Amit Singh* Raj Kumar Naresh P Singh Ramakant Rawat Amit Singh
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
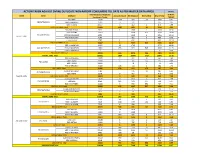
Action Taken Against Dvvnl Duplicate Non-Rapdrp Consumers Till Date As Per Master Data Apr20 in Nos
ACTION TAKEN AGAINST DVVNL DUPLICATE NON-RAPDRP CONSUMERS TILL DATE AS PER MASTER DATA APR20 IN NOS. Total Suspected Duplicate % W.R.T. ZONE Circle DivName Account Closed Bill Stopped Dismantled Grand Total Consumers Target TARGET EDD-BAH 17047 1116 289 28 1433 8.41 EDCFATEHABAD EDD-ETMADPUR 10405 75 232 307 2.95 EDD-III AGRA 23657 6 462 2 470 1.99 EDCFATEHABAD Total 51109 1197 983 30 2210 4.32 EDD-FIROZABAD 9032 1 1566 1 1568 17.36 EDD-JASRANA 14167 3408 826 4234 29.89 EDC-FIROZABAD EDD-SHIKOHABAD 6292 1449 6 1455 23.12 AGRA 1 ZONE EDD-SHIRSAGANJ 7149 482 3 485 6.78 S EDD-TUNDLA 4787 1 632 1 634 13.24 EDC-FIROZABAD Total 41427 2 7537 837 8376 20.22 EDD-II MAINPURI 16327 32 1745 1777 10.88 EDC-MAINPURI EDD-III MAINPURI 13681 433 629 546 1608 11.75 EUDD-1 MAINPURI 7 0 0.00 EDC-MAINPURI Total 30015 465 2374 546 3385 11.28 AGRA 1 ZONE Total 122551 1664 10894 1413 13971 11.40 EDD KHERAGARH 12877 7 322 32 361 2.80 EDD-I AGRA 27184 5 105 133 243 0.89 EDC-IAGRA EDD-II AGRA 24091 78 1 79 0.33 EDD-IV KIRAWALI 15183 146 114 4 264 1.74 EDC-IAGRA Total 79335 158 619 170 947 1.19 EDD-III MATHURA 7781 476 11 487 6.26 EDC-IIMATHURA EDD-MATH 5270 9 467 476 9.03 AGRA 2 ZONE EDC-IIMATHURA Total 13051 9 943 11 963 7.38 EDD GOVERDHAN 13014 7 613 2 622 4.78 EDCMATHURA EDD KOSI 8099 185 171 144 500 6.17 EDD-I MATHURA 10226 3 333 391 727 7.11 EDCMATHURA Total 31339 195 1117 537 1849 5.90 EUDD-II VRINDAVAN 1432 3 225 228 15.92 EUDCMATHURA EUDD-III MATHURA 453 2 4 6 1.32 EUDCMATHURA Total 1885 5 229 234 12.41 AGRA 2 ZONE Total 125610 367 2908 718 3993 3.18 EDD-I -

Drishti IAS Coaching in Delhi, Online IAS Test Series & Study Material
Drishti IAS Coaching in Delhi, Online IAS Test Series & Study Material drishtiias.com/printpdf/uttar-pradesh-gk-state-pcs-english Uttar Pradesh GK UTTAR PRADESH GK State Uttar Pradesh Capital Lucknow Formation 1 November, 1956 Area 2,40,928 sq. kms. District 75 Administrative Division 18 Population 19,98,12,341 1/20 State Symbol State State Emblem: Bird: A pall Sarus wavy, in Crane chief a (Grus bow–and– Antigone) arrow and in base two fishes 2/20 State State Animal: Tree: Barasingha Ashoka (Rucervus Duvaucelii) State State Flower: Sport: Palash Hockey Uttar Pradesh : General Introduction Reorganisation of State – 1 November, 1956 Name of State – North-West Province (From 1836) – North-West Agra and Oudh Province (From 1877) – United Provinces Agra and Oudh (From 1902) – United Provinces (From 1937) – Uttar Pradesh (From 24 January, 1950) State Capital – Agra (From 1836) – Prayagraj (From 1858) – Lucknow (partial) (From 1921) – Lucknow (completely) (From 1935) Partition of State – 9 November, 2000 [Uttaranchal (currently Uttarakhand) was formed by craving out 13 districts of Uttar Pradesh. Districts of Uttar Pradesh in the National Capital Region (NCR) – 8 (Meerut, Ghaziabad, Gautam Budh Nagar, Bulandshahr, Hapur, Baghpat, Muzaffarnagar, Shamli) Such Chief Ministers of Uttar Pradesh, who got the distinction of being the Prime Minister of India – Chaudhary Charan Singh and Vishwanath Pratap Singh Such Speaker of Uttar Pradesh Legislative Assembly, who also became Chief Minister – Shri Banarsidas and Shripati Mishra Speaker of the 17th Legislative -

District Census Handbook, Mainpuri, Part-XII-A, Series-25, Uttar Pradesh
CENSUS199~ ~~C11-25 SERIES-25 UTTAR PRADESH ~-XII3i J» ART -XIIA "IDB q ~:Plx VILLAGE & TOWN A~~IC151 DIRECTORY "Mc1r iJFP I 0 IrJ I gtfl gffii q) I DISTRICT CENSUS HANDBOOK '~~ DISTRICT MAINPURI Pl~~I(f) ISl'iJIOI'i1 cnRf DIRECTOR OF CENSUS OPERATIONS \3ITR ~ UTTARPRADES:___j Wr:r~ ~~ 1. ~ 2. mcfC!i~ v 3. fum CIiT ~ IX 4. furB*~~ 5. ltrffi \iRlfURT ~furclir CIiT ~ ~ XV 6 3TTWf (i) ~ ~ 1JIl1 ~ 1 ftlj~If£lCb ~ ~- RIm 2 2 ftlj~If£lCb ~ ~-~ 12 3 ftlj~If£lCb ~ ~-~ 26 4 ftlj~If£lCb ~ ~-~ 36 5 ftlj~If£lCb ~ ~-~ 48 6 ftlj~If£lCb ~ ~ ~i:'fl1111';l1 62 7 ftlj~lf£I(j) ~ ~-ffi 76 8 ftlj~lf£I(j) ~ ~-m 96 9. ftlj~If£lCb ~ ~-f$'A 104 10. CA''l.1l11 J!- (ii) lJTI11 ~ ~ ~ 1 ftlj~If£lCb ~ ~- RIm 116 2 ftlj~If£lCb ~ ~-~ 120 3 ftlj<If£lCb ~ ~-~ 125 4 ~ilj<If£lCb ~ ~-~ 129 5 fllj<If£lCb ~ ~-~ 133. 6 ~iljGIf£lCf) ~ ~ ~i:'flH11';l1 138 7 XiI:i~lfZlC/l m ~-tcR 143 8 XiI:i~lfZlC/l m ~-m 150 9. XiI:i~lfZlC/l m ~-~ 153 qR~lffc41 XiI5~lfZlC/l m ~ erR rom, ~ om 3RT ~ 158 II \iR1TUAT ~ ~ m, 11A <n) 11Tit, \if11TURT 11Tit C!iT ~ _ N.f.Tt ~ 164 ][] ~ C!iT $ CIiX WM ~ m q\l ~ (XiI:i~lfZlC/l fcICIlrn ~) 165 IV ~ _ om ~ ,JFi\J1IRt<11 q\l ~"C/lT <gc1 ~ ~. ~ * 166 ~mq\l~ 8. ~-IIW~ I mfuITff 3tR ~ ~ 183 I1 -;pffi q\lg 'far -qq' ftqfu, 1989 184 ][] ;PI~qlfBC/l1 fc)m, 1988-89 185 IV ~3tR~~, 1989 186 IV 3l-~"IfftR qfum'f # ~ -qq' 3RT~, 1989 187 V ~,~,~3tR~~,1989 188 VI ~,~, m 3tR ~, 1989 190 ~ -;pffi q\l ~ om ~ ~ 191 CONTENTS Page No. -

Investigation of Wild Species in Yamuna - Chambal
International Journal of Fauna and Biological Studies 2015; 2(6): 08-13 ISSN 2347-2677 IJFBS 2015; 2(6): 08-13 Investigation of wild species in Yamuna - Chambal Received: 09-09-2015 forest, in Etawah - Auraiya (UP) India Accepted: 11-10-2015 CP Singh Department of Zoology Janta CP Singh, Dr Yogesh Dixit, Dr RRS Chauhan, SB Mishra Mahavidyalaya Ajitmal Auraiya (U. P) India. Abstract A detailed exploration of Yamuna –Chambal forest was carried out between Udi to Pachnada in March Dr. Yogesh Dixit 2012 to Sep 2014. The entire study area is covering about 3000 Sq. km from Udi to Pachnada. The Department of Zoology Janta riverine study stretch of Chambal and Yamuna was surveyed by row boat, motor boat and the forests Mahavidyalaya Ajitmal Auraiya stretch surveyed on foot and on motor cycle for documented important land marks and various activities. (U. P) India. Occasionally information gathered from local people and forest department staff members. The general Dr. RRS Chauhan achievements were- Department of Zoology Janta Riverine Achievments Mahavidyalaya Ajitmal Auraiya Chambal is unpolluted river. (U. P) India. At Bhareh confluence (Chambal with Yamuna) water was found less polluted due to mixing of Yamuna water. SB Mishra Avian fauna was satisfactory. National Chambal Sanctuary UP Gharial population is higher than mugger. India. Dolphin population is high at Herpura. Hard shell turtle high but soft shell turtle is less. Deforestation and fishing is main anti conservation. River bank condition is much concern. Annelids, Molluscs and Arthropods were noticed as main Invertebrates. Forest Achievments 1. More than 350 species of forest vegetations have been presented. -

Section-VIII : Laboratory Services
Section‐VIII Laboratory Services 8. Laboratory Services 8.1 Haemoglobin Test ‐ State level As can be seen from the graph, hemoglobin test is being carried out at almost every FRU studied However, 10 percent medical colleges do not provide the basic Hb test. Division wise‐ As the graph shows, 96 percent of the FRUs on an average are offering this service, with as many as 13 divisions having 100 percent FRUs contacted providing basic Hb test. Hemoglobin test is not available at District Women Hospital (Mau), District Women Hospital (Budaun), CHC Partawal (Maharajganj), CHC Kasia (Kushinagar), CHC Ghatampur (Kanpur Nagar) and CHC Dewa (Barabanki). 132 8.2 CBC Test ‐ State level Complete Blood Count (CBC) test is being offered at very few FRUs. While none of the sub‐divisional hospitals are having this facility, only 25 percent of the BMCs, 42 percent of the CHCs and less than half of the DWHs contacted are offering this facility. Division wise‐ As per the graph above, only 46 percent of the 206 FRUs studied across the state are offering CBC (Complete Blood Count) test service. None of the FRUs in Jhansi division is having this service. While 29 percent of the health facilities in Moradabad division are offering this service, most others are only a shade better. Mirzapur (83%) followed by Gorakhpur (73%) are having maximum FRUs with this facility. CBC test is not available at Veerangna Jhalkaribai Mahila Hosp Lucknow (Lucknow), Sub Divisional Hospital Sikandrabad, Bullandshahar, M.K.R. HOSPITAL (Kanpur Nagar), LBS Combined Hosp (Varanasi), -

ORIGINAL ARTICLE Pissn 0976 3325│Eissn 2229 6816 Open Access Article
ORIGINAL ARTICLE pISSN 0976 3325│eISSN 2229 6816 Open Access Article www.njcmindia.org ASSESSMENT OF MAGNITUDE AND THE CO-MORBIDITIES OF OVERWEIGHT AND OBESITY IN URBAN AND RURAL AREAS OF KANPUR Naresh Pal Singh1, Pankaj K Jain2, R P Sharma3, Suresh Chandra4, Seema Nigam4, Anamika Singh5 Financial Support: None declared Conflict of interest: None declared ABSTRACT Copy right: The Journal retains the copyrights of this article. However, reproduction of this article in the Background: Obesity is emerging as a global epidemic with part or total in any form is permis- growing threat to health in both developed and developing coun- sible with due acknowledgement of tries. It has become a major health concern for almost all the age the source. groups of the society. Objectives of the study is assess the preva- How to cite this article: lence and co-morbidities of overweight and obesity among per- Singh NP, Jain PK, Sharma RP, sons 15 years and above in urban and rural areas of Kanpur, UP. Chandra S, Nigam S, Singh A. As- Methods: For this cross-sectional study, multistage random sam- sessment of Magnitude and the Co- pling technique was used to select one colony in urban and one morbidities of Overweight and Obesity in Urban and Rural areas of village in rural area of Kanpur district. The desired sample size Kanpur. Natl J Community Med. was 2200. Detailed socio-demographic information was collected 2015; 6(1):1-5. on a pre-designed and pre-tested questionnaire. After anthropo- metric examination, Body Mass Index (BMI) was used to assess Author’s Affiliation: the overweight and obesity status. -

Name of Officers at Zones and Their Estate Management Offices S.No
Name of officers at Zones and their Estate Management Offices S.No. Zone & Zonal Officer Office Name of Officer Designation Contact Details Landline Mobile 1 Lucknow Zone EMO office Indira Nagar,Lucknow Sri Ambuj Rastogi Estate Manager 0522-2355280 8795811608 Dr. Anil Kumar EMO Office Vikas Nagar,Lucknow Sri Ambuj Rastogi Estate Manager 0522-2769137 8795811608 Deputy Housing Commissioner EMO Office Rajajipuram,Lucknow Sri S.N.Pathak Estate Manager 0522-2418414 8795810794 Mobile : 8795810018 EMO Office Vrindavan Yojna,Lucknow Sri K.D.Sharma Estate Manager 0522-2443531 8795811111 EMO Office Rae Bareilly Sri K.D.Sharma Estate Manager 0522-2443531 8795811111 EMO Office Sitapur Sri Ambuj Rastogi Estate Manager 0522-2769137 8795811608 EMO Office Lakhimpur Sri Ambuj Rastogi Estate Manager 0522-2769137 8795811608 EMO Office Hardoi/Shahabad Sri Ambuj Rastogi Estate Manager 0522-2769137 8795811608 EMO Office Amrapali Yojna, Lucknow Sri Hari Mohan Estate Manager 0522-6561042 7705002895 EMO office Avadh Vihar Yojna, Office Complex 1st Floor, Sector-9, Sri Nripendra Bahadur Singh Estate Manager 0522-2355280 8795811528 Vrindavan Yojna,Lucknow-226029/Diamond Dairy/Unnao 2 Meerut Zone EMO office, Meerut/Hapur Sri Subhash Maurya Estate Manager 0121-2762011 8795811050 Ms. Sherry EMO office, Vasundhara-Ghaziabad Sri Hetam Pal Singh Astt Housing Commissioner 0120-2882025 8795811049 Deputy Housing Commissioner EMO office, Mandola Vihar-Ghaziabad Sri Hetam Pal Singh Astt Housing Commissioner - 8795811049 Phone/Fax: (0121)-2760415 EMO office, Saharanpur/Muzzaffarnagar/Khatauli -

District Ground Water Brochure of Auraiya District, U.P
DISTRICT GROUND WATER BROCHURE OF AURAIYA DISTRICT, U.P. By Dr. B.C. Joshi Scientist 'B' CONTENTS Chapter Title Page No. AURAIYA DISTRICT AT A GLANCE ..................2 1.0 INTRODUCTION ..................5 2.0 RAINFALL & CLIMATE ..................6 3.0 GEOMORPHOLOGY & SOIL TYPES ..................7 4.0 GROUND WATER SCENARIO ..................8 5.0 GROUND WATER MANAGEMENT STRATEGY ..................12 6.0 GROUND WATER RELATED ISSUES AND PROBLEMS ..................12 7.0 AWARENESS & TRAINING ACTIVITY ..................13 8.0 AREA NOTIFIED BY CGWA / SGWA ..................13 9.0 RECOMMENDATIONS ..................14 PLATES: I. LOCATION MAP OF AURAIYA DISTRICT, U.P. II. GEOMORPHOLOGICAL MAP, AURAIYA DISTRICT, U.P. III. HYDROGEOLOGICAL MAP, AURAIYA DISTRICT, U.P. IV. DEPTH TO WATER MAP (PREMONSOON), AURAIYA DISTRICT, U.P. V. DEPTH TO WATER MAP (POSTMONSOON), AURAIYA DISTRICT, U.P. VI. CATEGORIZATION OF BLOCKS, AURAIYA DISTRICT, U.P. DISTRICT AT A GLANCE (AURAIYA) 1. GENERAL INFORMATION i. Geographical Area (Sq. Km.) : 2015 ii. Administrative Divisions (as on 31.3.2005) Number of Tehsil / Block : 2/7 Number of Panchayats /Villages : -/841 iii. Population (As on 2001 census) : 1179993 iv. Average Annual Rainfall (mm) : 807.35 2. GEOMORPHOLOGY Major physiograpic units : Ganga-Yamuna Doab sub divided in Lowland area (Active & Old flood plain) and Upland area (Varanasi & Banda alluvial plain) Major Drainages : Yamuna, Chambal, Sengar, & Rind rivers. 3. LAND USE (Sq. Km.) a) Forest area : 102.83 b) Net area sown : 1438.82 c) Cultivable area : 1667.15 4. MAJOR SOIL TYPES : Sandy loam and clay, locally classified as Bhur, Matiyar, Dumat and Pilia. 5. AREA UNDER PRINCIPAL CROPS (As on 2005-06) : 1342.03 6. -

Head, Department of Neurosurgery
1 Full Bio-data in 106 Pages PROF. (DR.) RAJ KUMAR Head, Department of Neurosurgery Co-chairman, United Nation Affair (World Kabaddi Federation) Sanjay Gandhi Post Graduate Institute of Medical Sciences Raebareli Road, Lucknow Ex-In charge Apex Trauma Centre, SGPGIMS Ex-Vice Chancellor Uttar Pradesh University of Medical Sciences, Saifai, Etawah Ex-Director All India Institute of Medical Sciences Rishikesh, Uttarakhand, India 2021 2 DR. RAJ KUMAR B.Sc., M.B.B.S., M.S., M.Ch., Ph.D., M.R.C.S., F.R.C.S., F.A.M.S., F.N.S., M.A.M.S, M.N.A.Sc., F.A.S.E.T, D.Sc. Profile __________________________________________________________________________ Personal Details: OFFICIAL ADDRESS : HOD, Department of Neurosurgery Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow (UP)-226014, India Contact Numbers : 0522-249-4735,0522-249-4771 Email : [email protected] PERMANENT ADDRESS : A/82, Omaxe city, Saheed Path, Opposite Ramabai Chauki & Ambedkar University, Lucknow, Uttar Pradesh, India-226025 E-mail : [email protected], Website : www.profrajkumar.com PERSONAL INFORMATION Father’s Name : Late Sri Chhote Lal Date of Birth : 15th December, 1959 Place of Birth : Village- Paman, Kanpur (Dehat), UP, India Nationality : Indian Marital Status : Married 3 OBJECTIVES As Professor: 1. To achieve excellence in medical and super speciality of Neurosurgery. 2. To render quality medical training, medical research & quality patient care. 3. To enhance reputation of country by relevant research in medical field of Neurosciences. 4. To develop centers of excellence in medical field. 5. Social awareness in young doctors and bright minds for developing International standard of patient care and health care system. -
District Census Handbook, Auraiya, Part-XII-A & B, Series-10, Uttar
CENSUS OF INDIA 2001 ~3ERIES-10 UTTAR PRADeSH DISTRICT CENSUS HANDBOOK Part - A & B AURAIYA VILLAGE & TOWN DIRECTORY VILLAGE AND TOWNWISE PRIMARY CENSUS ABSTRACT {_ -~. I ( ! ) I F·~ ~ ~ _~. ~: ~ i I'i (\I'i!. (11(11 NIIII Dlr~ECTORATE OF Cf-':l\ISUS OPERATIONS, UTTAR PF~!\DESH LUCKNOW UTTAR PRADESH DISTRICT AURAIY A KILOMETRES , ,. 5 5 10 15 20 25 N A Area(sq.km.) . 2,015 (:::, Pepu) a tion .. ... 1,1'79,993 Number of Tahsils .. Number of Vikas Khand. ... ~ I· Number of Towns. Q; Number of Villages .. ·•• sj A L A DISTRICT AURAIYA-i S - PART OF VIKAS KHAND SAHAR (NEWL Y CREATED) CHANGE IN JURISDICTION 1991 - 2001 KILOMET~ :'".~~ '.~ . BOUNDARY DISTRICT -----: ! TAHSIL VIKAS KHAND .~ HEADQUARTERS DISTRICT, TAHSIL VIKAS KHAND @ @ NATJONAL HIGHWAY NH 2 STATE HIGHWAY SH 21 IMPORTANT METALLED ROAD RAILWAY LINE BROAD GAUGE. RIVER AND STREAM VILLAGE HAVING 5000 AND ABOVE POPULATJON WITH NAME • Kasba Khanpur TOWNS WITH POPULATION SIZE AND CLASS II JIl , IV , V ~.~.-.~" . DEGREE COLLEGE ~ AREA GAINED- FROM ~ DISTRICT ETAWAH MOTIF JAMUNAPARI GOATS The main centre of availability of Jamunapari Goats is considered in the surroundings of the village Pachnada in the district Auraiya at the banks of the rivers Yamuna, Chambal, Kunwari, Rind and Pahunj. Though these goats are extended from Chakarnagar to the either of the banks of river Yamuna, their height is much more than other goats with the backbone lying downwards likewise came and having two long ears in addition to two amazing short ears below their necks. There is a variety of species which are bit different from each other, but among them ~Alwari goats' are the best one, which give about 3 to4 kg. -

Notice for Appointment of Regular/Rural Retail Outlets Dealerships
Notice for appointment of Regular/Rural Retail Outlets Dealerships Hindustan Petroleum Corporation Limited proposes to appoint Retail Outlet dealers in the State of Uttar Pradesh, as per following details: Fixed Fee Minimum Dimension (in / Min bid Security Estimated Type of Finance to be arranged by the Mode of amount ( Deposit ( Sl. No. Name Of Location Revenue District Type of RO M.)/Area of the site (in Sq. Site* applicant (Rs in Lakhs) selection monthly Sales Category M.). * Rs in Rs in Potential # Lakhs) Lakhs) 1 2 3 4 5 6 7 8 9a 9b 10 11 12 SC/SC CC 1/SC PH/ST/ST CC Estimated Estimated fund 1/ST working required for PH/OBC/OBC CC/DC/ capital Draw of Regular/Rural MS+HSD in Kls Frontage Depth Area development of CC 1/OBC CFS requirement Lots/Bidding infrastructure at PH/OPEN/OPE for operation RO N CC 1/OPEN of RO CC 2/OPEN PH ON LHS, BETWEEN KM STONE NO. 0 TO 8 ON 1 NH-AB(AGRA BYPASS) WHILE GOING FROM AGRA REGULAR 150 SC CFS 40 45 1800 0 0 Draw of Lots 0 3 MATHURA TO GWALIOR UPTO 3 KM FROM INTERSECTION OF SHASTRIPURAM- VAYUVIHAR ROAD & AGRA 2 AGRA REGULAR 150 SC CFS 20 20 400 0 0 Draw of Lots 0 3 BHARATPUR ROAD ON VAYU VIHAR ROAD TOWARDS SHASTRIPURAM ON LHS ,BETWEEN KM STONE NO 136 TO 141, 3 ALIGARH REGULAR 150 SC CFS 40 45 1800 0 0 Draw of Lots 0 3 ON BULANDSHAHR-ETAH ROAD (NH-91) WITHIN 6 KM FROM DIBAI DORAHA TOWARDS 4 NARORA ON ALIGARH-MORADABAD ROAD BULANDSHAHR REGULAR 150 SC CFS 40 45 1800 0 0 Draw of Lots 0 3 (NH 509) WITHIN MUNICIAPL LIMITS OF BADAUN CITY 5 BUDAUN REGULAR 120 SC CFS 30 30 900 0 0 Draw of Lots 0 3 ON BAREILLY -

Kanpur Dehat District, U.P
DISTRICT GROUND WATER BROCHURE KANPUR DEHAT DISTRICT, U.P. (AAP: 2012-13) By P.K. Tripathi Scientist 'C' CONTENTS Chapter Title Page No. KANPUR DEHAT DISTRICT AT A GLANCE ..................3 1.0 INTRODUCTION ..................6 2.0 RAINFALL & CLIMATE ..................7 3.0 GEOMORPHOLOGY & SOIL TYPE ..................7 4.0 GROUND WATER SCENARIO ..................8 4.1 Hydrogeology 4.2 Ground Water Resource 4.3 Ground Water Quality 4.4 Status of Ground Water Development 5.0 GROUND WATER MANAGEMENT STRATEGY ..................14 5.1 Ground Water Development 5.2 Water Conservation Structure & Artificial Recharge 6.0 GROUND WATER RELATED ISSUES AND PROBLEMS ..................15 7.0 RECOMMENDATIONS ..................16 PLATES: I. INDEX MAP OF KANPUR DEHAT DISTRICT, U.P. II. HYDROGEOMORPHOLOGICAL MAP OF KANPUR DEHAT DISTRICT, U.P. III. CANAL'S MAP OF KANPUR DEHAT, U.P. IV. FENCE DIAGRAM KANPUR DEHAT, U.P. V. DEPTH TO WATER LEVEL PREMONSOON 2012, KANPUR DEHAT DISTRICT, U.P. VI. DEPTH TO WATER LEVEL POSTMONSOON 2012, KANPUR DEHAT DISTRICT, U.P. VII. CATEGORIZATION OF BLOCKS (GROUND WATER RESOURCES /DRAFT), KANPUR DEHAT DISTRICT, U.P. VIII. ISOCON MAP AND POINT VALUES OF ARSENIC (PHREATIC AQUIFER), KANPUR DEHAT DISTRICT, U.P. APPENDIX: I. DETAILS OF EXPLORATORY TUBEWELLS IN KANPUR DEHAT DISTRICT, U.P. 2 KANPUR DEHAT DISTRICT AT GLANCE 1. GENERAL INFORMATION i. Geographical Area (Sq km.) : 3021 ii. Administrative Divisions : Number of Tehsil/Block 5/10 Number of Panchayat/Villages 102/1032 iii. Population (as on 2001 census) : 15,63,336 iv. Average Annual Rainfall (mm) : 782.8 2. GEOMORPHOLOGY Major Physiographic Units : Older Alluvium plain, older flood plain & active flood plain Major Drainages : Yamuna, Pandu, Rind, Sengar 3.