem M ouda Noun Batcham Bafoussam Alou Fongo-Tongo 2e 14 Nkong-Ni BafouMssamif 1eir Fontem Dschang Penka-Michel Bamendjou Poumougne Foumbot MenouaFokoué Mbam-et-Kim Baham Djebem Santchou Bandja Batié Massangam Ngambé-Tikar Nguti Koung-Khi 1 Banka Bangou Kekem Toko Kupe-Manenguba Melong Haut-Nkam Bangangté Bafang Bana Bangem Banwa Bazou Baré-Bakem Ndé 1 Bakou Deuk Mundemba Nord-Makombé Moungo Tonga Makénéné Konye Nkongsamba 1er Kon Ndian Tombel Yambetta Manjo Nlonako Isangele 5 1 Nkondjock Dikome Balue Bafia Kumba Mbam-et-Inoubou Kombo Loum Kiiki Kombo Itindi Ekondo Titi Ndikiniméki Nitoukou Abedimo Meme Njombé-Penja 9 Mombo Idabato Bamusso Kumba 1 Nkam Bokito Kumba Mbanga 1 Yabassi Yingui Ndom Mbonge Muyuka Fiko Ngambé 6 Nyanon Lekié West-Coast Sanaga-Maritime Monatélé 5 Fako Dibombari Douala 55 Buea 5e Massock-Songloulou Evodoula Tiko Nguibassal Limbe1 Douala 4e Edéa 2e Okola Limbe 2 6 Douala Dibamba Limbe 3 Douala 6e Wou3rei Pouma Nyong-et-Kellé Douala 6e Dibang Limbe 1 Limbe 2 Limbe 3 Dizangué Ngwei Ngog-Mapubi Matomb Lobo 13 54 1 Feedback: [email protected]/ [email protected] Data Source: OCHA Based on OSM / INC *Data collected from NFI/Shelter cluster 4W.