Category: Article
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Letter from Melbourne Is a Monthly Public Affairs Bulletin, a Simple Précis, Distilling and Interpreting Mother Nature
SavingLETTER you time. A monthly newsletter distilling FROM public policy and government decisionsMELBOURNE which affect business opportunities in Australia and beyond. Saving you time. A monthly newsletter distilling public policy and government decisions which affect business opportunities in Australia and beyond. p11-14: Special Melbourne Opera insert Issue 161 Our New Year Edition 16 December 2010 to 13 January 2011 INSIDE Auditing the state’s affairs Auditor (VAGO) also busy Child care and mental health focus Human rights changes Labor leader no socialist. Myki musings. Decision imminent. Comrie leads Victorian floods Federal health challenge/changes And other big (regional) rail inquiry HealthSmart also in the news challenge Baillieu team appointments New water minister busy Windsor still in the news 16 DECEMBER 2010 to 13 JANUARY 2011 14 Collins Street EDITORIAL Melbourne, 3000 Victoria, Australia Our government warming up. P 03 9654 1300 Even some supporters of the Baillieu government have commented that it is getting off to a slow F 03 9654 1165 start. The fact is that all ministers need a chief of staff and specialist and other advisers in order to [email protected] properly interface with the civil service, as they apply their new policies and different administration www.letterfromcanberra.com.au emphases. These folk have to come from somewhere and the better they are, the longer it can take for them to leave their current employment wherever that might be and settle down into a government office in Melbourne. Editor Alistair Urquhart Some stakeholders in various industries are becoming frustrated, finding it difficult to get the Associate Editor Gabriel Phipps Subscription Manager Camilla Orr-Thomson interaction they need with a relevant minister. -

Australian Slang Dictionaryaustralian Slang Dictionary R4.17
R4.17 AUSTRALIAN SLANG DICTIONARYAUSTRALIAN SLANG DICTIONARY R4.17 It wasn’t easy but we’ve tried to include uniquely Australian slang here and to exclude British and American slang even though these are commonly used in Australia. We see no point in informing the world that “fridge” is Australian slang for a “refrigerator”. © Koala Net 1997-2007 www.koala-net.com.au/australian-slang.htm A Ace! : Excellent! Very good! Aerial pingpong : Australian Rules football Amber fluid : beer Ambo : ambulance, ambulance driver Ankle biter : small child Apples, she’ll be : It’ll be all right Arvo : afternoon Aussie (pron. Ozzie) : Australian Aussie salute : brushing away flies with the hand Avos : avocados B B & S : Bachelors’ and Spinsters’ Ball - a very enjoyable party usually held in rural areas Back of Bourke : a very long way away Bail (somebody) up : to corner somebody physically Bail out : depart, usually angrily Banana bender : a person from Queensland Barbie : barbecue (noun) Barrack : to cheer on (football team etc.) Bastard : term of endearment Bathers : swimming costume Battler : someone working hard and only just making a living Beaut, beauty : great, fantastic Big-note oneself : brag, boast Bikkie : biscuit (also “it cost big bikkies” - it was expensive) Billabong : an ox-bow river or watering hole Billy : teapot. Container for boiling water. Bingle : motor vehicle accident Bities : biting insects Bitzer : mongrel dog (bits of this and bits of that) Bizzo : business (“mind your own bizzo”) Black Stump, beyond the : a long way away, the -

Melbourne City Council MINUTES
CITY OF MELBOURNE Melbourne City Council MINUTES Meeting Number 30 Tuesday 30 November 2010 5pm PRESENT Lord Mayor, Robert Doyle (Chair) Deputy Lord Mayor, Susan Riley Councillor Peter Clarke Councillor Carl Jetter Councillor Jennifer Kanis Councillor Kevin Louey (arrived at 5.02pm) Councillor Ken Ong Councillor Brian Shanahan APOLOGIES Councillor Cathy Oke Confirmed at the meeting of Council on 21 December 2010. COMMENCEMENT OF MEETING AND APOLOGIES The meeting commenced at 5pm. The Chair, Lord Mayor, Robert Doyle, read the following acknowledgment statement: I welcome Councillors, Management and members of the public in attendance to the City of Melbourne. We respecully acknowledge that we are meeting on the traditional land of the Kulin Nation. This special place is now known by its European name of Melbourne. Today, Melbourne is one of the great multicultural cities of the world, a significant meeting place. For the great Kulin Nation, Melbourne has always been an important meeting place and location for events of social, educational, sporting and cultural significance. The Chair, Lord Mayor, Robert Doyle, advised the agenda comprised of: • seven Reports from Committee, three of which were confidential; and • eight Reports from Management, three of which were confidential. An apology was received from Councillor Oke. The Chair, Lord Mayor, Robert Doyle, acknowledged the change of leadership of the state government, stating that he wished to: • thank former Premier John Brumby and his cabinet for their contribution to public life and the city; • congratulate John Brumby for service to the state as opposition leader, treasurer and premier; • thank the Brumby family as well as members who retired, were defeated at election or lost office and that their contribution should be honoured; and • congratulate new Premier Ted Baillieu and the Coalition for their win in the election and that Council is looking forward to working with him and the new team. -

Vic Libs Reeling Over Secret Baillieu Tape PUBLISHED: 24 JUN 2014 12:38:00 | UPDATED: 25 JUN 2014 05:58:53
Vic Libs reeling over secret Baillieu tape PUBLISHED: 24 JUN 2014 12:38:00 | UPDATED: 25 JUN 2014 05:58:53 LUCILLE KEEN AND MATHEW DUNCKLEY An embarrassing leaked recording of former Victorian premier Ted Baillieu criticising other Liberal MPs to journalists has inflamed tensions in the party. In the recording of a conversation with an Age journalist Mr Baillieu slammed the factional divides which led to the selection of Tim Smith to contest the blue-ribbon seat of Kew at the next election. Mr Baillieu supported front bencher Mary Wooldridge in her unsuccessful tilt for the seat. Mr Baillieu also criticises MPs Michael Gidley and Murray Thompson and the conservative faction that overturned Denis Napthine as opposition leader in 2002 to be replaced by Robert Doyle. “The technique with Michael Gidley was the technique with Tim Smith,” Mr Baillieu said. He also criticised balance-of-power MP Geoff Shaw. Mr Shaw quit the parliamentary Liberal Party, citing a lack of faith in the leadership, contributing to Mr Baillieu’s resignation hours later. “Shaw has been sponsored into his position by a bunch of people from the very first day led by Bernie Finn and some crazy mates in the parliamentary team and a very senior member of the organisation who is very close to [federal MP] Kevin Andrews,” he said. Mr Shaw said Mr Baillieu can hold his own opinions but the “sad thing is he didn’t allow” his backbenchers any opinions while he was premier. He said claims about his backers were false and he was in a safe Liberal seat, “he takes for granted”. -

Exploring the Culture of Youth Homelessness in Melbourne
HANGING OUT IN THE CONCRETE JUNGLE: EXPLORING THE CULTURE OF YOUTH HOMELESSNESS IN MELBOURNE Submitted By Jennifer L. Hill BSocSc(YthSt) (Hons) A thesis submitted in total fulfilment of the requirements of the degree of Master of Philosophy School of Arts and Sciences Faculty of Arts and Sciences Australian Catholic University Research Services Locked Bag 4115 Fitzroy Victoria 3065 I STATEMENT OF AUTHORSHIP AND SOURCES This thesis contains no material published elsewhere or extracted in whole or in part from a thesis by which I have qualified for or been awarded another degree or diploma. No parts of this thesis have been submitted towards the award of any other degree or diploma in any other tertiary institution. No other person’s work has been used without due acknowledgment in the main text of the thesis. All research procedures reported in the thesis received the approval of the Australian Catholic University Research Ethics Committee. Editorial assistance in the preparation of this thesis was obtained from Ms. R. Almond. Editorial services included proof reading the final draft of the thesis. Jennifer Hill ________________________ II ACKNOWLEDGEMENTS Hanging Out in the Concrete Jungle is the product of the generosity, input, patience and support of those who made this journey with me. Although I cannot divulge their true names, I wish to acknowledge and express my gratitude to the young people who contributed their time and invaluable insights to this research. It took a great deal of courage or ‘dash’ (as participants would say) to speak so openly about their lives and experiences. I feel honoured to have been entrusted with their stories and photographs that together shaped this thesis, I hope that my interpretation has done them justice. -

A Typology of the Traditional Games of Australian Aboriginal and Torres Strait Islander Peoples
A Typology of the Traditional Games of Australian Aboriginal and Torres Strait Islander Peoples Ken Edwards Author Ken Edwards has studied health and physical education, environmental science and sports history. He has taught health and physical education at both primary and secondary school level and has been a Head of Health and Physical Education at various schools. Ken completed a Ph.D. through UQ and has been an academic at QUT and Bond University and is now an Associate Professor in Sport, Health and Physical Education at USQ (Springfield Campus). Ken has had involvement in many sports as a player, coach and administrator. Wener ganbony tilletkerrin? What shall we play (at) first (Language of the Western people of Victoria) A Typology of the Traditional Games of Australian Aboriginal and Torres Strait Islander Peoples Ken Edwards Artwork by Aboriginal artist Maxine Zealey (of the Gureng Gureng people in Queensland). Copyright © 2012 by Ken Edwards. All rights are reserved. No portion of this book may be reproduced in any form or by any means without the written permission of the Copyright owner. ISBN 978-0-9872359-0-9 Paper size: 16.5cms X 23 cms Page printing for ebook: Scale to fit A4 Acknowledgements Great excitement existed amongst the players in this game, which was begun in this manner: each player had one of these toys in his hands, standing at a mark on the ground some 30 yards or 40 yards from the disc. The thrower standing on the mark would measure the distance with his eye, and turning round would walk some few yards to the rear, and suddenly turning to the front would run back to the mark, discharging his weitweit with great force at the disc. -
Melbourne Creating a Great Street
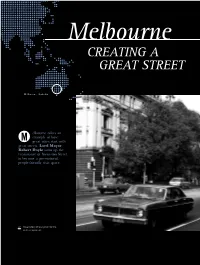
Melbourne Creating A Great STREET Melbourne, Australia elbourne offers an example of how M great cities start with great streets. Lord Mayor Robert Doyle sums up the renaissance of Swanston Street to become a pre-eminent, people-friendly civic space. 01 Swanston Street prior to the redevelopment. 23 case study The Challenge Swanston Street has been the most frequented pedestrian strip in Melbourne since the 1850s and has the busiest tram route in the world. Melbourne’s civic spine is trodden on by more pedestrians per day than When I became Lord Mayor Regent Street, London. in 2008, the road was a It is home to some of the mess. At night, private city’s marvellous historic vehicles could use it, but buildings, including the during the day, it operated Town Hall, State Library as a quasi-mall that allowed and St Paul’s Cathedral. buses, taxis and delivery vans only at certain times. It is also the main It was confusing and parade route, with grand disjointed, and also unsafe. processions celebrating Motorists, pedestrians and Australia Day, Moomba, cyclists were not happy. Christmas, Melbourne Cup, Australian Football As a city, we needed to League Grand Final and come up with an engineering Anzac Day travelling down solution to fix the traffic the thoroughfare. chaos and improve safety and amenity on the thoroughfare. The catalyst for action for me happened in September 2008, when a young, pregnant cyclist slipped on the tram tracks and was killed by a tour bus that ran over her. February 2015 February 2015 01 • • ISSUE 6 ISSUE 6 The Solution The City of Melbourne wanted to develop Swanston Street as the pre- eminent civic space that provides enhanced experiences for shoppers, visitors, workers, cyclists and tram patrons. -

And Boundaries: a Perceptual Dialectology of Australian English
‘Bogans’ and Boundaries: A perceptual dialectology of Australian English by Madalyn B. Danielson … Undergraduate Honors Thesis NYU Department of Linguistics Spring 2014 1 ‘Bogans’ and Boundaries: A perceptual dialectology of Australian English by Madalyn B. Danielson Although linguistics is primarily centered on the study of language competence, Dennis Preston has put forth strong arguments for the legitimization of perceptual dialectology, or the study of “folk” perceptions of language, as a proper subfield of sociolinguistics. Traditionally, structuralists have regarded this subfield with criticism, as the study of nonlinguists’ perceptions of speech varieties was thought to have little to do with the objective, ‘scientific’ approach to language research. Yet Preston claims that the study of nonlinguists’ perception of language is a critical component of linguistics, as these views have often inspired and informed empirical research in the first place (1999:xxiv). Furthermore, folk perceptions of language can impact the production of language itself, as well as affect the larger processes of language change (Preston 1989:2). The present study is an undergraduate thesis inspired by Preston’s original research methods and Bucholtz et al.’s perceptual dialectology of California (2007, 2008). This paper examines the data collected from 85 surveys distributed primarily within Sydney, New South Wales that were designed to elicit Australians impressions and perceptions of variation in Australian English. The paper will explore what types of attitudes Australian English speakers have to their own language and how those attitudes manifest through overt and covert expression. Crucially, it has been generally recognized among linguists that Australian English (hereafter, AusE) is “remarkably” homogeneous when compared to other dialects of English (namely British and American English), regardless of regional distribution or 2 speakers’ social characteristics (e.g. -
A Fair Dinkum Aussie Dictionary a Collection of Aussie Terms and Sayings
A fair dinkum Aussie Dictionary A collection of Aussie terms and sayings “Mate, give this a burl!” “You little beauty! “Grouse!!” “Cripes, fire up the billy, pass me a bickie and cop a look at this.” A fair dinkum Aussie Dictionary A collection of Aussie terms and sayings “Whether you’re a bloke or a sheila, have a go at our Aussie lingo. In an arvo, you’ll be speaking like you’re from Down Under!” ustralian English is Many early Australianisms were Not included in this collection, While the terms which made justifiably notorious for its words taken over by or derived but something you are bound to it into this dictionary are as Acolourful and seemingly from the languages spoken by encounter at some point during Australian as meat pie, we’d have endless collection of slang terms Aboriginal tribes. Thus, words your stay, is the popular Aussie to have more hide than Ned Kelly and sayings. Some Australianisms such as boomerang, billabong, habit of nicknaming mates and to suggest that this is the last such as “she’ll be right, mate” kangaroo and cockatoo soon cobbers by embellishing the word on the matter. and “fair dinkum” are well known became part of the general endings of their first names with around the world, but these are language (lingo) spoken by all an “o”. Like all languages, Aussie English just the start. Australians. is growing and changing with the For example, if your name is David, times. And while you’ll be flat out Many a visitor to the land Down Australian place names of you may find yourself being called like a lizard drinking if you try to Under has been more than a Aboriginal origin can be another Davo; likewise, Stevens can expect make head or tail of all the local little mystified when told that source of amazement to to be called Stevo; and Johns to be lingo, this book will, hopefully, give it is his or her turn to “shout” newcomers – especially tongue- called Johnno. -

Information Booklet
COMMUNITY KNOWLEDGE SCIENCE ART Great societies are defined through their art, science and knowledge. W onderment W alk W onderment W alk wondermentwalk.org.au wondermentwalk.org.au “It is a wonderful addition to our city. You’ve taken vision and with hard work, turned it into a very beautiful reality” The Right Honourable Lord Mayor of Melbourne, Robert Doyle WONDERMENT WALK VICTORIA LIMITED MISSION STATEMENT / THE VISION 2 INDEX FRIENDS OF WONDERMENT WALK 3 WONDERMENT WALK EXHIBITION - PHOTOS 6 WONDERMENT WALK LAUNCH - PHOTOS 8 WONDERMENT WALK FLOOR TALK - PHOTOS 10 THE COLLECTION 11 LOCATIONS 20 FOUNDATION SUPPORT 21 3 MISSION STATEMENT Great societies are defined through their art, science and knowledge. Wonderment Walk Victoria will strengthen Melbourne’s reputation as a creative city of knowledge by enhancing walking routes connecting places of significance with sculptural wonderments. We aim to create accessible open-air galleries of artworks, sculptures and installations combining science, mathematics and art to engage passers- by with wonder, delight and curiosity. THE VISION Wonderment Walk installations use art as a science communications medium. The works are intended to engage the general public, inspiring curiosity and encouraging innovative thoughts and expression. We aim to create open-air galleries that excite and inspire; galleries without walls and without boundaries; galleries to complement and enhance Victoria’s reputation nationally and internationally as a place of art, culture, innovation and knowledge. 2 FRIENDS OF DIGNITARIES “I hope that Wonderment Walk will further enhance Victoria’s reputation as a multicultural international hub of culture, science, business, innovation and as a Knowledge City.” Eddie Kutner, Wonderment Walk Founder and Chair “I commend the vision of the team behind Wonderment Walk. -
'Aussie Bloke': Gender, Class and Contextualizing a Hegemony Of
Looking out for the ‘Aussie Bloke’: Gender, Class and Contextualizing a Hegemony of Working-Class Masculinities in Australia. Kirsty Whitman School of Humanities and Social Science Discipline of Gender Studies and Social Analysis (60%) and Politics (40%). Submitted for the degree of Doctor of Philosophy June 2013. Contents Abstract …..v Declaration ….. vi Acknowledgements ….. vii Introduction …..1 Contextualizing a Hegemony of Centralizing Working-Class Masculinity ….. 5 Gender and Legitimate Australian-ness ….. 10 Format and Structure ….. 12 Chapter 1: Theorizing the ‘Aussie Bloke’: Gender, Masculinities, Class and the Hegemony of Centralizing Working-Class Masculinities Introduction ….. 21 Gender and Masculinity ….. 23 Modern and Postmodern Accounts of Gender: Masculinity Theory, Sexuality and Discourse ….. 25 Masculinity/Masculinities: Debates and Clarifications ….. 28 Recognizing Variations and Fluidity: Multiple Masculinities ….. 33 Contextualizing Hegemonic Masculinity/Masculinities, Hegemony and Men ….. 37 Hegemony, Gender and Class ….. 46 Intersections of Class and Gender ….. 49 Class: Moving Beyond Economic Categories ….. 50 Theoretical Conclusions and Use of Terms ….. 61 Conclusion ….. 64 Chapter 2: It’s Not Just Something Working-Class Men Do: The Methodological Journey to a Discursive Approach to Centralizing Working-Class Masculinities Introduction ….. 67 Identifying as a Working-Class Woman ….. 70 Terminology: The Methodological Journey to Centralizing Working-Class Masculinity ….. 73 Qualitative Methodology and Feminist Research ….. 75 ii Critical Discourse and Textual Analysis ….. 78 Recruitment of Participants ….. 83 The Reflexive Standpoint of the Participants: Gender, Class and Mistrust of Academic Elites ….. 87 Gender as an Issue ….. 88 Culture and Class ….. 91 Telephone Interviews ….. 92 Question Choice ….. 95 Reading the Unsaid ….. 96 Changes in Scope and Methodology: The Eventual Structure of this Study …. -

Ad Astra No.133 Dec 2017
Ad Astra The Geelong College Community Magazine Issue No 133 December 2017 From the Editor to all Australians who did not come home in the First World War. This service was part of a remarkable reunion involving both The Geelong College and Geelong Grammar School in France, where we relived a moment in our schools’ shared history from 100 years ago. See page 36 to read about the Albert Centenary Reunion. Another special event this year was The Geelong College Gala Ball, organised by our parent associations. Nearly 550 members of our community came together at The Pier Geelong in October for the ball (page 34). We encourage you to take a moment to watch the video commissioned for the occasion, by scanning the QR code on page 35. “Celebrating Who We Are” is quite a moving production – the result of a collaboration between College staff member Sam McIntosh and Year 12 student Oliver Manton, showing College life through the eyes of a young student. As 2017 draws to a close, this edition of Ad Astra provides Indeed, the College community gives us much cause to glimpses into the many and varied learning experiences celebrate. Our College Prefects have shown leadership which have shaped our students, as well as our Old beyond school, in the Geelong region (page 8); staff, Collegian community. parents and students have worked together to help We begin on the next page with Chair of Council Dr Hugh disadvantaged children in local schools (page 31); Seward AM, who writes about the exciting opportunities and the Geelong College Connect platform for Old that lie ahead with the College Master Plan.