Kansas Eyecon 2018 Program Book
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ocular Injury; Hazard to Society: a Case Series
Quest Journals Journal of Medical and Dental Science Research Volume 7~ Issue 8 (2020) pp: 34-44 ISSN(Online) : 2394-076X ISSN (Print):2394-0751 www.questjournals.org Research Paper Ocular Injury; Hazard to Society: A Case Series Dr Rashmi kujur1, Dr Pallavi. M.P2, Dr Harshita Dubey3, Dr Varsha4 1Dept. of ophthalmology, Madhav dispensary JAH, GRMC, Gwalior, Madhyapradesh. 2Senior girls hostel, GRMC, Gwalior, Madhyapradesh. 3Senior girls hostel, GRMC, Gwalior, Madhyapradesh. 4Senior girls hostel, GRMC, Gwalior,Madhyapradesh. Corresponding Author: Dr.Pallavi.M.P ABSTRACT Purpose: To describe various types of ocular trauma due to different modes of injuryoccured on the same day Design: Prospective interventional study (case series) Materials & Methods: A series of cases of ocular trauma in different age group on the same day. Results: Five patients of ocular trauma were studied & managed. All five patients were males. Out of 5 cases, 3 cases had open globe injury and 2 cases had closed globe injury. Three out of five patients required surgical intervention while 2 patients were managed with medical therapy. Conclusion: This study describes the types and characteristics of ocular trauma presenting in eye department. The frequency of ocular trauma is common in males. Eye injuries resulting from ocular trauma pose a frequent threat to vision the world over. While afocussed history and prompt ocular examination are essential to immediate management, patient educationregarding safety precautions and risk reduction help to prevent future recurrences. KEYWORDS: Ocular morbidity, Ocular Injury, globe rupture, iridodialysis, fire cracker injury, hyphema, Road Traffic accident (RTA), loss of vision. Received 05 December, 2020; Accepted 20 December, 2020 © The author(s) 2020. -

Traumatic Retinal Detachment Br J Ophthalmol: First Published As 10.1136/Bjo.75.1.18 on 1 January 1991
18 BritishJournalofOphthalmology, 1991,75, 18-21 Traumatic retinal detachment Br J Ophthalmol: first published as 10.1136/bjo.75.1.18 on 1 January 1991. Downloaded from P B Johnston Abstract trauma is a well recognised cause of rhegmato- Seventy-seven patients developed retinal genous retinal detachment, which was reported breaks following an episode of ocular con- by Eagling' to affect 4-6% of such injuries. The tusion, and 65 (84.4%) of these developed characteristics of postcontusion retinal detach- rhegmatogenous retinal detachment. Surgical ments were described by Cox et all and the treatment successfully restored or maintained mechanism ofbreak formation was elucidated by retinal apposition in 74 (96-1%) of the eyes. Delori et all who studied the effect of high speed Thirty-six (46-8%) eyes recovered visual acuity projectiles on enucleated pig eyes. Experimental of6/9orbetter. Ofthe retinal breaks recognised evidence indicates that retinal breaks form at the dialysis at the ora serrata was observed in 49 time of ocular impact. However, clinical reports eyes, of which 28 were situated at the lower show considerable delay in the diagnosis of temporal quadrant. Seventeen eyes had post-traumatic retinal detachment. For example, irregular breaks arising within necrotic retina Cox et all reported that only 30% of post- at the site of scleral impact. Twenty-four traumatic retinal detachments were diagnosed (31.2%) patients had retinal break or retinal within one month of injury, and Ross4 found detachment diagnosed within 24 hours ofinjury 40% in a similar period. and 49 (63-6%) within six weeks. Immediate The following study is of a series of patients retinal detachment was a feature of necrotic who developed retinal breaks or retinal detach- retinal breaks, while inferior oral dialyses led ment after ocular contusion. -

Full Name Phone # Gender State City
OPHTHALMOLOGISTS IN THE USA LIST OF ALL OPHTHALMOLOGY DOCTORS IN THE USA (Illinois OPHTHALMOLOGISTS are Highlighted in Yellow) FULL NAME PHONE # GENDER STATE CITY Robert Wendell Arnold 907-276-1617 Male AK Anchorage David Guy Chamberlain 907-729-1470 Male AK Anchorage Eric William Coulter 907-569-1551 Male AK Anchorage Edward Eugene Crouch 907-276-1617 Male AK Anchorage Donald Walter Dippe 907-264-1405 Male AK Anchorage Clyde William Farson 907-243-7516 Male AK Anchorage Marvin John Grendahl 907-561-1917 Male AK Anchorage Robin Lynn Grendahl 907-561-1917 Female AK Anchorage Thomas John Harrison Male AK Anchorage Oliver Marc Korshin 907-276-8838 Male AK Anchorage Thomas Henry Mader 253-968-1770 Male AK Anchorage Jan Holland Nyboer 907-561-1167 Male AK Anchorage Kenneth T Richardson 907-373-0225 Male AK Anchorage Carl E Rosen 907-276-1617 Male AK Anchorage Jon Albert Shiesl 907-563-3911 Male AK Anchorage Griffith Conway Steiner 907-276-1617 Male AK Anchorage David Ernest Swanson 907-561-1530 Male AK Anchorage Robert Paul Werner 907-349-8541 Male AK Anchorage Scott Arthur Limstrom 907-276-1617 Male AK Eagle River Denise Cruz Johnson Female AK Elmendorf Afb Alfred De Ramus 907-479-0852 Male AK Fairbanks Ronald Wayne Zamber 907-456-7760 Male AK Fairbanks Garret Lee Sitenga Male AK Homer Robert Alan Breffeilh 907-586-2700 Male AK Juneau Gordon Rex Preecs 907-586-2700 Male AK Juneau Peter Ernest Cannava Male AK Soldotna Evan Wolf 907-373-0225 Male AK Wasilla Aric Jason Aldridge Male AL Alabaster Andrew Wilfred Everett Male AL Alabaster Frank -

February 20, 2015 Vol. 119 No. 8
VOL. 119 - NO. 8 BOSTON, MASSACHUSETTS, FEBRUARY 20, 2015 $.35 A COPY WATCHING WHILE THE WORLD BURNS A Winter Poem by Sal Giarratani It’s winter in Massachusetts Back when Jack Kennedy and the gentle breezes blow. was a young man, he penned At seventy miles an hour a great piece of non-fiction entitled, “While England and at thirty-five below. Sleeps” in which he warned Oh how I love Massachusetts the world that to sit back and when the snow’s up to your butt. watch evil like a helpless bystander led to World War II. You take a breath of winter While Hitler and the Nazis and your nose gets frozen shut. slaughtered millions of inno- Yes, the weather here is wonderful cent people, including six so I guess I’ll hang around. million Jews, the West sat on its hands, but eventually I could never leave Massachusetts evil has a way of growing if cuz I’m frozen to the ground. left alone. I see the very same thing — Author Unknown taking place as I write this commentary. Just over the Presidents’ Day holiday weekend, 21 Coptic Chris- when it comes to his objec- puts a target on Europe and tians were rounded up by tivity on Radical Islam who especially Rome, Italy. Our ISIS and all dressed in or- are trying to create a global president may not believe ange jumpsuits had their caliphate when Jewish pa- we are in a war, but we are heads severed on video for trons at a Paris deli are ex- thanks to the other side. -

Vertical Perspective Medical Assistance Program
Kansas Vertical Perspective Medical Assistance Program December 2006 Provider Bulletin Number 688 General Providers Emergent and Nonemergent Diagnosis Code List Attached is a list of diagnosis codes and whether the Kansas Medical Assistance Program (KMAP) considers the code to be emergent or nonemergent. Providers are responsible for validating whether a particular diagnosis code is covered by KMAP under the beneficiary’s benefit plan and that all program requirements are met. This list does not imply or guarantee payment for listed diagnosis codes. Information about the Kansas Medical Assistance Program as well as provider manuals and other publications are on the KMAP Web site at https://www.kmap-state-ks.us. If you have any questions, please contact the KMAP Customer Service Center at 1-800-933-6593 (in-state providers) or (785) 274-5990 between 7:30 a.m. and 5:30 p.m., Monday through Friday. EDS is the fiscal agent and administrator of the Kansas Medical Assistance Program for the Kansas Health Policy Authority. Page 1 of 347 Emergency Indicators as noted by KMAP: N – Never considered emergent S – Sometimes considered emergent (through supporting medical documentation) Y – Always considered emergent Diagnosis Emergency Diagnosis Code Description Code Indicator 0010 Cholera due to Vibrio Cholerae S 0011 Cholera due to Vibrio Cholerae El Tor S 0019 Unspecified Cholera S 019 Late Effects of Tuberculosis N 0020 Typhoid Fever S 0021 Paratyphoid Fever A S 0022 Paratyphoid Fever B S 0023 Paratyphoid Fever C S 024 Glanders Y 025 Melioidosis -

Simon Stevin
II THE PRINCIPAL WORKS OF SIMON STEVIN E D IT E D BY ERNST CRONE, E. J. DIJKSTERHUIS, R. J. FORBES M. G. J. MINNAERT, A. PANNEKOEK A M ST E R D A M C. V. SW ETS & Z E IT L IN G E R J m THE PRINCIPAL WORKS OF SIMON STEVIN VOLUME II MATHEMATICS E D IT E D BY D. J. STRUIK PROFESSOR AT THE MASSACHUSETTS INSTITUTE OF TECHNOLOGY, CAMBRIDGE (MASS.) A M S T E R D A M C. V. SW ETS & Z E IT L IN G E R 1958 The edition of this volume II of the principal works of SIMON STEVIN devoted to his mathematical publications, has been rendered possible through the financial aid of the Koninklijke. Nederlandse Akademie van Wetenschappen (Royal Netherlands Academy of Science) Printed by Jan de Lange, Deventer, Holland The following edition of the Principal Works of SIMON STEVIN has been brought about at the initiative of the Physics Section of the Koninklijke Nederlandse Akademie van Weten schappen (Royal Netherlands Academy of Sciences) by a committee consisting of the following members: ERNST CRONE, Chairman of the Netherlands Maritime Museum, Amsterdam E. J. DIJKSTERHUIS, Professor of the History of Science at the Universities of Leiden and Utrecht R. J. FORBES, Professor of the History of Science at the Municipal University of Amsterdam M. G. J. M INNAERT, Professor of Astronomy at the University of Utrecht A. PANNEKOEK, Former Professor of Astronomy at the Municipal University of Amsterdam The Dutch texts of STEVIN as well as the introductions and notes have been translated into English or revised by Miss C. -
Index of Articles and Authors for the First Twenty-Four Numbers
Index of Articles and Authors for the first Twenty-four Numbers MARCH 1923 — NOVEMBER 1935 0 THE HYDROGRAPHIC REVIEW The Directing Committee of the I nternational H ydrographic B u r e a u will be pleased to consider articles for insertion in the Hydrographic Review. Such articles should be addressed to : The Secretary-General, I nternational H ydrographic B u r e a u Quai de Plaisance Mo n te -C arlo (Principality of Monaco) and should reach him not later than 1st February or ist August for the May or November numbers respectively. INDEX OF ARTICLES AND AUTHORS for the First Twenty-four Numbers MARCH 1923 - NOVEMBER 1935 FOREWORD This Index is in two parts : P a r t I. — Classification of articles according to the Subjects dealt with. P a r t II. — Alphabetical Index of the names of Authors of articles which have been published in The Hydrographic Review. NOTE. — Articles marked (R ) are Reviews of publications. Articles marked (E) are Extracts from publications. When no author’s name is given, articles have been compiled from information received by the Interna tional Hydrographic Bureau. Reviews of Publications appear under the name or initials of the author of the review. Descriptions of instruments or appliances are given in the chapters relating to their employment, in Chapter XIV (Various Instruments), or occasionally in Chapter XXT (Hints to Hydrographic Surveyors). CLASSIFICATION OF ARTICLES ACCORDING TO THE SUBJECTS DEALT WITH List of subjects I . — H ydrographic Offic e s a n d o th er Mar itim e a n d S c ie n t ific Organisations (Patrols, Life- saving, Observatories, Institutes of Optics)..................................................................................... -
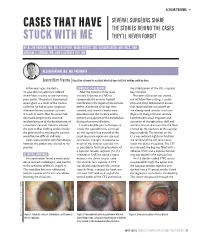
Cases That Have Stuck with Me
OCULAR TRAUMA s SEVERAL SURGEONS SHARE CASES THAT HAVE THE STORIES BEHIND THE CASES STUCK WITH ME THEY’LL NEVER FORGET BY ALLON BARSAM, MD, MA, FRCOPHTH; MARK KONTOS, MD; SOOSAN JACOB, MD, FRCS, DNB; MICHAEL E. SNYDER, MD; AND ELIZABETH YEU, MD ALLON BARSAM, MD, MA, FRCOPHTH Severe Blunt Trauma | A positive outcome for a patient who had been told that nothing could be done. A few years ago, I treated a SURGICAL PROCEDURE the stabilization of the IOL –capsular 41-year-old man who had suffered After the creation of the main bag complex. severe blunt trauma to one eye many incision, I injected an OVD to Phacoemulsification was carried years earlier. The patient experienced tamponade the anterior hyaloid out with low flow settings. I used a severe glare as a result of the trauma, membrane in the region of the zonular stop-and-chop technique to ensure such that he had to wear sunglasses defect. A cohesive OVD was then that minimal force was placed on whenever he was outdoors or even injected, and three iris hooks were the already weak zonular structures in a well-lit room. Also, his vision had placed to keep the iris back and to (Figure 2). Using a Simcoe cannula, decreased progressively since the prevent propagation of the iridodialysis I performed manual irrigation and incident because of the development of during phacoemulsification. aspiration of the epinuclear shell and a traumatic cataract. Doctors advised I used a double-pass technique to soft lens matter to ensure that the force the patient that nothing could remedy create the capsulorhexis, centered exerted on the contents of the capsular the glare and that treating the cataract on the capsular bag instead of the bag was gentle. -

Eleventh Edition
SUPPLEMENT TO April 15, 2009 A JOBSON PUBLICATION www.revoptom.com Eleventh Edition Joseph W. Sowka, O.D., FAAO, Dipl. Andrew S. Gurwood, O.D., FAAO, Dipl. Alan G. Kabat, O.D., FAAO Supported by an unrestricted grant from Alcon, Inc. 001_ro0409_handbook 4/2/09 9:42 AM Page 4 TABLE OF CONTENTS Eyelids & Adnexa Conjunctiva & Sclera Cornea Uvea & Glaucoma Viitreous & Retiina Neuro-Ophthalmic Disease Oculosystemic Disease EYELIDS & ADNEXA VITREOUS & RETINA Blow-Out Fracture................................................ 6 Asteroid Hyalosis ................................................33 Acquired Ptosis ................................................... 7 Retinal Arterial Macroaneurysm............................34 Acquired Entropion ............................................. 9 Retinal Emboli.....................................................36 Verruca & Papilloma............................................11 Hypertensive Retinopathy.....................................37 Idiopathic Juxtafoveal Retinal Telangiectasia...........39 CONJUNCTIVA & SCLERA Ocular Ischemic Syndrome...................................40 Scleral Melt ........................................................13 Retinal Artery Occlusion ......................................42 Giant Papillary Conjunctivitis................................14 Conjunctival Lymphoma .......................................15 NEURO-OPHTHALMIC DISEASE Blue Sclera .........................................................17 Dorsal Midbrain Syndrome ..................................45 -

Interesting and Artistic 1 2 3 Grand Prize Winner
s BEST OF 2018: PHOTO CONTEST 1 s SERGEI LUZHETSKIY, MD DANIEL DE SOUZA A Dog’s Cataract COSTA, MD s 2 A Spontaneous Displacement of the Lens WINNER GRAND PRIZE WINNER s PATRIK RAJS Gramophone Record 3 in the Eye INTERESTING AND ARTISTIC YONG s WINNERS OF KAM, MD Anterior CRST’S ANNUAL Segment Dysgenesis 2018 PHOTO CONTEST INTERESTING AND ARTISTIC 1 This is an image of an inherited cataract in a dog. 2 This photo is of the eye of a 46-year-old woman who presented with displacement of the lens into the anterior 4 chamber with no history of ocular trauma. 3 This photo is of the eye of a patient with presbyopia who underwent laser cataract surgery. A multifocal IOL was captured GRAND with a combination of two vintage Zeiss and Pentax lenses. WINNER PRIZE RARE AND UNUSUAL WINNER s This photo shows the eye of a newborn patient with DANIEL 4 increased IOP; a diffusely edematous, hazy, and enlarged DE SOUZA cornea; and an absent Schlemm canal and trabecular COSTA, MD meshwork on surgical exploration, consistent with severe A Prominent anterior segment dysgenesis. Symblepharon 5 The eye of this 5-year-old girl has epidermolysis bullosa and serious ocular manifestations of this condition. Biomicroscopy examination revealed the presence of 5 6 symblepharon in both eyes. The ocular complication was so severe that it deformed the palpebral anatomy. Significant keratoglobus in the eye of this patient with s AARON S. WANG, MD 6 Fish Tank Down Syndrome, who frequently rubs his eyes. This picture RARE AND UNUSUAL was taken just prior to corneal transplantation. -

To Assess the Intraoperative Complications in Small Incision Cataract Surgery and Visual Outcome
Acta Scientific Ophthalmology (ISSN: 2582-3191) Volume 3 Issue 8 August 2020 Research Article To Assess the Intraoperative Complications in Small Incision Cataract Surgery and Visual Outcome Smita Kunwar1*, Janak Poudel2 and Dr. Jyoti Kattige3 Received: July 14, 2020 1B. Optom Vittala International Institute of Ophthalmology, Bangalore, India Published: July 28, 2020 2B. Optom,Vittala International Institute of Ophthalmology Bangalore, India © All rights are reserved by Janak Poudel., 3Consultant Ophthalmologist, Fellowship in Glaucoma, Bangalore, India *Corresponding Author: Janak poudel B.Optom, Vittala International Institute of et al. Ophthalmology, Bangalore, India. DOI: 10.31080/ASOP.2020.03.0154 Abstract Background and Objective: Small incision cataract surgical procedure is the most normally performed surgical treatment for cataract in growing countries. This system is safe and effective to boom the output of cataract surgical services, at the identical time affordable. The present have a look at is undertaken to recognize the prevalence of intraoperative complications and how exceptional the complications may be minimized and dealt with and additionally its visual outcome. Method: A general of 471 instances turned into studied. Intraoperative complications have been studied and managed. Visual outcome following these complications have been studied with the aid of noting the BCVA after 1st week and 6th week of surgical treatment. Results: Out of 471 patients, 52(11%) patients The intraoperative complications were posterior capsular rupture occurred in 29 patients (55.8%), iris prolapse in 18 patients (34.6%), premature entry in 6 patients (11.5%), iridodialysis in 1 patient (1.9%), zonular dialysis in 1 patients (1.9%). 52 patients who had intraoperative problem came for follow up till sixth weeks, 28 cases (53.8%) had post-operative BCVA 6/9 or higher in 1st week and 24 cases had post-operative BCVA 6/18 or worse in 1st week. -

Sww Army Crosses Frontier of Reich
-------------r ~ — "Tr^VaS^''%f*, i -^ A «a •' * t .A -s '' ' . ■ ' - . > THURSDAY, DECEMBER 14, 1944 I ■ * ' Manchester Jivening Herald Buy Now to Spend in the. Future ■— Buy Bonds! The meetln* of the Board of Ad- Master John Keibiah, of 9 Bank street, was nine years old yastar- Gains Promotion Firemen Plan minlitration and deacons of Eman Wrecks Auto, dey. His mother arranged a party Average Daily Cirealatloii uel Lutheran church will be post Setting Pretty For Christmos The Weather About Town arid invited nine of hia neighbor For toe M toth a t November, 1844 Forecast ol U. H. Weather Bureau poned from this eveninit untill hood boy frienda to help Johnnie For Big Party g i f t c h a i r s a n d s u i t e s f o r l i v i n g r o o m Monday tvening The deacona will' Driver Skips celebrate the event. Games were ARE MOST WELCOME GIFTS! Increaelag eloudiBeaa, uat aa ■ In ttaa Itwntone, D#«l#r ntore, meet at eight o’clock and the played and prises swsrded. A LUXURIOUS LOUNGE CHAIRS THAT MEN 9,016 cold tonight; Hght m o w late to SW Main ntrMt, advcrtiMinent in Board of Adi^nlstration at 8:30. birthday sake and refreshments night, eudlag Saturday afteraooa; jiMtarday'a Harmld no piMe w»s Found Missing When the All Four Companies of REALLY LIKE, WITH HASSOCK Member of toa Aa8lt were sewed. TTie following boys tnereasiag winds tealghL iHvon OB tho (equine fU cx coffeo were present: Jerry Donahue, FOR PU R E COMFORT! Bureau ef dretilatloBa Trinity Faat Noble Grands As I a i c b I Police Arrive at| South End Department ■iakara.