Morphometric Study of a Huge Elongated Styloid Process
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Head& Neck II
nd Dr.Ban I.S. head & neck anatomy 2 y جامعة تكريت كلية طب اﻻسنان مادة التشريح املرحلة الثانية أ.م.د. بان امساعيل صديق 6102-6102 1 nd Dr.Ban I.S. head & neck anatomy 2 y Triangles of the neck: Each side of the neck is divided into anterior and posterior triangles by the obliquely placed sternocleidomastoid muscle. The anterior triangle is bounded by the midline, lower border of mandible and anterior border of sternocleidomastoid muscle. The posterior triangle is bounded by the posterior border of sternocleidomastoid, the anterior border of trapezius and the clavicle. Sternocleidomastoid: This muscle has two heads of origin below: that from the sternal manubrium is a rounded tendon and that from the clavicle is a flat tendon. A triangular interval exists between the two above the sternoclavicular joint, and the lower end of the internal jugular vein lies behind. The muscle is attached by a tendon to the lateral surface of the mastoid process and the lateral half of the superior nuchal line. The muscle is crossed superficially by the great auricular nerve, the external jugular vein and the transverse cervical nerve. 2 nd Dr.Ban I.S. head & neck anatomy 2 y Nerve supply. By the spinal part of the accessory nerve. Action. Contraction of one muscle tilts the head towards the ipsilateral shoulder, and rotates the head to the opposite side. When both muscles acting together, draw the head forwards. Trapezius muscle: It arises from medial third of superior nuchal line, external occipital protuberance, ligamentum nuchae, spine of 7th cervical vertebra, and all thoracic vertebrae . -

Comparative Study of the Digastric and the Stylohyoid Muscles Between
Original Article https://doi.org/10.5115/acb.20.301 pISSN 2093-3665 eISSN 2093-3673 Comparative study of the digastric and the stylohyoid muscles between wild boars (Sus scrofa scrofa) and domestic swine (Sus scrofa domesticus): revisiting the gross anatomy Henrique Inhauser Riceti Magalhães1, Jeferson Borges Barcelos2, Fabiano Braz Romão3, Tânia Ribeiro Junqueira Borges2, Roseâmely Angélica de Carvalho-Barros4, Maria Angelica Miglino1, Frederico Ozanam Carneiro e Silva2, Lucas de Assis Ribeiro2 1Department of Surgery, School of Veterinary Medicine and Animal Sciences, University of São Paulo, São Paulo, 2Animal Anatomy Laboratory, School of Veterinary Medicine and Animal Sciences, Federal University of Uberlândia, Uberlândia, 3Animal Anatomy Laboratory, School of Veterinary Medicine, University Center of Patos de Minas, Patos de Minas, 4Anatomy Laboratory, School of Biological Sciences, Federal University of Catalão, Catalão, Brazil Abstract: Considering Suidae Familie as a perfect and viable experimental biomedical model for research applied to human medicine, it has been sought to describe the comparative anatomy of the digastric and the stylohyoid muscles between boars and domestic swine. Heads of Sus scrofa scrofa and Sus scrofa domesticus were dissected. The digastric muscle presented only one muscle belly as anatomical component of a tendinous origin in the jugular process of the occipital bone, and muscle insertion in the midventral edge of the caudal two thirds of the body of the mandible. Thus, its function is fundamentally associated with the lowering and the retracting of the mandible which, by the way, can deliver greater muscle power at lesser energy expense. For the stylohyoid muscle, the tendinous origin was in the laterocaudal edge of the dorsal third of the stylohyoid bone. -

An Anomalous Digastric Muscle in the Carotid Sheath: a Case Report with Its
Short Communication 2020 iMedPub Journals Journal of Stem Cell Biology and Transplantation http://journals.imedpub.com Vol. 4 ISS. 4 : sc 37 ISSN : 2575-7725 DOI : 10.21767/2575-7725.4.4.37 8th Edition of International Conference on Clinical and Medical Case Reports - An anomalous digastric muscle in the carotid sheath: a case report with its embryological perspective and clinical relevance Srinivasa Rao Sirasanagandla Sultan Qaboos University, Oman Abstract Key words: Although infrahyoid muscles show considerable variations in Anterior belly, Posterior belly, Variation, Stylohyoid muscle, My- their development, existence of an anomalous digastric muscle lohyoid muscle, Hyoid bone in the neck was seldom reported. During dissection of trian- Anatomy gles of the neck for medical undergraduate students, we came across an anomalous digastric muscle in the carotid sheath of There is a pair of digastric muscles in the neck, and each digas- left side of neck. It was observed in a middle-aged cadaver at tric muscle has the anterior belly and the posterior belly. The College of Medicine and Health Sciences, Sultan Qaboos Uni- anterior belly is attached to the digastric fossa on the base of versity, Muscat, Oman. Digastric muscle was located within the the mandible close to the midline and runs toward the hyoid carotid sheath between the common and internal carotid arter- bone. The posterior belly is attached to the notch of the mas- ies and internal jugular vein. It had two bellies; cranial belly and toid process of the temporal bone and also runs toward the caudal belly which were connected by an intermediate tendon. -

Genioglossus Muscle Is the Largest Extrinsic Tongue Muscle and Upper Airway Dilator
PLEASE TYPE THE UNIVERSITY OF NEW SOUTH WALES Thesis/Dissertation Sheet Surname or Family name: Kwan First name: Benjamin Other name/s: Chi Hin Abbreviation for degree as given in the University calendar: PhD School: Prince of Wales Hospital Clinical School Faculty: Medicine Title: Breathing movements of the human tongue and genioglossus measured with ultrasound imaging Abstract 350 words maximum: (PLEASE TYPE) Genioglossus muscle is the largest extrinsic tongue muscle and upper airway dilator. To maintain pharyngeal patency within and between breaths, delicate moment-to-moment coordination of pharyngeal muscles activity and drive is required. Dynamic pharyngeal muscle movement in response to the neural input during sleep/wake states is not clearly understood. This thesis reports a novel ultrasound method to visualise and measure dynamic genioglossus motion in healthy and OSA subjects. In Chapter 2, the method revealed ~1 mm predominantly anterior peak displacement within a 50 mm2 area in the infero-posterior genioglossus in healthy awake subjects during quiet breathing. Motion within this area was non-uniform. The method has good reliability, intraclass correlation coefficient (ICC) of 0.85 across separate imaging sessions. Chapter 3 reported good agreement between ultrasound and tagged MRI in measuring regional tongue motion in healthy and OSA subjects, with an ICC of 0.79. Compared to MRI, ultrasound revealed greater anterior displacement in the posterior tongue (mean difference of 0.24 ± 0.64 mm, 95% limits of agreement: 1.03 to -1.49). Chapter 4 examined influence of respiratory mechanics and drive on genioglossus movement. Inspiration against a resistive load increased posterior genioglossus motion, but it had less anterior and more inferior displacement at the highest inspiratory resistance. -

Head and Neck of the Mandible
Relationships The parotid duct passes lateral (superficial) and anterior to the masseter muscle. The parotid gland is positioned posterior and lateral (superficial) to the masseter muscle. The branches of the facial nerve pass lateral (superficial) to the masseter muscle. The facial artery passes lateral (superficial) to the mandible (body). On the face, the facial vein is positioned posterior to the facial artery. The sternocleidomastoid muscle is positioned superficial to both the omohyoid muscle and the carotid sheath. The external jugular vein passes lateral (superficial) to the sternocleidomastoid muscle. The great auricular and transverse cervical nerves pass posterior and lateral (superficial) to the sternocleidomastoid muscle. The lesser occipital nerve passes posterior to the sternocleidomastoid muscle. The accessory nerve passes medial (deep) and then posterior to the sternocleidomastoid muscle. The hyoid bone is positioned superior to the thyroid cartilage. The omohyoid muscle is positioned anterior-lateral to the sternothyroid muscle and passes superficial to the carotid sheath. At the level of the thyroid cartilage, the sternothyroid muscle is positioned deep and lateral to the sternohyoid muscle. The submandibular gland is positioned posterior and inferior to the mylohyoid muscle. The digastric muscle (anterior belly) is positioned superficial (inferior-lateral) to the mylohyoid muscle. The thyroid cartilage is positioned superior to the cricoid cartilage. The thyroid gland (isthmus) is positioned directly anterior to the trachea. The thyroid gland (lobes) is positioned directly lateral to the trachea. The ansa cervicalis (inferior root) is positioned lateral (superficial) to the internal jugular vein. The ansa cervicalis (superior root) is positioned anterior to the internal jugular vein. The vagus nerve is positioned posterior-medial to the internal jugular vein and posterior-lateral to the common carotid artery. -

Styloglossus Muscle: a Critical Landmark in Head and Neck Oncology
European Annals of Otorhinolaryngology, Head and Neck diseases 135 (2018) 421–425 Available online at ScienceDirect www.sciencedirect.com Review Styloglossus muscle: a critical landmark in head and neck oncology a, b a c O. Laccourreye ∗, R.K. Orosco , F. Rubin , F.C. Holsinger a Service d’otorhinolaryngologie et de chirurgie cervicofaciale, HEGP, université Paris Descartes Sorbonne Paris Cité, AP–HP, 20–40, rue Leblanc, 75015 Paris, France b Departments of otorhinolaryngology, Head and Neck Surgery, university of California San Diego, San Diego, CA, USA c Department of otolaryngology, school of medicine, Stanford University, 875 Blake Wilbur Drive, 94305-5820 Palo Alto, CA, USA a r t i c l e i n f o a b s t r a c t Keywords: Goal: To document the role of the styloglossus muscle (SG) in head and neck oncology and at the time Oropharynx of surgical treatment and mandibular preservation surgery for squamous cell carcinoma of the lateral Oropharyngectomy oropharynx (SCCLO). Squamous cell carcinoma Method: Based on a search conducted within the Pubmed, Embase, and Cochrane databases, using the key Cancer words SG muscle, parapharyngeal space and oropharynx, the authors discuss the embryology, physiology, Styloglossus muscle anatomy and radiology of this muscle as well as its role in the oncologic staging surgery of SCCLO. Results: The most specific radiologic exam to evaluate the involvement of SG muscle in SCCLO is magnetic resonance imaging (MRI). According to the eigth international staging classification systems, radiologic invasion of the SG muscle, at the time of MRI, leads to reclassify as T4a many tumors considered as T1-3 at the time of clinical and/or on computerized tomography evaluation. -

Lecture 15 احمد فاضل د. the Submandibular Region
د.احمد فاضل Lecture 15 Anatomy The Submandibular Region The submandibular region lies under cover of the body of the mandible, between the mandible and the hyoid bone. It contains the following structures: • Muscles: Digastric, mylohyoid. hyoglossus. geniohyoid, genioglossus, and styloglossus. • Salivary glands: Submandibular and sublingual. • Nerves: Lingual, glossopharyngeal and hypoglossal. • Parasympathetic ganglion: Submandibular. • Blood vessels: Facial artery and vein and lingual artery and vein. • Lymph nodes: Submandibular group. MUSCLES OF THE SUBMANDIBULAR REGION Digastric Muscle The digastric muscle has a posterior belly, an intermediate tendon, and an anterior belly. • Origin and Insertion: The posterior belly arises from the medial surface of the mastoid process of the temporal bone, passes downward and forward across the carotid sheath, and ends in the intermediate tendon. The intermediate tendon pierces the stylohyoid insertion and is held in position by a loop of deep fascia , which binds the tendon down to the junction of the body and greater cornu of the hyoid bone. The anterior belly runs forward and medially and is attached to the lower border of the body of the mandible, near the median plane. • Nerve supply: The posterior belly is supplied by the facial nerve and the anterior belly is supplied by the nerve to the mylohyoid, which is a branch of the mandibular division of the trigeminal nerve. • Action: Depresses the mandible or elevates the hyoid bone. Stylohyoid Muscle The stylohyoid muscle is a small slip that passes along the upper border of the posterior belly of the digastric muscle. • Origin: From the styloid process of the temporal bone. • Insertion: The muscle passes downward and forward and is inserted into the junction of the body with the greater cornu of the hyoid bone. -
IV. DEFINITION of LYMPH NODE GROUPS (FIGURE 1) Level IA
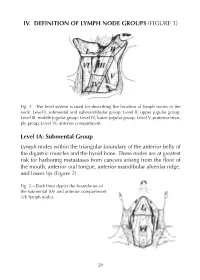
IV. DEFINITION OF LYMPH NODE GROUPS (FIGURE 1) Fig. 1—The level system is used for describing the location of lymph nodes in the neck: Level I, submental and submandibular group; Level II, upper jugular group; Level III, middle jugular group; Level IV, lower jugular group; Level V, posterior trian - gle group; Level VI, anterior compartment. Level IA: Submental Group Lymph nodes within the triangular boundary of the anterior belly of the digastric muscles and the hyoid bone. These nodes are at greatest risk for harboring metastases from cancers arising from the floor of the mouth, anterior oral tongue, anterior mandibular alveolar ridge, and lower lip (Figure 2). Fig. 2—Dark lines depict the boundaries of the submental (IA) and anterior compartment (VI) lymph nodes. 29 Level IB: Submandibular Group Lymph nodes within the boundaries of the anterior and posterior bel - lies of the digastric muscles, the stylohyoid muscle, and the body of the mandible. Radiographically, the vertical plane at the posterior aspect of the submandibular gland forms a use means of demarcat - ing the posterior aspect of Level IB from IIA.The group includes the pre- and postglandular nodes, and the pre- and postvascular nodes. The submandibular gland is included in the specimen when the lymph nodes within this triangle are removed. These nodes are at greatest risk for harboring metastases from the cancers arising from the oral cavity, anterior nasal cavity, soft tissue structures of the mid - face, and submandibular gland (Figure 3). Fig. 3—The boundaries dividing levels I, II, and V into sublevels A and B. -

The 12 Cranial Nerves
The 12 Cranial Nerves Nerve # Name Function 1st Olfactory Relays smell 2nd Optic Transmits visual information 3rd Oculomotor External muscles of the eye 4th Trochlear Also supplies muscles of the eye 5th Trigeminal Chewing and sensation in the face 6th Abducent Controls lateral eye movement 7th Facial Muscles of facial expression, taste buds, sensation in fingers and toes, blinking 8th Auditory Hearing and balance 9th Glossopharyngeal Sensation, taste and swallowing 10th Vagus Organs in chest and abdomen 11th Accessory Supplies two neck muscles, the sternomastoid and trapezius 12th Hypoglossal Muscles of the tongue and neck The 12 Cranial Nerves—Detail Cranial Nerve 1 Sensory nerve – Olfactory Nerve – controls sense of smell Cranial Nerve 2 Sensory nerve- Optic Nerve- controls vision by sending information from retina Cranial Nerve 3 Motor nerve- Oculomotor Nerve-Controls most eye muscles. Works closely with Cranial Nerves 4 & 6. Controls eye movement, pupil dilation, and pupillary constriction. It also controls the muscles that elevate the upper eyelids. Cranial Nerve 4 Motor nerve- Trochlear Nerve- Controls the downward and outward movement of the eye. Works closely with Cranial Nerves 3 & 6. Can cause vertical Diplopia (double vision). Weakness of downward gaze can cause difficulty in descending stairs. Cranial Nerve 5 Motor and sensory nerve-Trigeminal Nerve-Carries sensory information from most of the head, neck, sinuses, and face. Also carries sensory information for ear and tympanic membrane. Provides motor supply to the muscles of masticulation (chewing), and to some of the muscles on the floor of the mouth. Also provides motor supply to tensor tympani (small muscle in the middle ear which tenses to protect the eardrum). -

Anatomy of Larynx the Larynx Situated in the Midline Ofthe Neck Opposite to the 3Rd - 6Th Cervical Vertebrae
د.علي عبداﻷمير جوادL 1 LARYNGOLOGY Anatomy of Larynx The larynx Situated in the midline ofthe neck opposite to the 3rd - 6th cervical vertebrae. It consists of framework of cartilages connected by ligaments & membranes. It is lined by a mucous membrane surrounded by muscles. Laryngeal cartilages: Form the main framework of the larynx & divided into: 1. unpaired cartilages: three in number: a. Thyroid cartilage: is the largest one & consists of 2parts, each one is called thyroid ala or lamina (square-shaped). The 2 alae meet in the midline forming an angle of about 90in men& about 120 in women,thusthe junction is more prominent in me n ( Ada m's Apple). The thyroid cartilage articulates inferiorly with the cricoid cartilage. b. cricoid cartilage: signet-shaped & it is the only complete ring in the respiratory tract. It consists of anarch anteriorly & lamina posteriorly, The lamina articulates superiorly with the arytenioids cartilage, while the junction between the arch & the lamina of cricoid is the site of articulation with the thyroid cartilage superiorly also. c. Epiglottis: rise up behind the tongue,it is a thin leaf like sheet of elastic fibrocartilage. It has free upper part & a thin long stem inferiorly attached to the inner surface of the thyroid alae at their junction. 2. Paired cartilages (Rt & Lt): also three in number: a. Arytenoid cartilages: pyramidal in shape, articulate with the superior surface of the cricoid lamina. It has a muscular process (to which 1 muscles of the larynx attach), & a vocal process (to which the vocal cords attach). Superiorly the arytenoids cartilage articulates with the corniculate cartilage. -

Dissection of the Speech Production Mechanism by the UCLA Phonetics Laboratory Editors: Melissa Epstein, Narineh Hacopian and Pe
Dissection of the Speech Production Mechanism by The UCLA Phonetics Laboratory Editors: Melissa Epstein, Narineh Hacopian and Peter Ladefoged Illustrations by Siri Tuttle UCLA Working Papers in Phonetics 102 2002 Dissection of the Speech Production Mechanism Preface Introduction i 1.The Respiratory Mechanism 1 2.The Lips 11 3.The Jaw and Related Structures 15 4.The Neck 21 5.The Brain and the Cranial Nerves 27 6.The Pharynx 39 7.The Tongue 45 8. The Larynx 53 9.The Velum 61 Appendix A: Glossary of Anatomical Terms 63 Appendix B: Muscles of the Speech Production Mechanism 67 Appendix C: Annotated Bibliography 81 Preface One can have all the knowledge available from anatomical atlases and from textbooks on speech production, but none of it substitutes for the hands-on experience acquired in an anatomy laboratory. There is nothing comparable with actually seeing where the muscles of the tongue attach, feeling the comparative thickness of different muscles, moving the arytenoid cartilages to stretch the vocal folds, and holding a brain in one’s hand. The aim of this manual is to suggest ways of dissecting the human vocal apparatus that are appropriate for students of speech. It is designed as a short course that could be part of another, more classroom oriented, course. We hope we can encourage people working in speech pathology, phonetics, and communication sciences to find a co-operative medical department and try dis- secting a human cadaver for themselves. Anatomy departments are often able to help, but we have found that a better solution is to contact people in Head and Neck Surgery, who are much more knowledgeable about the anatomy of the areas of interest to students of speech. -

Discovery of a Novel Variant of the Stylochondrohyoideus Muscle
eISSN 1308-4038 International Journal of Anatomical Variations (2010) 3: 197–199 Case Report Discovery of a novel variant of the stylochondrohyoideus muscle Published online December 14th, 2010 © http://www.ijav.org H. Wayne LAMBERT [1,2] ABSTRACT [1,2] Stavros ATSAS During routine dissection of the suprahyoid region, a duplicate stylohyoid muscle was found in a 65-year- Taylor A. DAYTON [1,3] old Caucasian female. This variant muscle arose from the base of the styloid process before proceeding to envelope and insert upon the stylohyoid ligament. While other authors have reported the presence of a stylochondrohyoideus muscle which replaced the stylohyoid ligament or inserted into the stylohyoid ligament distally, this case study presents the first reported finding of a muscle completely enveloping the stylohyoid ligament proximally and then inserting directly into the ligament itself. Due to its association with the Department of Neurobiology and Anatomy, West Virginia University School of Medicine, stylohyoid ligament, this muscle is being classified as a new variant of the stylochondrohyoideus muscle. This Robert C. Byrd Health Sciences Center, Morgantown, West Virginia [1], Department of paper also attempts to resolve the nomenclature discrepancies associated with duplicate stylohyoid muscles. © Anatomical Sciences and Neurobiology, University of Louisville Health Sciences Center, IJAV. 2010; 3: 197–199. Louisville, Kentucky [2], Department of Biochemistry, Virginia Polytechnic Institute and State University, Blacksburg, Virginia [3], USA. Dr. H. Wayne Lambert, PhD Associate Professor West Virginia University School of Medicine Robert C. Byrd Health Sciences Center Department of Neurobiology and Anatomy HSN 4052; P.O. Box 9128 Morgantown, 26506-9128, WV, USA.