(Public Pack)Agenda Document for Families and Wellbeing Policy And
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pharmacy Name
Think Pharmacy Scheme Pharmacies - December 2019 Pharmacy Name Asda Pharmacy – Birkenhead – 222 Grange Rd, Birkenhead CH41 6EB Asda Pharmacy – Liscard – Seaview Road, Wallasey CH45 4NZ Asda Pharmacy – Upton – Woodchurch Road, Upton, CH49 5PD Asda Pharmacy – Bromborough – Welton Road, Croft Business Park, CH62 3QP Birkenhead Pharmacy – 31 Laird Street, Birkenhead CH41 8DB Blackheath Pharmacy – 113 Reeds Lane, Leasowe, CH46 1QT Boots – Birkenhead – 215 Grange Road, Birkenhead, Merseyside, CH41 2PH Boots – Bromborough Retail Park – Welton Road, Croft Retail Park, Bromborough, CH62 3PN Boots – Manor Health Centre – Manor Health Centre, Liscard Village,Wallasey, CH45 4JG Boots – Higher Bebington – 118 Teehey Lane, Bebington, Wirral CH63 8QT Boots – West Kirby – 11-13 The Crescent, West Kirby, CH48 4HL Boots – Rock Ferry – 206 Bedford Road, Birkenhead CH42 2AT Boots – Noctorum Upton Road – 395 Upton Road, Birkenhead CH43 9SE Boots – Bromborough The Precinct – 3-5 The Rake Precinct, Bromborough, CH62 7AD Boots – Moreton – 254 Hoylake Road, Moreton, CH46 6AF Boots – Greasby – 148 Greasby Road, Greasby, CH49 3NQ Boots – Upton – 23 Arrowe Park Road, Wirral, CH49 0UB Boots – Bidston – 30 Hoylake Road, Birkenhead CH41 7BX Boots – Arrowe Park – 156 Common Field Rd, Woodchurch, Wirral CH49 7LP Boots – Thingwall – 509 Pensby Road, Wirral, CH61 7UQ Boots – Prenton Woodchurch Road – 379 Woodchurch Rd, Birkenhead CH42 8PE Boots – Heswall – 218-220, Telegraph Road, Heswall, CH60 0AL Boots – Prenton Holmlands Drive – 8-10 Holmlands Dr, Birkenhead CH43 0TX -

Meet the Estates Team 04
FREE C Please take me home Winter/Spring 2014 3 EX PATIENT KATIE BIRCHALL OPENS NEW CHILDREN’S WAITING AREA Read her story inside NEW STAFF ACHIEVEMENT Meet the AWARDS/WINNERS Estates Team New pharmacy Papillon Suite launch Help to give up smoking Charity News THIS ISSUE Welcome Contents 02 Welcome 04 Ex patient Katie Birchall’s story 06 New on-site pharmacy brings patient benefits 07 Maggie’s to open its first Merseyside centre 08 Charity News 09 Update on plans for the new Clatterbridge I would like to wish all our staff, patients and their families, members and supporters a Happy New Year. 2013 was an exciting and busy year for The Clatterbridge Cancer Centre. Cancer Centre in Liverpool This issue will bring you up-to-date with what’s been happening since the last issue and as you will see the year ended on a high with some fantastic new developments. 10 Meet the Estates Team 04 12 Trust is recognised for outstanding care 3 C’s: Centre, Clinic, Charity. 13 New addition to our first class team of cancer experts The Centre welcomed a number of new senior appointments to further strengthen the clinical expertise and eight new oncologists and 20 new radiographers have been added to our team of 14 Help to stop smoking specialists to ensure we always improve our care. You can read all about this on page 13. 15 Meet Ian Boycott-Samuels - Foundation It was great to see one of our ex patients, Katie Birchall, back at the Centre to open a new children’s play area in the radiotherapy department. -

Viking Wirral … and the Battle of Brunanburh Professor Steve Harding
Viking Wirral … and the Battle of Brunanburh Professor Steve Harding Neil Oliver, “History of Scotland” BBC2, 2009 “ The many armies, tens of thousands of warriors clashed at the site known as Brunanburh where the Mersey Estuary enters the sea . For decades afterwards it was simply known called the Great Battle. This was the mother of all dark-age bloodbaths and would define the shape of Britain into the modern era. Althouggg,h Athelstan emerged victorious, the resistance of the northern alliance had put an end to his dream of conquering the whole of Britain. This had been a battle for Britain, one of the most important battles in British historyyy and yet today ypp few people have even heard of it. 937 doesn’t quite have the ring of 1066 and yet Brunanburh was about much more than blood and conquest. This was a showdown between two very different ethnic identities – a Norse-Celtic alliance versus Anglo-Saxon. It aimed to settle once and for all whether Britain would be controlled by a single Imperial power or remain several separate kingdoms. A split in perceptions which, like it or not, is still with us today”. Some of the people who’ve been trying to sort it out Nic k Hig ham Pau l Cav ill Mic hae l Woo d John McNeal Dodgson 1928-1990 Plan •Background of Brunanburh • Evidence for Wirral location for the battle • If it did happen in Wirra l, w here is a like ly site for the battle • Consequences of the Battle for Wirral – and Britain Background of Brunanburh “Cherchez la Femme!” Ann Anderson (1964) The Story of Bromborough •TheThe Viking -
Greasby, Frankby and Irby
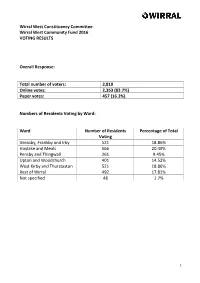
Wirral West Constituency Committee Wirral West Community Fund 2016 VOTING RESULTS Overall Response: Total number of voters: 2,810 Online votes: 2,353 (83.7%) Paper votes: 457 (16.3%) Numbers of Residents Voting by Ward: Ward Number of Residents Percentage of Total Voting Greasby, Frankby and Irby 521 18.86% Hoylake and Meols 566 20.49% Pensby and Thingwall 261 9.45% Upton and Woodchurch 401 14.52% West Kirby and Thurstaston 521 18.86% Rest of Wirral 492 17.81% Not specified 48 1.7% 1 VOTING RESULTS – GREASBY, FRANKBY AND IRBY PROJECTS 1. Support from Greasby, Frankby and Irby residents (ranked highest to lowest) Ranking Project Amount Number of Percentage of Requested Votes Greasby, Frankby and Irby Vote 1st Coronation Park Playground £1,000.00 308 59.1% Improvements (Greasby Association: Friends of Coronation Park Playground) 2nd Greasby Christmas Lights £1,000.00 255 48.9% (Greasby Community Association) 3rd Green and Blooming Greasby £750.00 238 45.7% Environmental Upkeep (Greasby Community Association) 4th Green and Blooming Greasby £900.00 219 42% New Planters (Greasby Community Association) 5th The Greasby Messenger £1,000.00 190 36.5% (Greasby Community Association) 6th Irby Library Improvements £1,000.00 179 34.4% (Friends of Irby Library) 7th Celebrate Greasby Day (Greasby £1,000.00 170 32.6% Community Association) 8th Greasby Allotments £1,000.00 157 30.1% Improvements (Greasby Allotment Holders and Gardeners Association) 9th Irby Cricket Club Improvements £600.00 153 29.4% 2 VOTING RESULTS – GREASBY, FRANKBY AND IRBY PROJECTS -

Matalan Bromborough
BROMBOROUGH VILLAGE ROAD BROMBOROUGH CHESHIRE CH62 7ES RETAIL WAREHOUSE INVESTMENT OPPORTUNITY ENTER RETAIL WAREHOUSE INVESTMENT OPPORTUNITY BROMBOROUGH Investment Location & Situation & Retail Description Tenancy, Tenure & Covenant, EPC Proposal & Highlights Catchment Warehousing in Planning & VAT Contacts Population Bromborough Offers are sought in excess of • Bromborough is strategically located on the Wirral Peninsular, between Liverpool and Chester. INVESTMENT £5,640,000 (Five Million, Six • Excellent visibility from the busy A41 New Chester Road, close to The Croft Retail & Leisure Park, Hundred and Forty Thousand which attracts 7 million visitors annually. HIGHLIGHTS Pounds), subject to contract • Standalone unit of 29,497 sq ft let to the 5A1 D&B rated covenant of Matalan Retail Ltd. and exclusive of VAT. This • £450,851 per annum rent (£15.05 per sq ft). equates to an attractive net • In excess of 8 years unexpired. initial yield of 7.50%, based on • Open A1 non-food planning consent. purchaser’s costs of 6.61%. RETAIL WAREHOUSE INVESTMENT OPPORTUNITY BROMBOROUGH Investment Location & Situation & Retail Description Tenancy, Tenure & Covenant, EPC Proposal & Highlights Catchment Warehousing in Planning & VAT Contacts Population Bromborough 6 5 4 ST HELENS M57 LOCATION & CATCHMENT POPULATION BOOTLE 3 WALLASEY Bromborough is one of the principal retail centres of the Wirral, being located 2 PRESCOT on the Wirral Peninsular in the North West of England. The town is 6 miles 1 LIVERPOOL HUYTON M62 8 south of Liverpool city centre across the Mersey and 13 miles north of Chester. 5 M62 7 Birkenhead is 2 miles north. HOYLAKE 2 BIRKENHEAD 6/1 M53 As a result of its strategic location, Bromborough benefits from excellent WEST KIRBY 3 communication links. -

H1 Bus Time Schedule & Line Route
H1 bus time schedule & line map H1 Greasby - Newton (mersyd) View In Website Mode The H1 bus line (Greasby - Newton (mersyd)) has 2 routes. For regular weekdays, their operation hours are: (1) Grange: 8:15 AM (2) Greasby: 3:18 PM Use the Moovit App to ƒnd the closest H1 bus station near you and ƒnd out when is the next H1 bus arriving. Direction: Grange H1 bus Time Schedule 8 stops Grange Route Timetable: VIEW LINE SCHEDULE Sunday Not Operational Monday 8:15 AM Eastcott Close, Greasby Eastcott Close, Birkenhead Tuesday 8:15 AM Millcroft Park, Greasby Wednesday 8:15 AM Millcroft Park, England Thursday 8:15 AM Frankby Green, Frankby Friday 8:15 AM The Nook, England Saturday Not Operational Frankby Stiles, Frankby Newton Park Road, Newton Newton Cross Lane, Newton H1 bus Info Direction: Grange Woodland Road, Larton Stops: 8 Trip Duration: 10 min Wirral Mount, Grange Line Summary: Eastcott Close, Greasby, Millcroft Park, Greasby, Frankby Green, Frankby, Frankby Stiles, Frankby, Newton Park Road, Newton, Newton Cross Lane, Newton, Woodland Road, Larton, Wirral Mount, Grange Direction: Greasby H1 bus Time Schedule 8 stops Greasby Route Timetable: VIEW LINE SCHEDULE Sunday Not Operational Monday 3:18 PM Hilbre High School, Newton Tuesday 3:18 PM Fulton Avenue, Grange Wednesday 3:18 PM China Farm Lane, Larton Thursday 3:18 PM Frankby Stiles, Frankby Friday 3:18 PM Frankby Green, Frankby Saturday Not Operational St Johns Church, Frankby Frankby Close, Greasby H1 bus Info Millcroft Park, England Direction: Greasby Hillcrest Drive, Greasby Stops: 8 Trip Duration: 10 min Line Summary: Hilbre High School, Newton, Fulton Avenue, Grange, China Farm Lane, Larton, Frankby Stiles, Frankby, Frankby Green, Frankby, St Johns Church, Frankby, Frankby Close, Greasby, Hillcrest Drive, Greasby H1 bus time schedules and route maps are available in an o«ine PDF at moovitapp.com. -

'Honeygreave' and the Rock House Ferry*
‘Honeygreave’ and the Rock House ferry* I In the published Bebington parish registers for the years 1558 to 1701 there occurs, 44 times between 1585 and 1692, the place- name ‘Honeygreave’, 30 in relation to christenings and 14 to burials (see appendix).1 The name, which does not recur after 1701 in the unpublished registers, was one of only three - apart from those of familiar villages or hamlets — used to denote the dwellings of individual parishioners. Its meaning is ‘Honey Grove’ or ‘Honey Wood’, and the allusion is apparently to honeysuckle, as in the Landican fieldname ‘Honey Field’.2 This pleasingly bucolic toponym is unremarkable in all respects but one: it is not found anywhere else. No trace of Honeygreave features in the recent and exhaustive survey The place-names o f Cheshire,3 even in the sizeable appendix of rare, unidentified or failed names. But although the record of its existence is confined to the Bebington registers, its occurrence there was nevertheless frequent enough, and its demise recent enough, to call for explanation. What and where was it, and why did it fail? The enigmatic ‘Honeysuckle Wood’ deserves attention; certainly more than it was given in the published registers, where no editorial explanation or comment is offered and where it is not even included in the index — hence its absence from Place-names. * The writer wishes to thank Mr D. N. Thompson of the Wirral Archives Service, Birkenhead Central Library, the staff of the Chester and Cheshire Record Office, Chester, and Dr Sean Cunningham of the National Archives for their advice and assistance. -

Transforming Cancer Care
TRANSFORMING CANCER CARE AN OPPORTUNITY TO SIGNIFICANTLY IMPROVE THE DELIVERY OF CANCER SERVICES ACROSS THE MERSEYSIDE AND CHESHIRE CANCER NETWORK May 2014 AN OPPORTUNITY TO SIGNIFICANTLY IMPROVE THE DELIVERY OF CANCER SERVICES ACROSS THE MERSEYSIDE AND CHESHIRE CANCER NETWORK Contents Section Page No. 1. Introduction 3 2. The Catchment Population served by The Clatterbridge Cancer 4 Centre 3. Cancer incidence & mortality across the Merseyside & Cheshire 5 Cancer Network (MCCN) 4. Current configuration of cancer services provided by CCC across 9 the MCCN 5. Proposals to transform cancer services in Merseyside & Cheshire – 10 The Case for Change 6. The current Strategic Environment 12 7. Outcome of the Pre-Consultation Engagement Work undertaken 14 over the Winter of 2012 / 13 8. The proposed changes in cancer services as a consequence of the 16 Transforming Cancer Care Project 9. Benefits which would be delivered by the Proposed Changes 19 10. Impact on patients as a consequence of their place of treatment 21 11. Timescales 26 12. Stakeholders involvement 26 13. Summary 26 2 AN OPPORTUNITY TO SIGNIFICANTLY IMPROVE THE DELIVERY OF CANCER SERVICES ACROSS THE MERSEYSIDE AND CHESHIRE CANCER NETWORK 1. INTRODUCTION The Clatterbridge Cancer Centre NHS Foundation Trust (CCC) is a highly regarded specialist cancer Trust providing non-surgical treatment for patients suffering from solid tumour cancers within the Merseyside and Cheshire Cancer Network (MCCN). This document has been produced by CCC, supported by Cheshire, Warrington and Wirral Area Team, its commissioner of services. The document describes the background to the Transforming Cancer Care project, the proposals for change and expansion of the CCC services, and both the clinical rationale for these changes and the benefits which will result from them. -

Hoylake Station Interchange Information
Hoylake Station Interchange Information Buses from Stop A A Buses from Stop B B Rail replacement services towards Rail replacement services towards Birkenhead North operate from this West Kirby operate from this stop. stop. From 28/03/2011 From 28/03/2011 To: NEW FERRY 38 To: WEST KIRBY Via: Birkenhead Road, Hoylake Road, Moreton Cross, 38 Hoylake Road, Fender Lane, Tollemache Road, Park Road West, Birkenhead Bus Station, Derby Road, Greenway Road, MONDAY TO FRIDAY SATURDAY SUNDAY Bebington Road, Old Chester Road 6.40am 7.10am 7.44am MONDAY TO FRIDAY SATURDAY SUNDAY 8.14am 8.53am 9.19am 9.54am 6.58am 7.54am THEN EVERY 30 MINUTES 7.22am 7.57am THEN EVERY 30 MINUTES 8.29am AT NO 24 54 AT 9.08am 9.38am 8.08am 8.38am MINUTES PAST EACH HOUR 24 54 SERVICE MINUTES PAST EACH HOUR THEN EVERY 30 MINUTES THEN EVERY 30 MINUTES UNTIL 3.24pm 3.54pm NO UNTIL 6.24pm 4.27pm 4.59pm AT 08 38 AT 08 38 SERVICE 5.35pm MINUTES PAST EACH HOUR MINUTES PAST EACH HOUR 6.09pm 6.40pm UNTIL 3.08pm 3.38pm UNTIL 6.08pm 6.38pm 7.10pm 4.08pm 4.42pm 5.12pm 5.48pm 6.21pm 6.52pm From 27/01/2013 39 To: WEST KIRKBY STATION To: NEW BRIGHTON From 27/01/2013 X39 Via: Meols Drive 39 Via: Birkenhead Road, Millhouse Lane, Town Meadow Lane, Pasture Road, Hoylake Road, Reeds Lane, Leasowe Road, X39 Breck Road, Wallasey Road, Seaview Road, MONDAY TO FRIDAY SATURDAY SUNDAY Mount Pleasant Road, Magazine Lane, Rowson Street 7.42am I 7.42am 8.02am 8.25am 10.38am MONDAY TO FRIDAY SATURDAY SUNDAY 8.02am 8.31am 9.01am 9.31am THEN EVERY 30 MINUTES 7.52am THEN EVERY 30 MINUTES 8.20am 8.49am -

The London Gazette, 24Th August 1989 9865 Notices Under the Trustee Act
THE LONDON GAZETTE, 24TH AUGUST 1989 9865 NOTICES UNDER THE TRUSTEE ACT Notice is hereby given pursuant to section 27 of the Trustee Act 1925 such particulars before the date specified in relation to that deceased that any person having a claim against or an interest in the estate person in the fourth column of the said table, after which date the of any of the deceased persons whose names and addresses are set out personal representatives will distribute the estate among the persons in the first and second columns of the following table is hereby required entitled thereto having regard only to the claims and interests of which to send particulars in writing of his claim or interest to the person or they have had notice and will not, as respects the property so persons whose names and addresses are set out opposite the name of distributed, be liable to any person of whose claim they shall not then the deceased person in the third column of the table, and to send have had notice. Names, addresses and descriptions of Date before which Name of Deceased Address, description and date of death Persons to whom notices of claims are (Surname first) of Deceased to be given and names, in parentheses, notices of claims to be given of Personal Representatives NICHOLAS, Yvonne Flat 39, Hovedene, 95 Cromwell Road, National Westminster Bank Pic, Trust 25th October 1989 (496) Josephine Hove, East Sussex, Widow. and Tax, Financial and Investment 5th August 1989. Service, Worthing Trustee and Investment Branch, 6s Littlehampton Road, Worthing, West Sussex BN13 1PT. -

Pick-Me-Up, Your Handy Guide
Your local, independent charity Registered charity number 1034510 2 Our services I’m Jamie Anderson, Chief Executive of Age UK Wirral. I hope you find this Guide a handy and easy introduction to our services available throughout Wirral. Below I have set out the services we provide and on Page 6 under How to Use This Guide it tells you how you can access them where you live. Our services include: Health & Activity If you’re looking to get in shape, pick up a new pastime or Jamie Anderson simply get out of the house to meet new people then our CEO Health and Activity programme has something for you. With our range of activities you can exercise both mind & body. Opportunities include tai chi, seated exercise classes, yoga groups, arts and crafts, flower arranging, pilates and zumba gold and much more including a range of computer & technology courses for the beginner and all levels of ability; these embrace laptops, desktops, tablets, ipads and mobile phones. There are ‘One to One’ sessions were you can learn at your own pace too; it will take you on a journey of education, enlightenment, plus the fun and joys of digital technology We are based in our Activity Hub at Meadowcroft, Bromborough and also offer a range of outreach services and activities at various community centres and housing complexes across Wirral. Lunch & Coffee Corners These are held at multiple venues throughout the Wirral. You will have the opportunity to join other people in your area for an enjoyable meal or cup of coffee in lovely, friendly surroundings, with a varied selection of menu Pick-me-up Handy Guide 3 Home & Communities Service Sometimes we do not always have the friends, family or help around us that we need to stay safe and independent in our home. -

(Public Pack)Agenda Document for Planning Committee, 26/11/2015 18:00
Planning Committee Date: Thursday, 26 November 2015 Time: 6.00 pm Venue: Committee Room 1 - Wallasey Town Hall Contact Officer: Vicky Rainsford Tel: 0151 691 8271 e-mail: [email protected] Website: http://www.wirral.gov.uk 1. MINUTES (Pages 1 - 16) To approve the accuracy of the minutes of the meeting held on 21 October 15. 2. MEMBERS' CODE OF CONDUCT - DECLARATIONS OF INTEREST Members of the committee are asked whether they have any personal or prejudicial interests in connection with any application on the agenda and, if so, to declare them and state the nature of the interest. 3. REQUESTS FOR SITE VISITS Members are asked to request all site visits before any application is considered. 4. APP/15/00398: 11 SEABANK ROAD, EGREMONT, CH44 0EE - CHANGE OF USE TO HOUSE IN MULTIPLE OCCUPANCY - 6 BEDROOM PROPERTY INCREASING TO 7 BEDROOMS WITH INTERNAL ALTERATIONS (Pages 17 - 22) 5. OUT/15/00977: GRAZING LAND, LEASOWE ROAD, WALLASEY VILLAGE - OUTLINE APPLICATION FOR 10 DWELLINGS (Pages 23 - 32) 6. APP/15/00979: LAND NORTH WEST TO 1 THE KNAP, GAYTON, CH60 0EX - PROPOSED NEW 2 BED DORMER PROPERTY ON LAND AT 1 THE KNAP (Pages 33 - 40) 7. APP/15/00983: CHESTNUT HOUSE, KINGS DRIVE, CALDY, CH48 2JF - RE-DESIGN OF EXISTING DWELLING WITH PROPOSED EXTENSIONS TO INCLUDE A NEW SWIMMING POOL, GYMNASIUM, HABITABLE SPACES. PROPOSED EXTERNAL WORKS AND RE-MODEL OF THE ELEVATIONS AND NEW EXTERNAL DETACHED DOUBLE GARAGE AND LANDSCAPING WORKS. (Pages 41 - 50) 8. APP/15/01040: CLEARED SITE GRASSED ADJACENT 54, OLD BIDSTON ROAD, BIRKENHEAD, CH41 8BL - ERECTION OF THREE DWELLINGS (Pages 51 - 56) 9.