Urinary Schistosomiasis Among Vulnerable Children in A
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
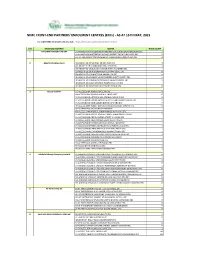
NIMC FRONT-END PARTNERS' ENROLMENT CENTRES (Ercs) - AS at 15TH MAY, 2021
NIMC FRONT-END PARTNERS' ENROLMENT CENTRES (ERCs) - AS AT 15TH MAY, 2021 For other NIMC enrolment centres, visit: https://nimc.gov.ng/nimc-enrolment-centres/ S/N FRONTEND PARTNER CENTER NODE COUNT 1 AA & MM MASTER FLAG ENT LA-AA AND MM MATSERFLAG AGBABIAKA STR ILOGBO EREMI BADAGRY ERC 1 LA-AA AND MM MATSERFLAG AGUMO MARKET OKOAFO BADAGRY ERC 0 OG-AA AND MM MATSERFLAG BAALE COMPOUND KOFEDOTI LGA ERC 0 2 Abuchi Ed.Ogbuju & Co AB-ABUCHI-ED ST MICHAEL RD ABA ABIA ERC 2 AN-ABUCHI-ED BUILDING MATERIAL OGIDI ERC 2 AN-ABUCHI-ED OGBUJU ZIK AVENUE AWKA ANAMBRA ERC 1 EB-ABUCHI-ED ENUGU BABAKALIKI EXP WAY ISIEKE ERC 0 EN-ABUCHI-ED UDUMA TOWN ANINRI LGA ERC 0 IM-ABUCHI-ED MBAKWE SQUARE ISIOKPO IDEATO NORTH ERC 1 IM-ABUCHI-ED UGBA AFOR OBOHIA RD AHIAZU MBAISE ERC 1 IM-ABUCHI-ED UGBA AMAIFEKE TOWN ORLU LGA ERC 1 IM-ABUCHI-ED UMUNEKE NGOR NGOR OKPALA ERC 0 3 Access Bank Plc DT-ACCESS BANK WARRI SAPELE RD ERC 0 EN-ACCESS BANK GARDEN AVENUE ENUGU ERC 0 FC-ACCESS BANK ADETOKUNBO ADEMOLA WUSE II ERC 0 FC-ACCESS BANK LADOKE AKINTOLA BOULEVARD GARKI II ABUJA ERC 1 FC-ACCESS BANK MOHAMMED BUHARI WAY CBD ERC 0 IM-ACCESS BANK WAAST AVENUE IKENEGBU LAYOUT OWERRI ERC 0 KD-ACCESS BANK KACHIA RD KADUNA ERC 1 KN-ACCESS BANK MURTALA MOHAMMED WAY KANO ERC 1 LA-ACCESS BANK ACCESS TOWERS PRINCE ALABA ONIRU STR ERC 1 LA-ACCESS BANK ADEOLA ODEKU STREET VI LAGOS ERC 1 LA-ACCESS BANK ADETOKUNBO ADEMOLA STR VI ERC 1 LA-ACCESS BANK IKOTUN JUNCTION IKOTUN LAGOS ERC 1 LA-ACCESS BANK ITIRE LAWANSON RD SURULERE LAGOS ERC 1 LA-ACCESS BANK LAGOS ABEOKUTA EXP WAY AGEGE ERC 1 LA-ACCESS -

Violence in Nigeria's North West
Violence in Nigeria’s North West: Rolling Back the Mayhem Africa Report N°288 | 18 May 2020 Headquarters International Crisis Group Avenue Louise 235 • 1050 Brussels, Belgium Tel: +32 2 502 90 38 • Fax: +32 2 502 50 38 [email protected] Preventing War. Shaping Peace. Table of Contents Executive Summary ................................................................................................................... i I. Introduction ..................................................................................................................... 1 II. Community Conflicts, Criminal Gangs and Jihadists ...................................................... 5 A. Farmers and Vigilantes versus Herders and Bandits ................................................ 6 B. Criminal Violence ...................................................................................................... 9 C. Jihadist Violence ........................................................................................................ 11 III. Effects of Violence ............................................................................................................ 15 A. Humanitarian and Social Impact .............................................................................. 15 B. Economic Impact ....................................................................................................... 16 C. Impact on Overall National Security ......................................................................... 17 IV. ISWAP, the North West and -

Advocacy Brief for Oyo State
OYO STATE FAMILY PLANNING/ CHILDBIRTH SPACING SERVICES OYO STATE Advocacy Kit Nigerian Urban Reproductive Nigerian Urban Reproductive Health Initiative Health Initiative HEALTHY FAMILY, HEALTHY STATE. FAMILY PLANNING/ CHILDBIRTH SPACING POLICY BRIEF Oyo State Health Indices Contraceptive Prevalence Rate: 37.4% Unmet Needs: 13.2% Infant Mortality: 69/1000 HIV/AIDS Prevalence: 3% Maternal Mortality Rate: 262/100,000 live Births Total Fertility Rate: 4.5 2013 NDHS OYO STATE POLICY BRIEF Oyo state prides herself as a pace setter in social, cultural and economic development. However the health indicators need a lot of improvement to keep the pace setter status. Oyo state has 262 maternal deaths per 100,000 live birth annually These maternal deaths are preventable with the use of reliable and appropriate interventions including family planning/ childbirth spacing (FP/CBS) services. Infant mortality stands at 69 deaths per 1,000 live births The unmet need for contraceptive use is 13.2% While the contraceptive prevalence Rate (CPR) is 37 .4% How to Improve Contraceptive Use in Oyo State. The Need for Specific Budget Line for Family Planning/ Child Spacing The NHIS and under 5/MDG fund initiative introduced by Oyo State as well as the new Health Insurance Agency provide a window of opportunity to mainstream FP/CBS in order to reach the undeserved and less privileged. There is the need to incorporate a specific budget line by creating a sub-code in the newly introduced IPSAS policy for FP/CBS programs. The continuous release of funds will create a huge opportunity to sustain FP services. Nigerian Urban Reproductive Health Initiative Adequate funding for FP/CBS is needed for logistics, capacity building, supervision, monitoring and demand creation to achieve improved uptake of FP/CBS Services. -

About the Contributors
ABOUT THE CONTRIBUTORS EDITORS MARINGE, Felix is Head of Research at the School of Education and Assistant Dean for Internationalization and Partnerships in the Faculty of Humanities, University of the Witwatersrand, South Africa. With Dr Emmanuel Ojo, he was host organizer of the Higher Education Research and Policy Network (HERPNET) 10th Regional Higher Education Conference on Sustainable Transformation and Higher Education held in South Africa in September 2015. Felix has the unique experience of working in higher education in three different countries, Zimbabwe; the United Kingdom and in South Africa. Over a thirty year period, Felix has published 60 articles in scholarly journals, written and co-edited 4 books, has 15 chapters in edited books and contributed to national and international research reports. Felix is a full professor of higher education at the School of Education, University of the Witwatersrand (WSoE) specialising in research around leadership, internationalisation and globalisation in higher education. OJO, Emmanuel is lecturer at the School of Education, University of the Witwatersrand, South Africa. He is actively involved in higher education research. His recent publication is a co-authored book chapter focusing on young faculty in South African higher education, titled, Challenges and Opportunities for New Faculty in South African Higher Education Young Faculty in the Twenty-First Century: International Perspectives (pp. 253-283) published by the State University of New York Press (SUNY). He is on the editorial board of two international journals: Journal of Higher Education in Africa (JHEA), a CODESRIA publication and Journal of Human Behaviour in the Social Environment, a Taylor & Francis publication. -

Wind Energy Evaluation for Electricity Generation Using WECS in Seven Selected Locations in Nigeria ⇑ O.S
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Covenant University Repository Applied Energy 88 (2011) 3197–3206 Contents lists available at ScienceDirect Applied Energy journal homepage: www.elsevier.com/locate/apenergy Wind energy evaluation for electricity generation using WECS in seven selected locations in Nigeria ⇑ O.S. Ohunakin a, , M.S. Adaramola b, O.M. Oyewola c a Mechanical Engineering Department, Covenant University, P.M.B 1023, Ota, Ogun State, Nigeria b Department of Energy and Process Engineering, Norwegian University of Science and Technology, Trondheim, Norway c Department of Mechanical Engineering, University of Ibadan, Oyo State, Nigeria article info abstract Article history: This paper statistically examine wind characteristics from seven meteorological stations within the Received 12 November 2010 North-West (NW) geo-political region of Nigeria using 36-year (1971–2007) wind speed data measured Received in revised form 14 February 2011 at 10 m height subjected to 2-parameter Weibull analysis. It is observed that the monthly mean wind Accepted 18 March 2011 speed in this region ranges from 2.64 m/s to 9.83 m/s. The minimum monthly mean wind speed was Available online 11 April 2011 recorded in Yelwa in the month of November while the maximum value is observed in Katsina in the month of June. The annual wind speeds range from 3.61 m/s in Yelwa to 7.77 m/s in Kano. It is further Keywords: shown that Sokoto, Katsina and Kano are suitable locations for wind turbine installations with annual Mean wind speed mean wind speeds of 7.61, 7.45 and 7.77 m/s, respectively. -
Federation Account Allocation Committee (FAAC)
Federation Account Allocation Committee (FAAC) (SEPTEMBER 2018 Disbursement) Report Date: November 2018 Data Source: National Bureau of Statistics / Office of The Accountant General of The Federation Contents Executive Summary 1 Federation Account Allocation Committee (FAAC) September 2018 Disbursement Summary of Gross Revenue Allocation by FAAC for the Month of August, 2018 Shared in September, 2018 2 Distribution of Revenue Allocation to FGN by FAAC for the Month of August, 2018 Shared in September, 2018 4 Distribution of Revenue Allocation to State and Local Governments by FAAC for the month of August, 2018 Shared in September, 2018 Abia 6 Adamawa 8 Akwa -ibom 11 Anambra 14 Bauchi 17 Bayelsa 20 Benue 22 Borno 25 Cross River 28 Delta 30 Ebonyi 33 Edo 35 Ekiti 37 Enugu 39 Gombe 41 Imo 43 Jigawa 46 Kaduna 49 Kano 52 Katsina 56 Kebbi 59 Kogi 62 Kwara 65 Lagos 67 Nasarawa 70 Niger 72 Ogun 75 Ondo 78 Osun 80 Oyo 83 Plateau 86 Rivers 88 Sokoto 91 Taraba 94 Yobe 96 Zamfara 98 Appendix 100 Methodology 120 Acknowledgements and Contacts 121 Executive Summary The Federation Account Allocation Committee (FAAC) disbursed the sum of N741.84bn to the three tiers of government in September 2018 from the revenue generated in August 2018. The amount disbursed comprised of N627.14bn from the Statutory Account, N114.54bn from Valued Added Tax (VAT) and N162.08bn exchange gain difference. Federal government received a total of N291.46bn from the N741.84bn. States received a total of N194.45bn and Local governments received N146.01bn. The sum of N53.05bn was shared among the oil producing states as 13% derivation fund while N40.00bn was transferred to Excess crude Account(ECA). -

Gusau Journal of Accounting and Finance, Vol
Gusau Journal of Accounting and Finance, Vol. 2, Issue 3, April, 2021 Gusau Journal of Accounting and Finance (GUJAF) Vol. 2 Issue 3, April, 2021 ISSN: 2756-665X A Publication of Department of Accounting and Finance, Faculty of Management and Social Sciences, Federal University Gusau, Zamfara State –Nigeria 1 Gusau Journal of Accounting and Finance, Vol. 2, Issue 3, April, 2021 BOARD COMPOSITION AND EARNINGS MANAGEMENT OF LISTED NON- FINANCIAL FIRMS IN NIGERIA Adeoye Lukmon Adewale Department of Accounting Osun State University, Osogbo [email protected] Olowookere Johnson Kolawole Department of Accounting Osun State University, Osogbo [email protected] Bankole Oluwaseun Emmanuel Department of Accounting Osun State University, Osogbo [email protected] Abstract In recent years, earnings management has gotten a lot of attention. This is owing to the fact that it is linked to the accuracy of published accounting reports. According to the academic literature, earnings management appears to be widespread among publicly traded firms. In response to calls for a higher proportion and composition of independent directors on boards and for the board of directors to be more financially sophisticated, the paper examined the effect of board composition on earnings management of listed non-financial firms in Nigeria from 2009 to 2018. Secondary data was used and extracted from various annual financial reports of the selected firms. The population for the study consisted of 117 listed non-financial firms in Nigeria as at December, 2018. This study used purposive sampling technique where 20 firms, whose data were accessible and available within the sample period of 2009 to 2018 were selected, being the most recent ten years within which the second corporate governance codes for quoted firms was introduced as a replacement to the 2003 SEC code. -

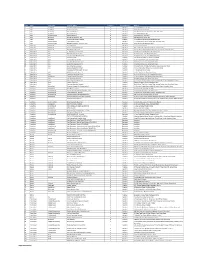
Agulu Road, Adazi Ani, Anambra State. ANAMBRA 2 AB Microfinance Bank Limited National No
LICENSED MICROFINANCE BANKS (MFBs) IN NIGERIA AS AT FEBRUARY 13, 2019 S/N Name Category Address State Description 1 AACB Microfinance Bank Limited State Nnewi/ Agulu Road, Adazi Ani, Anambra State. ANAMBRA 2 AB Microfinance Bank Limited National No. 9 Oba Akran Avenue, Ikeja Lagos State. LAGOS 3 ABC Microfinance Bank Limited Unit Mission Road, Okada, Edo State EDO 4 Abestone Microfinance Bank Ltd Unit Commerce House, Beside Government House, Oke Igbein, Abeokuta, Ogun State OGUN 5 Abia State University Microfinance Bank Limited Unit Uturu, Isuikwuato LGA, Abia State ABIA 6 Abigi Microfinance Bank Limited Unit 28, Moborode Odofin Street, Ijebu Waterside, Ogun State OGUN 7 Above Only Microfinance Bank Ltd Unit Benson Idahosa University Campus, Ugbor GRA, Benin EDO Abubakar Tafawa Balewa University Microfinance Bank 8 Limited Unit Abubakar Tafawa Balewa University (ATBU), Yelwa Road, Bauchi BAUCHI 9 Abucoop Microfinance Bank Limited State Plot 251, Millenium Builder's Plaza, Hebert Macaulay Way, Central Business District, Garki, Abuja ABUJA 10 Accion Microfinance Bank Limited National 4th Floor, Elizade Plaza, 322A, Ikorodu Road, Beside LASU Mini Campus, Anthony, Lagos LAGOS 11 ACE Microfinance Bank Limited Unit 3, Daniel Aliyu Street, Kwali, Abuja ABUJA 12 Achina Microfinance Bank Limited Unit Achina Aguata LGA, Anambra State ANAMBRA 13 Active Point Microfinance Bank Limited State 18A Nkemba Street, Uyo, Akwa Ibom State AKWA IBOM 14 Ada Microfinance Bank Limited Unit Agwada Town, Kokona Local Govt. Area, Nasarawa State NASSARAWA 15 Adazi-Enu Microfinance Bank Limited Unit Nkwor Market Square, Adazi- Enu, Anaocha Local Govt, Anambra State. ANAMBRA 16 Adazi-Nnukwu Microfinance Bank Limited Unit Near Eke Market, Adazi Nnukwu, Adazi, Anambra State ANAMBRA 17 Addosser Microfinance Bank Limited State 32, Lewis Street, Lagos Island, Lagos State LAGOS 18 Adeyemi College Staff Microfinance Bank Ltd Unit Adeyemi College of Education Staff Ni 1, CMS Ltd Secretariat, Adeyemi College of Education, Ondo ONDO 19 Afekhafe Microfinance Bank Ltd Unit No. -

Ibadan, Nigeria by Laurent Fourchard
The case of Ibadan, Nigeria by Laurent Fourchard Contact: Source: CIA factbook Laurent Fourchard Institut Francais de Recherche en Afrique (IFRA), University of Ibadan Po Box 21540, Oyo State, Nigeria E-mail: [email protected] [email protected] INTRODUCTION: THE CITY A. URBAN CONTEXT 1. Overview of Nigeria: Economic and Social Trends in the 20th Century During the colonial period (end of the 19th century – agricultural sectors. The contribution of agriculture to 1960), the Nigerian economy depended mainly on agri- the Gross Domestic Product (GDP) fell from 60 percent cultural exports and on proceeds from the mining indus- in the 1960s to 31 percent by the early 1980s. try. Small-holder peasant farmers were responsible for Agricultural production declined because of inexpen- the production of cocoa, coffee, rubber and timber in the sive imports and heavy demand for construction labour Western Region, palm produce in the Eastern Region encouraged the migration of farm workers to towns and and cotton, groundnut, hides and skins in the Northern cities. Region. The major minerals were tin and columbite from From being a major agricultural net exporter in the the central plateau and from the Eastern Highlands. In 1960s and largely self-sufficient in food, Nigeria the decade after independence, Nigeria pursued a became a net importer of agricultural commodities. deliberate policy of import-substitution industrialisation, When oil revenues fell in 1982, the economy was left which led to the establishment of many light industries, with an unsustainable import and capital-intensive such as food processing, textiles and fabrication of production structure; and the national budget was dras- metal and plastic wares. -

DREF Final Report Nigeria: Flash Floods
DREF final report Nigeria: Flash floods DREF operation n° MDRNG010 GLIDE n° FF-2011-000088-NGA 23 March, 2012 The International Federation of Red Cross and Red Crescent (IFRC) Disaster Relief Emergency Fund (DREF) is a source of un-earmarked money created by the Federation in 1985 to ensure that immediate financial support is available for Red Cross Red Crescent response to emergencies. The DREF is a vital part of the International Federation’s disaster response system and increases the ability of National Societies to respond to disasters. Summary: CHF 289,282 was allocated from the IFRC’s Disaster Relief Emergency Fund (DREF) on 25 July 2011 to support the Nigerian Red Cross Society (NRCS) to deliver assistance to some 12,500 beneficiaries conduct an in-depth assessment, support 2011 flood preparedness programmes and preposition relief materials. NRCS provided assistance to 7,500 people (approximately 1,500 households) in three most affected areas of Alimosho, Ebute Metta and Agege that was affected by the flood disaster caused by a 17-hour heavy downpour in Lagos State on 11 July 2011. In August 2011, NRCS also provided assistance to Nigerian Red Cross Society volunteers in Agege during and environmental 1,500 persons (approximately 300 sanitation of gutters. Photo: NRCS households) affected by a 22-hour storm that led to flash floods in Ibadan, Oyo State. NRCS collaborated with Lagos State Emergency Management Agency (LASEMA), Oyo State Emergency Management Agency, National Emergency Management Agency (NEMA) and other humanitarian agencies to carry out a joint assessment in both of the affected states. With IFRC’s support through DREF and technical support from the IFRC West Coast regional representation, the National Society distributed relief items, water and sanitation items and carried out sensitization and awareness campaigns in the most affected areas of Alimosho, Ebute Metta and Agege in Lagos State and two communities in Oyo State. -

Willingness to Pay for Cataract Surgery Is Much Lower Than Actual Costs in Zamfara State, Northern Nigeria
Willingness to pay for cataract surgery is much lower than actual costs in Zamfara State, northern Nigeria Nazaradden Ibrahim1 Jacqueline Ramke2 Francisco Pozo-Martin3 Clare E Gilbert4 1. Zamfara State Eye Care Programme, Ministry of Health, Gusau, Nigeria 2. Department of Epidemiology and Biostatistics, Faculty of Medicine and Health Sciences, University of Auckland, Auckland, New Zealand 3. Department of Global Health and Development, London School of Hygiene and Tropical Medicine, London, United Kingdom 4. International Centre for Eye Health, Clinical Research Unit, Department of Infectious & Tropical Diseases, London School of Hygiene and Tropical Medicine, London, United Kingdom Corresponding Author: Jacqueline Ramke [email protected] Dept of Epidemiology & Biostatistics, Faculty of Medical and Health Sciences, The University of Auckland. Private Bag 92019 Auckland Mail Centre Auckland 1142, New Zealand Conflict of interest: None of the authors have any proprietary interests or conflicts of interest related to this submission. Financial support: The study was funded by the Commonwealth Scholarship Scheme, Sightsavers UK and Hooper Scholarship. None of the funders contributed to the design of the study, data collection and analysis, interpretation of data or in writing the script, or the decision to submit the publication. Running head: Willingness to pay for cataract surgery in Nigeria This submission has not been published anywhere previously and it is not simultaneously being considered for any other publication. ABSTRACT Purpose: Direct medical and non-medical costs incurred by those undergoing subsidised cataract surgery at Gusau eye clinic, Zamfara state were recently determined. The aim of this study was to assess the willingness to pay for cataract surgery among adults with severe visual impairment or blindness from cataract in rural Zamfara, and to compare this to actual costs. -
S/No State City/Town Provider Name Category Coverage Type Address
S/No State City/Town Provider Name Category Coverage Type Address 1 Abia AbaNorth John Okorie Memorial Hospital D Medical 12-14, Akabogu Street, Aba 2 Abia AbaNorth Springs Clinic, Aba D Medical 18, Scotland Crescent, Aba 3 Abia AbaSouth Simeone Hospital D Medical 2/4, Abagana Street, Umuocham, Aba, ABia State. 4 Abia AbaNorth Mendel Hospital D Medical 20, TENANT ROAD, ABA. 5 Abia UmuahiaNorth Obioma Hospital D Medical 21, School Road, Umuahia 6 Abia AbaNorth New Era Hospital Ltd, Aba D Medical 212/215 Azikiwe Road, Aba 7 Abia AbaNorth Living Word Mission Hospital D Medical 7, Umuocham Road, off Aba-Owerri Rd. Aba 8 Abia UmuahiaNorth Uche Medicare Clinic D Medical C 25 World Bank Housing Estate,Umuahia,Abia state 9 Abia UmuahiaSouth MEDPLUS LIMITED - Umuahia Abia C Pharmacy Shop 18, Shoprite Mall Abia State. 10 Adamawa YolaNorth Peace Hospital D Medical 2, Luggere Street, Yola 11 Adamawa YolaNorth Da'ama Specialist Hospital D Medical 70/72, Atiku Abubakar Road, Yola, Adamawa State. 12 Adamawa YolaSouth New Boshang Hospital D Medical Ngurore Road, Karewa G.R.A Extension, Jimeta Yola, Adamawa State. 13 Akwa Ibom Uyo St. Athanasius' Hospital,Ltd D Medical 1,Ufeh Street, Fed H/Estate, Abak Road, Uyo. 14 Akwa Ibom Uyo Mfonabasi Medical Centre D Medical 10, Gibbs Street, Uyo, Akwa Ibom State 15 Akwa Ibom Uyo Gateway Clinic And Maternity D Medical 15, Okon Essien Lane, Uyo, Akwa Ibom State. 16 Akwa Ibom Uyo Fulcare Hospital C Medical 15B, Ekpanya Street, Uyo Akwa Ibom State. 17 Akwa Ibom Uyo Unwana Family Hospital D Medical 16, Nkemba Street, Uyo, Akwa Ibom State 18 Akwa Ibom Uyo Good Health Specialist Clinic D Medical 26, Udobio Street, Uyo, Akwa Ibom State.