A Review of Tobacco Harm Reduction Hearing Committee on Energy and Commerce House of Representatives
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Family Smoking Prevention and Tobacco Control Act’’
H. R. 1256 One Hundred Eleventh Congress of the United States of America AT THE FIRST SESSION Begun and held at the City of Washington on Tuesday, the sixth day of January, two thousand and nine An Act To protect the public health by providing the Food and Drug Administration with certain authority to regulate tobacco products, to amend title 5, United States Code, to make certain modifications in the Thrift Savings Plan, the Civil Service Retirement System, and the Federal Employees’ Retirement System, and for other purposes. Be it enacted by the Senate and House of Representatives of the United States of America in Congress assembled, DIVISION A—FAMILY SMOKING PRE- VENTION AND TOBACCO CONTROL ACT SECTION 1. SHORT TITLE; TABLE OF CONTENTS. (a) SHORT TITLE.—This division may be cited as the ‘‘Family Smoking Prevention and Tobacco Control Act’’. (b) TABLE OF CONTENTS.—The table of contents of this division is as follows: Sec. 1. Short title; table of contents. Sec. 2. Findings. Sec. 3. Purpose. Sec. 4. Scope and effect. Sec. 5. Severability. Sec. 6. Modification of deadlines for Secretarial action. TITLE I—AUTHORITY OF THE FOOD AND DRUG ADMINISTRATION Sec. 101. Amendment of Federal Food, Drug, and Cosmetic Act. Sec. 102. Final rule. Sec. 103. Conforming and other amendments to general provisions. Sec. 104. Study on raising the minimum age to purchase tobacco products. Sec. 105. Enforcement action plan for advertising and promotion restrictions. Sec. 106. Studies of progress and effectiveness. TITLE II—TOBACCO PRODUCT WARNINGS; CONSTITUENT AND SMOKE CONSTITUENT DISCLOSURE Sec. 201. Cigarette label and advertising warnings. -

Tool 2. Stakeholder-Specific Arguments for Tobacco Control
TOOL 2. STAKEHOLDER-SPECIFIC ARGUMENTS FOR TOBACCO CONTROL This tool provides arguments to convince different sectors and stakeholders to support and actively engage in tobacco control and actively participate in the NCM. The tool will also help health ministry officials answer questions from representatives of other sectors, and articulate a clear vision for why a whole-of-government approach is critical for tobacco control and related sustainable development objectives. Efforts to generate whole-of-government responses to tobacco control typically fail where tobacco is presented as a health challenge only. NCM engagement should be presented as more than just a benefit to, and responsibility of, the health sector. Clear, convincing and sector-specific arguments can take several forms, discussed below. Those involved in tobacco control planning should consider which line of argument or combination of arguments is most likely to persuade in a given context. The first argument is to emphasize whole-of-government efforts and policy coherence as necessary to fulfill WHO FCTC obligations. Entire governments sign the WHO FCTC, and thus it is legally incumbent upon all relevant government sectors to implement the treaty’s provisions. This means that different sectors are legally obliged to reconcile any contradictions between their mandates and the WHO FCTC. That the WHO FCTC is a legally binding international treaty, with reporting requirements, should be considered in priority setting discussions across ministries. Ministries could also be -

Impact-Of-Tobacco-Use-On-Cancer-In
Page 2 Executive Summary Tobacco use remains the world’s most preventable cause of death. Despite decades of declines in cigarette smoking prevalence, almost one-third of cancer deaths in the United States are still caused by smoking. This report describes the prevalence of tobacco use and its impact on cancers associated with tobacco use in Ohio. Key findings from this report include: • In 2016, 22.5 percent of Ohio adults ages 18 and older were current cigarette smokers compared to the median prevalence of 17.1 percent in the United States. • In Ohio in 2016, 2.7 percent of Ohio adults were cigar smokers, 5.7 percent used electronic cigarettes and 4.7 percent used smokeless tobacco. • The prevalence of current smoking among Ohio adults has decreased over the past 20 years. Groups for which the prevalence of current smoking was higher in 2016 include those ages 25 to 44, males, those with lower household income and education, lesbian, gay, bisexual and transgender adults, and those who have a disability or poor mental health. • County-level smoking prevalence among adult residents of Ohio ranged from 14 percent to 25 percent. Smoking was more common among residents of southern counties in Ohio. Cancer incidence and mortality rates were also highest in southern Ohio as well as southeastern Ohio. • Cigarette use among Ohio high school students decreased 74.5 percent from 2000 to 2016; however, this may partially be due to the increase in -e cigarette use in youth. • According to the U.S. Surgeon General, tobacco smoking is associated with 12 cancer sites/types. -

Family Smoking Prevention and Tobacco Control and Federal Retirement Reform
PUBLIC LAW 111–31—JUNE 22, 2009 FAMILY SMOKING PREVENTION AND TOBACCO CONTROL AND FEDERAL RETIREMENT REFORM VerDate Nov 24 2008 08:41 Jun 25, 2009 Jkt 079139 PO 00031 Frm 00001 Fmt 6579 Sfmt 6579 E:\PUBLAW\PUBL031.111 APPS06 PsN: PUBL031 dkrause on GSDDPC29 with PUBLIC LAWS 123 STAT. 1776 PUBLIC LAW 111–31—JUNE 22, 2009 Public Law 111–31 111th Congress An Act To protect the public health by providing the Food and Drug Administration with certain authority to regulate tobacco products, to amend title 5, United States June 22, 2009 Code, to make certain modifications in the Thrift Savings Plan, the Civil Service [H.R. 1256] Retirement System, and the Federal Employees’ Retirement System, and for other purposes. Be it enacted by the Senate and House of Representatives of the United States of America in Congress assembled, Family Smoking DIVISION A—FAMILY SMOKING PRE- Prevention and Tobacco Control VENTION AND TOBACCO CONTROL Act. ACT SECTION 1. SHORT TITLE; TABLE OF CONTENTS. 21 USC 301 note. (a) SHORT TITLE.—This division may be cited as the ‘‘Family Smoking Prevention and Tobacco Control Act’’. (b) TABLE OF CONTENTS.—The table of contents of this division is as follows: Sec. 1. Short title; table of contents. Sec. 2. Findings. Sec. 3. Purpose. Sec. 4. Scope and effect. Sec. 5. Severability. Sec. 6. Modification of deadlines for Secretarial action. TITLE I—AUTHORITY OF THE FOOD AND DRUG ADMINISTRATION Sec. 101. Amendment of Federal Food, Drug, and Cosmetic Act. Sec. 102. Final rule. Sec. 103. Conforming and other amendments to general provisions. -

The Findley Davies Virginia CEO Pay Report Estimated Compensation
Business Trends: Executive Compensation CEO ranking based on total The Findley Davies Virginia CEO Pay Report estimated compensation Compensation of CEOs at Virginia’s public companies with annual revenue of at least $1 billion COMPANY PERFORMANCE % Change % Change % Change Previous year % change Total 1 Year total Total Fiscal year Fiscal year Company name Executive name Base salary Previous year from Bonus Previous year from Total salary from Equity awards Long-term Other Total estimated total estimated from compensation shareholder return vs. revenues net income base salary previous bonus previous and bonus previous cash awards compensation compensation compensation previous (as disclosed return S&P500** ($ millions) ($ millions) year year year year in latest proxy) General Dynamics Corp., Falls Church Nicholas D. Chabraja $ 1,375,000 $ 1,300,000 5.8% $ 4,500,000 $ 3,500,000 29% $ 5,875,000 22.4% $ 25,619,046 N/A $ 404,603 $ 31,898,649 $ 15,634,585 104.0% $ 21,926,640 -33.78% 4.71% $ 29,300.0 $ 2,478.0 Norfolk Southern Corp., Norfolk Charles W. Moorman 950,000 800,000 18.8 1,759,400 862,400 104 2,709,400 63.0 9,639,106 N/A 132,239 12,480,745 12,637,254 -1.2 14,226,049 -4.30 34.19 10,661.0 1,716.0 Dominion Resources Inc., Richmond Thomas F. Farrell II 1,191,667 1,100,000 8.3 2,355,000 4,402,400 -47 3,546,667 -35.5 3,107,029 $ 4,380,000 626,421 11,660,117 12,930,286 -9.8 14,285,252 -21.14 19.16 16,290.0 1,836.0 Brinks Co.1, Richmond Michael T. -

Best Places to Launch a Career” Ranking That This Book Is Based Upon Requires Surveys of Career Services Directors, Students, and Employers Themselves
The Best Places toLaunch a Career This page intentionally left blank BusinessWeek Fast Track The Best Places toLaunch a Career Lindsey Gerdes New York Chicago San Francisco Lisbon London Madrid Mexico City Milan New Delhi San Juan Seoul Singapore Sydney Toronto Copyright © 2008 by McGraw-Hill. All rights reserved. Manufactured in the United States of America. Except as permitted under the United States Copyright Act of 1976, no part of this publication may be reproduced or distributed in any form or by any means, or stored in a database or retrieval system, without the prior written permission of the publisher. 0-07-160114-7 The material in this eBook also appears in the print version of this title: 0-07-149655-6. All trademarks are trademarks of their respective owners. Rather than put a trademark symbol after every occurrence of a trademarked name, we use names in an editorial fashion only, and to the benefit of the trademark owner, with no intention of infringement of the trademark. Where such designations appear in this book, they have been printed with initial caps. McGraw-Hill eBooks are available at special quantity discounts to use as premiums and sales promotions, or for use in corporate training programs. For more information, please contact George Hoare, Special Sales, at [email protected] or (212) 904-4069. TERMS OF USE This is a copyrighted work and The McGraw-Hill Companies, Inc. (“McGraw-Hill”) and its licensors reserve all rights in and to the work. Use of this work is subject to these terms. Except as permitted under the Copyright Act of 1976 and the right to store and retrieve one copy of the work, you may not decompile, disassemble, reverse engineer, reproduce, modify, create derivative works based upon, transmit, distribute, disseminate, sell, publish or sublicense the work or any part of it without McGraw-Hill’s prior consent. -

Bibliography on Smoking and Health. INSTITUTION Public Health Service (DHEW), Rockville, Md
DOCUMENT RESUME ED 068 857 CG 007 558 TITLE Bibliography on Smoking and Health. INSTITUTION Public Health Service (DHEW), Rockville, Md. National Clearinghouse for Smoking and Health. PUB DATE 71 NOTE 344p. AVAILABLE FROMSuperintendent of Documents, U. S. Government Printing Office, Washington, D. C. 20402 EDRS PRICE MF-S0.65 HC- $13.16 DESCRIPTORS Bibliographic Coupling; *Bibliographies; Booklists; Disease Control; Disease Rate; Diseases; Health; *Health Education; Indexing; Information Retrieval; *Literature Reviews; *Smoking; *Tobacco ABSTRACT This Bibliography includes all of the items added to the Technical Information Center of the National Clearinghouse for Smoking and Health from January through December 1971. The publication is broken down into eleven major categories. These are: (1) chemistry, pharmacology and toxicology; (2) mortality and morbidity;(3) neoplastic diseases;(4) non-neoplastic respiratory diseases; (5) cardiovascular diseases; (6) other diseases and conditions;(7) behavioral and educational research;(8) tobacco economics;(9) bills and legislation; and (10) general references. Also included in this bibliography are a cumulative author and organizational index and a cumulative subject index. U00 1971 NATIONAL CLEARINGHOUSE FOR SMOKING AND HEALTH BIBLIOGRAPHY on SMOKING AND HEALTH U.S. DEPARTMENT OF HEALTII. EDUCATION & WELFARE OFFICE OF EDUCATION THIS DOCUMENT HAS BEEN REPRO- DUCED EXACTLY AS RECEIVED FROM THE PERSON OR ORGANIZATION ORIG INATING IT. POINTS OF VIEW OR OPIN IONS STATED DO NOT NECESSARILY REPRESENT OFFICIAL OFFICE OF EDU- CATION POSITION OR POLICY. U.S. DEPARTMENT OF HEALTH, EDUCATION, AND WELFARE Public Health Service Health Services and Mental Health Administration FILMED FROM BEST AVAILABLE COPY 1 PREFACE This Bibliography includes all of the items added to theTechnical Information Center of the National Clearinghouse for Smoking and Health fromJanuary through December 1971. -

Restricting Youth Access and Exposure to Tobacco and Nicotine Delivery Products
Regulation of the Amherst Board of Health Restricting Youth Access and Exposure to Tobacco and Nicotine Delivery Products I. Statement of Purpose: Despite state laws prohibiting the sale of tobacco products to youth, access by youth to tobacco and nicotine delivery products is a major problem. In the interest of public health, it is the policy of the Town of Amherst to discourage youth from accessing and experimenting with tobacco and nicotine delivery products. The purpose of this regulation is to regulate establishments that sell tobacco and nicotine delivery products in a way that will: 1. reduce the number of youth who use tobacco and nicotine delivery products; 2. prevent the sale of tobacco and nicotine delivery products to individuals under the age of 21; 3. educate shop owners and employees who sell tobacco and nicotine delivery products within the Town of Amherst; and 4. reduce life-long consequences associated with tobacco and nicotine delivery product use. The Massachusetts Supreme Judicial Court has held that "...[t]he right to engage in business must yield to the paramount right of government to protect the public health by any rational means"[Druzik et al v. Board of Health of Haverhill, 324 Mass.129 (1949)]. Now, therefore the Amherst Board of Health intends to regulate the sale of tobacco and nicotine delivery products. II. Supporting Evidence: Tobacco use remains the number one cause of preventable disease, disability and death in the United States. Approximately 34 million American adults currently smoke cigarettes. Most tobacco product use begins during adolescence. In recent years, tobacco products have evolved to include various smoked, smokeless and electronic products(Adams, 2020; Wang et al, 2019). -

Appendices to Final Mem & Order\Appendix a Part 1.Wpd
APPENDIX A Excerpts from United States v. Philip Morris USA. Inc., et al. — F. Supp. 2d —, No. 99-2496 (GK), 2006 WL 2380622, 2006 WL 2380648, 2006 WL 2380632, 2006 WL 2381449, 2006 WL 2380650, and 2006 WL 2380681 (D.D.C. Aug. 17, 2006). [The Table of Contents from the opinion itself follows. Italicized headings appear in whole or in part in this appendix. Note that the page numbers in this table of contents do not correspond to the pages in this appendix. Footnotes have been omitted or moved to the text in brackets.] TABLE OF CONTENTS I. INTRODUCTION .......................................................1 A. Overview ........................................................1 B. Preliminary Guidance for the Reader..................................5 II. PROCEDURAL HISTORY...............................................10 III. CREATION, NATURE, AND OPERATION OF THE ENTERPRISE.....................................................15 A. Pre-1953 Overview–The Rise in American Smoking and the Status of Scientific Research on Smoking and Health ..............16 B. Creation of the Enterprise ..........................................18 C. TIRC/CTR -- Tobacco Industry Research Committee/Council for Tobacco Research-USA .........................................26 1. Selection and Approval of TIRC’s Scientific Advisory Board Members and Scientific Director .........................37 2. Research Activities of TIRC/CTR ..............................43 3. Public Relations Activities of TIRC/CTR ........................50 4. Publications and Public Statements -
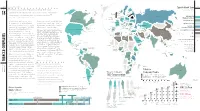
Tobacco Companies: Philip Morris Without Some of the Risks of Smoking
56 RESEARCH Says: Cigarette Market Share 57 Chapter These companies remain some of the most Sweden Finland by country, 2008 Norway . This is thanks in part to their endless British Estonia “profitable in the world American Russian United Kingdom Tobacco Latvia Fed. 18 London, inventive ways of undermining and circumventing regulation. Lithuania Denmark Russian Federation Ireland Philip Morris USA/ Anna Gilmore, University of Bath, UK, 2011 Netherlands Belarus Philip Morris International ” Canada Poland Imperial Tobacco Group Germany Bristol, UK Belgium n recent years, publicly traded tobacco Nicoventures, a separate company dedicated to Czech Rep. Ukraine British American Tobacco Philip Morris International Slovakia Rep. Lausanne, Switzerland Austria Moldova I companies have consolidated through creating alternative nicotine products that offer Switz. Hungary Slovenia— France —Croatia Romania Imperial Tobacco Group privatization and mergers. Today there are five the same experience expected from cigarettes Bosnia & Herzegovina Serbia Kazakhstan Japan Tobacco/ major private tobacco companies: Philip Morris without some of the risks of smoking. Bulgaria Albania —FYR Japan Japan Tobacco International Philip Morris International Italy Macedonia DPR Portugal Uzbekistan China National International, Altria/Philip Morris USA, Japan New York, NY Spain Georgia Kyrgyzstan Korea United States of America Greece Tobacco Corporation Korea Estimates of revenues from the global tobacco Armenia— —Azerbaijan Beijing State-Owned Tobacco Company Turkmenistan Rep Tobacco International, British American Altria Group/Philip Morris USA Turkey industry vary widely but are likely approaching Richmond, VA —Malta Syrian Tobacco, and Imperial Tobacco. In addition to Tunisia Cyprus— China Japan Tobacco/ Other Arab Rep. Japan Tobacco International half a trillion dollars annually. Although Lebanon*— Isl. -

Health Consequences of Smoking
The Health Consequences of Smoking Executive Summary This report of the Surgeon General on the health This approach separates the classification of the effects of smoking returns to the topic of active smok- evidence concerning causality from the implications ing and disease, the focus of the first Surgeon General’s of that determination. In particular, the magnitude of report published in 1964 (U.S. Department of Health, the effect in the population, the attributable risk, is Education, and Welfare [USDHEW] 1964). The first considered under “implications” of the causal deter- report established a model of comprehensive evidence mination. For example, there might be sufficient evi- evaluation for the 27 reports that have followed: for dence to classify smoking as a cause of two diseases those on the adverse health effects of smoking, the but the number of attributable cases would depend evidence has been evaluated using guidelines for as- on the frequency of the disease in the population and sessing causality of smoking with disease. Using this the effects of other causal factors. model, every report on health has found that smoking This report covers active smoking only. Passive causes many diseases and other adverse effects. Re- smoking was the focus of the 1986 Surgeon General’s peatedly, the reports have concluded that smoking is report and subsequent reports by other entities the single greatest cause of avoidable morbidity and (USDHHS 1986; U.S. Environmental Protection Agen- mortality in the United States. cy [EPA] 1992; California EPA 1997; International Agen- Of the Surgeon General’s reports published since cy for Research on Cancer [IARC] 2002). -

Tobacco Control in Ukraine
Tobacco Control in Ukraine The National report Ministry of Health of Ukraine ABSTRACT This report describes the status of tobacco control and tobacco control policies in Ukraine in mid–2008. It reviews progress following the adoption of national tobacco control legislation in 2005, and establishes a baseline for monitoring the implementation of the WHO Framework Convention on Tobacco Control (ratified in 2006) and the national tobacco control programme, which is being prepared by the government. The document presents an overview of the situation regarding tobacco use and related harm in Ukraine and policy responses and implementation of tobacco control measures at national and local levels. Keywords SMOKING – adverse effects – prevention and control HEALTH POLICY HEALTH PROMOTION TOBACCO – legislation TOBACCO INDUSTRY– legislation GUIDELINES UKRAINE Address requests about publications of the WHO Regional Office for Europe to: Publications WHO Regional Office for Europe Scherfigsvej 8 DK-2100 Copenhagen Ø, Denmark Alternatively, complete an online request form for documentation, health information, or for permission to quote or translate, on the Regional Office web site (http://www.euro.who.int/pubrequest). © World Health Organization 2009 All rights reserved. The Regional Office for Europe of the World Health Organization welcomes requests for permission to reproduce or translate its publications, in part or in full. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries.