ORIGINAL ARTICLE Pissn 0976 3325│Eissn 2229 6816 Open Access Article
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

River Ganga at a Glance: Identification of Issues and Priority Actions for Restoration Report Code: 001 GBP IIT GEN DAT 01 Ver 1 Dec 2010
Report Code: 001_GBP_IIT_GEN_DAT_01_Ver 1_Dec 2010 River Ganga at a Glance: Identification of Issues and Priority Actions for Restoration Report Code: 001_GBP_IIT_GEN_DAT_01_Ver 1_Dec 2010 Preface In exercise of the powers conferred by sub‐sections (1) and (3) of Section 3 of the Environment (Protection) Act, 1986 (29 of 1986), the Central Government has constituted National Ganga River Basin Authority (NGRBA) as a planning, financing, monitoring and coordinating authority for strengthening the collective efforts of the Central and State Government for effective abatement of pollution and conservation of the river Ganga. One of the important functions of the NGRBA is to prepare and implement a Ganga River Basin: Environment Management Plan (GRB EMP). A Consortium of 7 Indian Institute of Technology (IIT) has been given the responsibility of preparing Ganga River Basin: Environment Management Plan (GRB EMP) by the Ministry of Environment and Forests (MoEF), GOI, New Delhi. Memorandum of Agreement (MoA) has been signed between 7 IITs (Bombay, Delhi, Guwahati, Kanpur, Kharagpur, Madras and Roorkee) and MoEF for this purpose on July 6, 2010. This report is one of the many reports prepared by IITs to describe the strategy, information, methodology, analysis and suggestions and recommendations in developing Ganga River Basin: Environment Management Plan (GRB EMP). The overall Frame Work for documentation of GRB EMP and Indexing of Reports is presented on the inside cover page. There are two aspects to the development of GRB EMP. Dedicated people spent hours discussing concerns, issues and potential solutions to problems. This dedication leads to the preparation of reports that hope to articulate the outcome of the dialog in a way that is useful. -

Kanpur Dehat
State: Uttar Pradesh Agriculture Contingency Plan for District: Kanpur Dehat 1.0 District Agriculture profile 1.1 Agro-Climatic/ Ecological Zone Agro-Ecological Sub Region(ICAR) Central Plain Zone Agro-Climatic Zone (Planning Commission) Upper Gangetic Plain Region Agro-Climatic Zone (NARP) UP-4 Central Plain Zone List all the districts falling the NARP Zone* (^ 50% area falling in the Lakhimpur Kheri, Sitapur, Hardoi, Farrukhabad, Etawah, Kanpur, Kanpur zone) Dehat, Unnao, Lucknow, Rae Bareilly, Fatehpur and Allahabad. Geographical coordinates of district headquarters Latitude Longitude Altitude(mt) 26.28 N 80.20 E Name and address of the concerned ZRS/ZARS/RARS/RRS/RRTTS Mention the KVK located in the district with address Krishi Vigyan Kendra, Zonal Agricultural Research Station, Daleep Nagar, Kanpur Dehat Name and address of the nearest Agromet Field Unit(AMFU,IMD)for CSA Kanpur agro advisories in the Zone 1.2 Rainfall Normal RF (mm) Normal Rainy Normal Onset Normal Cessation Days (Number) (Specify week and month) (Specify week and month) SW monsoon (June-sep) 713.1 45 3nd week of June 4th week of September Post monsoon (Oct-Dec) 38.1 10 Winter (Jan-March) 37.1 10 - - Pre monsoon (Apr-May) 13.2 2 - - Annual 801.5 67 - - 1.3 Land use pattern Geographical Cultivable Forest Land under Permanent Cultivable Land Barren and Current Other of the district area area area non- pastures wasteland under uncultivable fallows fallows (Latest agricultural Misc.tree land statistics) use crops and groves Area in (000 ha) 315.0 262.8 5.8 29.8 0.4 4.3 2.7 16.2 21.5 12.4 1.4 Major Soils Area(‘000 ha) Percent(%) of total Deep, fine soils moderately saline and sodic 71.0 27 % Deep, loamy soils 55.2 21 % Deep, loamy soils associated with sandy soils 79.1 30 % and eroded 1.5 Agricultural land use Area(‘000 ha) Cropping intensity (%) Net sown area 221.9 132.2 % Area sown more than once 71.5 Gross cropped area 293.4 1.6 Irrigation Area(‘000 ha) Net irrigation area 155.8 Gross irrigated area 201.0 Rain fed area 66.1 Sources of irrigation (gross irr. -
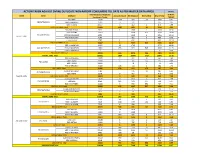
Action Taken Against Dvvnl Duplicate Non-Rapdrp Consumers Till Date As Per Master Data Apr20 in Nos
ACTION TAKEN AGAINST DVVNL DUPLICATE NON-RAPDRP CONSUMERS TILL DATE AS PER MASTER DATA APR20 IN NOS. Total Suspected Duplicate % W.R.T. ZONE Circle DivName Account Closed Bill Stopped Dismantled Grand Total Consumers Target TARGET EDD-BAH 17047 1116 289 28 1433 8.41 EDCFATEHABAD EDD-ETMADPUR 10405 75 232 307 2.95 EDD-III AGRA 23657 6 462 2 470 1.99 EDCFATEHABAD Total 51109 1197 983 30 2210 4.32 EDD-FIROZABAD 9032 1 1566 1 1568 17.36 EDD-JASRANA 14167 3408 826 4234 29.89 EDC-FIROZABAD EDD-SHIKOHABAD 6292 1449 6 1455 23.12 AGRA 1 ZONE EDD-SHIRSAGANJ 7149 482 3 485 6.78 S EDD-TUNDLA 4787 1 632 1 634 13.24 EDC-FIROZABAD Total 41427 2 7537 837 8376 20.22 EDD-II MAINPURI 16327 32 1745 1777 10.88 EDC-MAINPURI EDD-III MAINPURI 13681 433 629 546 1608 11.75 EUDD-1 MAINPURI 7 0 0.00 EDC-MAINPURI Total 30015 465 2374 546 3385 11.28 AGRA 1 ZONE Total 122551 1664 10894 1413 13971 11.40 EDD KHERAGARH 12877 7 322 32 361 2.80 EDD-I AGRA 27184 5 105 133 243 0.89 EDC-IAGRA EDD-II AGRA 24091 78 1 79 0.33 EDD-IV KIRAWALI 15183 146 114 4 264 1.74 EDC-IAGRA Total 79335 158 619 170 947 1.19 EDD-III MATHURA 7781 476 11 487 6.26 EDC-IIMATHURA EDD-MATH 5270 9 467 476 9.03 AGRA 2 ZONE EDC-IIMATHURA Total 13051 9 943 11 963 7.38 EDD GOVERDHAN 13014 7 613 2 622 4.78 EDCMATHURA EDD KOSI 8099 185 171 144 500 6.17 EDD-I MATHURA 10226 3 333 391 727 7.11 EDCMATHURA Total 31339 195 1117 537 1849 5.90 EUDD-II VRINDAVAN 1432 3 225 228 15.92 EUDCMATHURA EUDD-III MATHURA 453 2 4 6 1.32 EUDCMATHURA Total 1885 5 229 234 12.41 AGRA 2 ZONE Total 125610 367 2908 718 3993 3.18 EDD-I -

Drishti IAS Coaching in Delhi, Online IAS Test Series & Study Material
Drishti IAS Coaching in Delhi, Online IAS Test Series & Study Material drishtiias.com/printpdf/uttar-pradesh-gk-state-pcs-english Uttar Pradesh GK UTTAR PRADESH GK State Uttar Pradesh Capital Lucknow Formation 1 November, 1956 Area 2,40,928 sq. kms. District 75 Administrative Division 18 Population 19,98,12,341 1/20 State Symbol State State Emblem: Bird: A pall Sarus wavy, in Crane chief a (Grus bow–and– Antigone) arrow and in base two fishes 2/20 State State Animal: Tree: Barasingha Ashoka (Rucervus Duvaucelii) State State Flower: Sport: Palash Hockey Uttar Pradesh : General Introduction Reorganisation of State – 1 November, 1956 Name of State – North-West Province (From 1836) – North-West Agra and Oudh Province (From 1877) – United Provinces Agra and Oudh (From 1902) – United Provinces (From 1937) – Uttar Pradesh (From 24 January, 1950) State Capital – Agra (From 1836) – Prayagraj (From 1858) – Lucknow (partial) (From 1921) – Lucknow (completely) (From 1935) Partition of State – 9 November, 2000 [Uttaranchal (currently Uttarakhand) was formed by craving out 13 districts of Uttar Pradesh. Districts of Uttar Pradesh in the National Capital Region (NCR) – 8 (Meerut, Ghaziabad, Gautam Budh Nagar, Bulandshahr, Hapur, Baghpat, Muzaffarnagar, Shamli) Such Chief Ministers of Uttar Pradesh, who got the distinction of being the Prime Minister of India – Chaudhary Charan Singh and Vishwanath Pratap Singh Such Speaker of Uttar Pradesh Legislative Assembly, who also became Chief Minister – Shri Banarsidas and Shripati Mishra Speaker of the 17th Legislative -

Head, Department of Neurosurgery
1 Full Bio-data in 106 Pages PROF. (DR.) RAJ KUMAR Head, Department of Neurosurgery Co-chairman, United Nation Affair (World Kabaddi Federation) Sanjay Gandhi Post Graduate Institute of Medical Sciences Raebareli Road, Lucknow Ex-In charge Apex Trauma Centre, SGPGIMS Ex-Vice Chancellor Uttar Pradesh University of Medical Sciences, Saifai, Etawah Ex-Director All India Institute of Medical Sciences Rishikesh, Uttarakhand, India 2021 2 DR. RAJ KUMAR B.Sc., M.B.B.S., M.S., M.Ch., Ph.D., M.R.C.S., F.R.C.S., F.A.M.S., F.N.S., M.A.M.S, M.N.A.Sc., F.A.S.E.T, D.Sc. Profile __________________________________________________________________________ Personal Details: OFFICIAL ADDRESS : HOD, Department of Neurosurgery Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow (UP)-226014, India Contact Numbers : 0522-249-4735,0522-249-4771 Email : [email protected] PERMANENT ADDRESS : A/82, Omaxe city, Saheed Path, Opposite Ramabai Chauki & Ambedkar University, Lucknow, Uttar Pradesh, India-226025 E-mail : [email protected], Website : www.profrajkumar.com PERSONAL INFORMATION Father’s Name : Late Sri Chhote Lal Date of Birth : 15th December, 1959 Place of Birth : Village- Paman, Kanpur (Dehat), UP, India Nationality : Indian Marital Status : Married 3 OBJECTIVES As Professor: 1. To achieve excellence in medical and super speciality of Neurosurgery. 2. To render quality medical training, medical research & quality patient care. 3. To enhance reputation of country by relevant research in medical field of Neurosciences. 4. To develop centers of excellence in medical field. 5. Social awareness in young doctors and bright minds for developing International standard of patient care and health care system. -
District Census Handbook, Auraiya, Part-XII-A & B, Series-10, Uttar
CENSUS OF INDIA 2001 ~3ERIES-10 UTTAR PRADeSH DISTRICT CENSUS HANDBOOK Part - A & B AURAIYA VILLAGE & TOWN DIRECTORY VILLAGE AND TOWNWISE PRIMARY CENSUS ABSTRACT {_ -~. I ( ! ) I F·~ ~ ~ _~. ~: ~ i I'i (\I'i!. (11(11 NIIII Dlr~ECTORATE OF Cf-':l\ISUS OPERATIONS, UTTAR PF~!\DESH LUCKNOW UTTAR PRADESH DISTRICT AURAIY A KILOMETRES , ,. 5 5 10 15 20 25 N A Area(sq.km.) . 2,015 (:::, Pepu) a tion .. ... 1,1'79,993 Number of Tahsils .. Number of Vikas Khand. ... ~ I· Number of Towns. Q; Number of Villages .. ·•• sj A L A DISTRICT AURAIYA-i S - PART OF VIKAS KHAND SAHAR (NEWL Y CREATED) CHANGE IN JURISDICTION 1991 - 2001 KILOMET~ :'".~~ '.~ . BOUNDARY DISTRICT -----: ! TAHSIL VIKAS KHAND .~ HEADQUARTERS DISTRICT, TAHSIL VIKAS KHAND @ @ NATJONAL HIGHWAY NH 2 STATE HIGHWAY SH 21 IMPORTANT METALLED ROAD RAILWAY LINE BROAD GAUGE. RIVER AND STREAM VILLAGE HAVING 5000 AND ABOVE POPULATJON WITH NAME • Kasba Khanpur TOWNS WITH POPULATION SIZE AND CLASS II JIl , IV , V ~.~.-.~" . DEGREE COLLEGE ~ AREA GAINED- FROM ~ DISTRICT ETAWAH MOTIF JAMUNAPARI GOATS The main centre of availability of Jamunapari Goats is considered in the surroundings of the village Pachnada in the district Auraiya at the banks of the rivers Yamuna, Chambal, Kunwari, Rind and Pahunj. Though these goats are extended from Chakarnagar to the either of the banks of river Yamuna, their height is much more than other goats with the backbone lying downwards likewise came and having two long ears in addition to two amazing short ears below their necks. There is a variety of species which are bit different from each other, but among them ~Alwari goats' are the best one, which give about 3 to4 kg. -

HFCL Bags Order Worth Rs.221.16 Crores for Kanpur Metro
HFCL Limited (formerly Himachal Futuristic Communications Ltd .) 8, Commercial Complex, Masjid Moth, Greater Kailash -II, mHFCLGROUP , New Delhi - 110048, India Tel : (+9111) 3520 9400, 3520 9500, Fax: (+9111) 35209525 Web : www.hfcl.com Email [email protected] HFCL/SEC/20-21 March 17, 2021 The BSE Ltd. The National Stock Exchange of India Ltd. 1st Floor, New Trading Wing, Rotunda Building Exchange Plaza, 5th Floor, C - 1, Block G Phiroze Jeejeebhoy Towers, Dalal Street, Fort Sandra- Kurla Complex, Bandra (E) Mumbai- 400001 Mumbai- 400051 [email protected] [email protected] Security Code No.: 500183 Security Code No.: HFCL RE: Intimation under Regulation 30 of SEBI (Listing Obligations and Disclosure Requirements) Regulations, 2015 (the "SEBI Listing Regulations"). Subject: HFCL bags Order worth U21.16 Crores for Kanpur Metro (Corridor-1 and Corridor-H) and Agra Metro (Corridor-I) Projects from Uttar Pradesh Metro Rail Corporation Ltd. Dear Sir(s)/ Madam, We are pleased to inform all our stakeholders that the Company has bagged an Order worth Rs.221.16 Crores from Uttar Pradesh Metro Rail Corporation Ltd., for Design, Manufacture, Supply, Installation, Testing and Commissioning of Telecommunication Systems for Kanpur Metro (Corridor-! and Corridor-II) and Agra Metro (Corridor-!) Project (the "Project") . The details as required under Regulation 30 of the SEBI Listing Regulations read with SEBI Circular No. CIR/CFD/CMD4/2015 dated 9th September, 2015 , are as under: s. Particulars Details No. a) Name of the entity awarding -

Auraiya District
lR;eso t;rs Government of India Ministry of MSME Brief Industrial Profile of Auraiya District MSME-Development Institute (Ministry of MSME, Govt. of India,) Phone: 0512-2295070-73 Fax: 0512-2240143 E-mail: [email protected] Web: msmedikanpur.gov.in FOREWORD District Industrial Potentiality Survey Report of District Auraiya is a key report which not only contains current industrial scenario of the district but also other useful information about the district. This report provides valuable inputs which may be useful for existing & prospective entrepreneurs of the District. It is the only source which provides the latest data on infrastructure, banking and industry of the district. It also provides information on potentials areas in manufacturing and service sector of the district. I sincerely hope that District Industrial Potentiality Survey Report of District Auraiya will facilitate easier dissemination of information about the district to policy makers and also to the professionals working in the MSME sector. I appreciate the efforts made by Shri Sushil Kumar Gangal, Investigator (Glass/Ceramics) in preparing the District Industrial Potentiality Survey Report of Auraiya District. June, 2016 ( U. C. Shukla ) Kanpur Director 2 CONTENTS S. No. Topic Page No. 1. General Characteristics of the District 03 1.1 Location & Geographical Area 03 1.2 Topography 03 1.3 Availability of Minerals. 04 1.4 Forest 04 1.5 Administrative set up 04 2. District at a glance 05-07 2.1 Existing Status of Industrial Area in the District Auraiya 08 3. Industrial Scenario of Auraiya 08 3.1 Industry at a Glance 09 3.2 Year Wise Trend Of Units Registered 10 3.3 Details Of Existing Micro & Small Enterprises & Artisan 10 Units in The District 3.4 Large Scale Industries / Public Sector undertakings 11 3.5 Major Exportable Item 11 3.6 Growth Trend 11 3.7 Vendorisation / Ancillarisation of the Industry 12 3.8.2 Major Exportable Item 12 3.9 Service Enterprises 12 3.9.2 Potentials areas for service industry 12 3.10 Potential for new MSMEs 12-13 4. -

Kanpur- Lucknow Expressway TERMS of REFERENCE for EIA STUDY A. INTRODUCTION
Kanpur- Lucknow Expressway TERMS OF REFERENCE FOR EIA STUDY A. INTRODUCTION: NHAI has decided to take up the Kanpur - Lucknow Expressway project to facilitate high speed travel in this corridor. The project is Consultancy Services for Preparation of DPR of Kanpur – Lucknow Expressway, have an approximate length of 75 km (the “Project”) including spurs through BOT and EPC basis. The DPR for Kanpur – Lucknow Expressway has been entrusted to Egis India Consulting Engineers Pvt. Limited by the National Highways Authority of India (NHAI). The contract for expressway comprises of 75km (the Project”) including spurs, will be awarded on BOT or EPC basis. The proposed expressway from Kanpur to Lucknow is a new alignment which will connect the Uttar Pradesh state capital Lucknow with the industrial town Kanpur. Lucknow is the capital city of Uttar Pradesh. Kanpur is the commercial capital of Uttar Pradesh. Presently, these two cities are connected by National Highway NH-25 which is congested. The proposed expressway will reduce the travel time between two cities and will be considered as twin cities. The proposed Kanpur - Lucknow Expressway falls in 2 districts of State Uttar Pradesh, i.e. Unnao district & Lucknow District. The existing National Highway– 25 which is running parallel to the proposed expressway carries one of the highest traffic from Lucknow to Kanpur & either side in the state of U.P. The proposed expressway facility is proposed to be developed as a fully access controlled facility on a new alignment. Start point from the intersection of Shaheed Path (Near Transport Nagar Metro Station) with existing NH-25 and endpoint is near Shuklaganj Intersection (near Ata village), which will connect the proposed expressway to the NH 91 bypass. -

District Census Handbook, Etawah, Part XIII-B, Series-22, Uttar Pradesh
,CENSUS' 1981 ·;"Ttl XIII - ~ I ' . , ~/SERIES·22i 'lff,"~' MqVfifl .... S1~~ ~~ ~ UTTAR'· ·PRADESH, Pt1rt XIII· B . PRIMARY CENSUS J,SST,RACl Nr'll {GmT !!tan ~"~T ·DISTlUCT ~~~~l ETAWAH DISTRICT CENSUS . HANDBOOK ~~ ~ ~vf.r" ftr ~;~~~, Qtlft, 1. SR=QTq.fT i-il 2. ' srrlf!fi'{<i' v-vi 3. f~~ <fiT ~T;rf",o;r ix-x 4. ~~~<11uf ari'Cfi~ s. fGfCifT Gf'flTll'f<rT ~R=;Cfir <fir qf~:qlf xi-xiii 6. f~T smrf1{Cfi iif~Hm: ~~Flt iif;:r~~t1T 18-17 7• ar~w:qcr iifrfcr~ ~ f¥i SlNf1{Cf) \ifiM''''<i'r~T~ 18-2,; 8, ~f.qij ;;t'f-~ffftff ~ full" 'SfNf'f'li iif;WIl'fi'f'Tl(fT, 26-33 9. ~1{)Jr/.'I1TU7.f ~T'rl'1{Cfi \jj;:r~lIFfHn, (;:r~'3Tm ~ UllIT c:f'fT 'f11'if it i(ri ~ ~~) 3S-lSl 1. t!~T q~" (i) CT~"r(:f1{r;;f," (ii) llnrl <fiT qllfliiiif q:;ft 36-39 (Iii)' 'n~T1Jf ~r~fq<fi iifif'l'olTifrrn 44-73 (iv) • <T'l1;Tll srr~f;r~ iifif~UFtRf" (~trSfT ;:r~~q'ffi;cy;T)' 74-75 ( v) ~cTqT iI1T~cnf(1Cfir <fiT qf~f~ 77-82 (vi) <T~Utr ~Tt:rf1{Cfi iifil1T1Jfi(f'lr, (iifijef"..crtilR iI1T,\q'rf(:f'Pr) 84-85 (vii) iifq<l~CA'IJ'\ ;:r~Cfrf.;;fCfir 'fiT q-f~f~c 87-88 (viii) iI1Ti'rlt ~r~f'fCfi ;r.pJ'G'fifmT-: (~f~~ ;;1H ~"I') 98-91 (i:l) ~f~~ .;,,~ ~"I' 'fir q'f'\f~c 93 2. ~,1AJ CI'~~" (i) tT~«~ ;rA'Rr-t (n) llnrl <tr q~ifilf q:qT 96-99 (iii) llr;rT1Jf ~~fqCfi Gfif~I!T'lHr~ 194-129 (iv) if~Tlt ~l'{flfCfi ~iI1T1Jfi(Tm\ (~n:''f;rr "I~\q'rf~'fiT) 139-131· (v) 'll~~ if~ \.qTf~lflr 'fiT qf,~ 132-133 (vi) 'Wf'rtr ~T'ff~ ~JFtT'3r'\ (~T iI1T{ ~"I') (vii) ~~ iflJ'\ ~'Jt Cfir qf(f~c ii 3. -

Lucknow-Kanpur-Agra Via Mainpuri Sl.No 1 2 3 4 5
LUCKNOW-KANPUR-AGRA VIA MAINPURI SL.NO 1 2 3 4 5 SERVICE CODE R185 P185 K185 K185 E185 From SONOLI-10:30-GKP ALD-19:00 ARR 23:30 0:30 KANPUR DEP 0 0:15 1:00 6:00 6:15 6:30 ARR 0 2:40 3:25 8:00 8:40 8:30 KANNOJ DEP 81 81 2:45 3:30 8:15 8:45 8:45 ARR 5:05 5:50 10:35 11:05 11:05 MAINPURI DEP 95 176 5:20 6:05 10:50 11:20 11:20 ARR 6:40 7:25 12:20 12:40 12:50 SHIKOHABAD DEP 53 229 6:45 7:30 12:50 12:45 13:20 ARR 8:35 9:20 12:50 14:35 12:50 AGRA DEP 67 296 10:20 TO JAIPUR-16:20 AGRA-KANPUR-LUCKNOW VIA MAINPURI SL. No. 1 2 3 4 5 SERVICE CODE K186 C186 K186 P186 K186 From JAIPUR- 19:20 AJMER 18:00-JAIPUR 22:00 ARR 0:30 3:30 AGRA DEP 0 0:50 4:00 4:15 4:30 4:45 ARR 0 2:20 5:30 5:45 6:00 6:15 SHIKOHABAD DEP 67 67 2:50 5:45 6:15 6:15 6:45 ARR 4:20 7:15 7:45 7:45 8:15 MAINPURI DEP 53 120 4:35 7:30 8:00 8:00 8:30 ARR 6:35 9:30 10:00 10:00 10:30 KANNOJ DEP 95 215 6:50 9:45 10:15 10:15 10:45 ARR 8:50 11:45 12:15 12:15 12:45 KANPUR DEP 81 296 12:30 13:45 13:00 ARR LUCKNOW DEP 90 386 TO HMR-MAHOBA FTP-ALD FATEHPUR-ALD Page 1 of 8 LUCKNOW-KANPUR-AGRA VIA MAINPURI SL.NO 6 7 8 9 10 11 SERVICE CODE K185 K185 K185 R185 K185 R185 From SONOLI-17:00-GKP SONOLI-18:30-GKP ARR 6:00 7:30 KANPUR DEP 0 6:45 7:00 7:15 7:30 8:00 8:15 ARR 0 8:45 9:00 9:40 9:55 10:25 10:40 KANNOJ DEP 81 81 9:00 9:15 9:45 10:00 10:30 10:45 ARR 11:20 11:35 12:05 12:20 12:50 13:05 MAINPURI DEP 95 176 11:35 11:50 12:20 12:35 13:05 13:20 ARR 13:05 13:20 13:40 13:55 14:25 14:40 SHIKOHABAD DEP 53 229 13:35 13:50 13:45 14:00 14:30 14:45 ARR 13:35 13:50 15:35 15:50 16:20 16:35 AGRA DEP 67 296 17:35 16:45 TO JAIPUR-23:20 JAIPUR-22:00 AGRA-KANPUR-LUCKNOW VIA MAINPURI SL. -

Electrification
Electrification I Executive Summary of Railway Electrification With a view to reduce the Nation’s dependence on imported petroleum based energy and to enhance energy security of the Country, as well as to make the Railway System more eco-friendly and modernized, Indian Railways have been progressively electrifying its rail routes. Upto March 2016, 23,555 Route kilometers which is 35.32% of the total Railway network has been electrified. On this electrified route 64.80% of freight traffic & 51.30% of Passenger traffic is hauled with fuel cost on electric traction being merely 38.70% of the total traction fuel cost on Indian Railways. In XIIth plan(2012-17), the target has been further enhanced to 6,500 RKMs, out of which, 5,772 RKMs have been electrified in the last four years of XIIth plan i.e. (in 2012-16) as against the proportionate target of 5,200 RKMs. II Plan Period wise Progress of Railway Electrification Plan Period RKM Electrified Pre-Independence - 1925-1947 388 1st Five Year Plan - 1951-56 141 2nd Five Year Plan - 1956-61 216 3rd Five Year Plan - 1961-66 1,678 Annual Plan - 1966-69 814 4th Five Year Plan - 1969-74 954 5th Five Year Plan - 1974-78 533 Inter Plan - 1978-80 195 6th Five Year Plan - 1980-85 1,522 7th Five Year Plan - 1985-90 2,812 Inter Plan - 1990-92 1,557 8th Five Year Plan - 1992-97 2,708 9th Five Year Plan - 1997-02 2,484 10th Five Year Plan - 2002-07 1,810 11th Five Year Plan - 2007-12 4,556 1st year of 12th Five Year Plan 1,317 2nd year of 12th Five Year Plan 1,350 3rd year of 12th Five Year Plan 1,375 4th year of 12th Five Year Plan 1,730 67 III Sections Opened for Electric Traction After Inspection by Commissioner of Railway Safety in 2015-16.