Discovery Awaits You at the 81ST Scientific Sessions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Spring 2021 Dean's List Bertolon School of Business
Spring 2021 Dean’s List Bertolon School of Business Ben Abrahamson Matt Carroll Ambra Doku Matthew S Gubitose Kyle Acciavatti Megan Carroll Gianni Dominguez Michael Hakioglu Gianluca Acquafredda Haley H Carter Amanda Donahue Molly Hamer Bianca Adam Nic Carter Bill Donalds Neal Hansen Noelle Alaboudi Sebastian Carvalho Daniel Donator Lana Kathleen Harris Jimmy Alcott Gabriela Cassidy Fiori Dorne Billy Hart Kevin Aleman Maradiaga Christopher Castillo Preston Dougherty Caroline E Hebert Rachel Allen Jacqueline Emily Chan Ashley Downey Handi Henriquez Kevin Almonte City Chen Katelyn Rose Downey Erika L Hernandez Cesare Aloise Stone M Chen Phillip Dube Julio Hernandez Luidwin Amaya Nok Wan Chu Luke D Dudek Leslie Maria Herrera Nicholas Ansaldi Carolyn R Cinelli Nick Dunfee Jack Hobbs Jayquan Anthony Arthur-Vance Lexi Ciolino Erin Dwyer Austin Holbrook William Aubrey Alex Cisneros Katie Eleftheriou Dom Hooven Hannah Aveni Amber Cokash Mikayla Evangelista Luan Horjeti Sonny Badwal Max Matthew Cole Wesley Fagan Miriam Alexandra Horton Jeffrey Baez Ryan Collins Art Fawehinmi Drew Howard Colleen Balfour Tatyana Conde-Correa Miles Feeley Ryan Huber Siena Mae Barone Nayely Contreras Sydney Ferguson Bailey Marie Hughes Melane Barrios-Macario Nicole Cooney Elise Firth-Gonzalez Geech Huot Peter Barry Rachael A Corrao Ariana Fitzgerald Abigail Hurley Zacharie Joshua Beauchamp Connor Corrigan Cassidy Fletcher Tina Huynh Christopher Beaudoin Michael Ralph Cosco Lynn M Fletcher Jake Irvine Blake Holland Benway Matt Coyle Yulianny Frias Leonora A Ivers Vikram S Bhamra Abby S Crogan Ryan Fuentes Steven Jack Timothy Blake Rupert Crossley Noor Galal Billy Jackson Jr Marissa Blonigen Anabel Cruzeta Kerry Galvin Jessica Jeffrey Alexander Bloomer John G D’Alessandro Steve Garber Hannah Jensen Madison Blum Louis Richard D’Amico Mateo Garcia Quelsi Georgia Jimenez Babin Bohara Carly D’Orlando Sabrina Y. -

Management of Diabetes Mellitus Standards of Care and Clinical Practice Guidelines
WHO-EM/DIN6/E/G MANAGEMENT OF DIABETES MELLITUS STANDARDS OF CARE AND CLINICAL PRACTICE GUIDELINES Edited by Dr A.A.S. Alwan Regional Adviser, Noncommunicable Diseases WHO Regional Office for the Eastern Mediterranean WHO-EM/DIN6/E/G INTRODUCTION Available data from many countries of the Eastern Mediterranean Region (EMR) indicate that diabetes mellitus has become a problem of great magnitude and a major public health concern. Studies have demonstrated that, in some countries, diabetes affects up to 10% of the population aged 20 years and older. This rate may be doubled if those with impaired glucose tolerance (IGT) are also included. The manifestations of diabetes cause considerable human suffering and enormous economic costs. Both acute and late diabetic complications are commonly encountered. Long-term complications represented by cardiovascular diseases, cerebrovascular accidents, end-stage renal disease, retinopathy and neuropathies are already major causes of morbidity, disability and premature death in countries of this Region. The development of long-term complications is influenced by hyperglycaernia. Poor control of diabetes accelerates their progression. Thus, to prevent complications, good control of diabetes is essential and the management of diabetes should therefore aim to improve glycaemic control beyond that required to control its symptoms. Intensified therapy and maintaining near-normal blood glucose levels can result in considerable reduction in the risk of development of retinopathy, nephropathy and neuropathy. However, despite the high prevalence of diabetes and its complications and the availability of successful prevention strategies, essential health care requirements and facilities for self-care are often inadequate in this Region. Action is needed at all levels of health care and in the various aspects of diabetes care to bridge this gap and to improve health care delivery to people with diabetes. -

Did Israel Invent the Cherry Tomato?
University of Pennsylvania ScholarlyCommons Department of Medical Ethics and Health Policy Perelman School of Medicine 2016 Seeding Controversy: Did Israel Invent the Cherry Tomato? Anna Wexler University of Pennsylvania, [email protected] Follow this and additional works at: https://repository.upenn.edu/mehp Recommended Citation Wexler, Anna, "Seeding Controversy: Did Israel Invent the Cherry Tomato?" (2016). Department of Medical Ethics and Health Policy. 13. https://repository.upenn.edu/mehp/13 This paper is posted at ScholarlyCommons. https://repository.upenn.edu/mehp/13 For more information, please contact [email protected]. Seeding Controversy: Did Israel Invent the Cherry Tomato? Abstract This research brief explores the controversial history of the cherry tomato and analyzes its role in the construction of Israel's national identity. Since 2003, mentions of Israel having “invented” the cherry tomato have appeared in both Israeli and international media. However, such claims have sparked outrage on various blogs and websites, and questions have been raised about the veracity of Israel's claims—as well as about the true origin of the cherry tomato. I explore the history of the cherry tomato, tracing mentions of it from the Renaissance period to modern times. In addition, I clarify the assertions of Israeli scientists credited with the development of the cherry tomato—that their research transformed the cherry tomato into a commodity in the 1980s. Finally, I discuss the cherry tomato claim in light of the Israeli government's hasbara (Hebrew for “explanation”) efforts, which attempt to counter negative images of Israel in the international press. While much previous scholarship on food and nationalism has focused on the relationship between the cultivation, preparation, or consumption of a food and the construction of a national identity, the present work focuses on the relationship between the food's invention narrative and national identity. -

Get App BROCHURE
#EXPERIENCELIFE INTRODUCTION GROUP ADVENTURES INDEPENDENT TRIPS BAMBA BRAND KENYA, UGANDA 4 SOUTH AMERICA ASIA & RWANDA 54 SOUTH AMERICA HISTORY & PERU VIETNAM, PERU 22 TANZANIA 67 PHILOSOPHY 5 CAMBODIA & 40 56 THAILAND BOLIVIA 27 ZIMBABWE, BOLIVIA 69 BAMBA FOR INDONESIA & BOTSWANA & 6 CHILE & 57 CHILE GOOD ARGENTINA 30 PHILIPPINES 43 NAMIBIA 71 WHY TRAVEL BRAZIL SRI LANKA & SOUTH AFRICA 58 ARGENTINA, 73 WITH BAMBA 7 31 MALDIVES 44 ISRAEL & COLOMBIA & BRAZIL 75 ECUADOR 33 INDIA, NEPAL & JORDAN 59 BAMBA APP 8 TIBET 45 COLOMBIA 77 TRIP STYLES JAPAN & SOUTH EUROPE 10 CENTRAL AMERICA GALPAGAGOS & KOREA 47 ICELAND MEXICO 34 60 ECUADOR 79 CHINA, BELIZE IRELAND, 35 KYRGYZSTAN, 48 SCOTLAND & CENTRAL AMERICA & THE KAZAKHSTAN 61 GUATEMALA & SCANDINAVIA CARIBBEAN COSTA RICA 36 OCEANIA SPAIN, MEXICO, CUBA, PORTUGAL, GUATEMALA & 82 NORTH AMERICA AUSTRALIA, NEW GERMANY & 62 BELIZE ZEALAND & FIJI 49 RUSSIA USA & CANADA 37 GUATEMALA, HONDURAS & AFRICA & MIDDLE EAST CROATIA, 85 GREECE & 63 COSTA RICA MOROCCO & TURKEY EGYPT 53 PANAMA 87 TABLE OF CONTENTS IT’S TIME TO GO AND EXPLORE THE WORLD! INDEPENDENT TRIPS TRAVEL PASSES CUBA & NEPAL 108 EUROPE SOUTH AMERICA CENTRAL THAILAND, CARIBBEAN 89 AMERICA 141 MALAYSIA & ISLANDS UZBEKISTAN, ICELAND & BRAZIL, SINGAPORE 153 MONGOLIA & NORWAY 120 ARGENTINA & COSTA RICA & CHINA 109 132 NORTH AMERICA UNITED CHILE PANAMA 142 VIETNAM, CAMBODIA & USA & CANADA JAPAN KINGDOM & 153 92 110 IRELAND 121 SOUTH AMERICA THAILAND PASSES 133 NORTH AMERICA ASIA OCEANIA SPAIN & USA & CANADA PORTUGAL 122 CHILE & 146 THAILAND NEW ZEALAND, -
Footprints an Informational Newsletter for Patients of APMA Member Podiatrists October 2017
footprints an informational newsletter for patients of APMA member podiatrists october 2017 special EDITION include a DPM for diabetes prevention & Manage Ment According to the CDC, more than 100 million US adults are living with either diabetes or prediabetes. If you have diabetes or prediabetes, it is essential to include a podiatrist for proper diabetes prevention and management. In fact, podiatrists can reduce amputation rates up to 80 percent. In order for you not to become a part of that statistic, here are a few simple things you can do to keep your risk for diabetic ulcers and amputation low: Inspect feet daily. Check your Don’t go barefoot. Don’t go 1 feet and toes every day for 5 without shoes, even in your cuts, bruises, sores, or changes to own home. The risk of cuts and the toenails, such as thickening or infection is too great for those discoloration. with diabetes. Wear thick, soft socks. Avoid Never try to remove calluses, 2 socks with seams, which could 6 corns, or warts by yourself. rub and cause blisters or other Over-the-counter products can burn skin injuries. the skin and cause irreparable damage to the foot for people Exercise. Walking can keep with diabetes. 3 weight down and improve circulation. Be sure to wear See a podiatrist. Regular appropriate athletic shoes when 7 checkups by a podiatrist— exercising. at least annually—are the best WALKING CAN KEEP way to ensure that your feet WEIGHT DOWN AND Have new shoes properly remain healthy. 4 measured and fitted. Foot size IMPROVE CIRCULATION. -

Clinical Use of Hemoglobin A1c to Improve Diabetes Management
PRACTICAL POINTERS Clinical Use of Hemoglobin A1c to Improve Diabetes Management Alan M. Delamater, PhD, ABPP or more than 25 years, the hemo- one recent study conducted in Norway6 A1C values. Only 14% of the youths globin A1c (A1C) test has been revealed that the majority (82.6%) of were able to accurately describe the A1C Fthe most widely accepted out- 201 adult patients with type 1 diabetes test. Just 11, 7.8, and 7.8% correctly come measure for evaluating glycemic knew what their last A1C was, and most identified the A1C ranges for good, fair, control in individuals with diabetes. patients (90%) knew what a satisfactory and poor glycemic control, respectively. The test provides an index of a patient’s A1C value would be. But a significant Very few youths (1.6–3.2%) knew the average blood glucose level during the number of patients (42%) reported they blood glucose values corresponding to past 2–3 months1 and is considered to had low knowledge of A1C testing in specific A1C results. Only a small num- be the most objective and reliable general. Furthermore, 25% of patients ber of youths correctly estimated the measure of long-term metabolic con- did not think that treatment intensifica- short- and long-term risks associated trol.2,3 The Diabetes Control and tion should occur at an A1C value of with A1C values of 7 and 12%. In this Complications Trial established that 10%. sample, there was a significant lack of maintaining A1C levels as close as pos- A recent cross-sectional study knowledge concerning the meaning and sible to the normal range results in con- examined the relationship between implications of the A1C test. -

De Nakomelingen Van Bernhard Wibben
een genealogieonline publicatie De nakomelingen van Bernhard Wibben door Cees Eekhout 5 augustus 2021 De nakomelingen van Bernhard Wibben Cees Eekhout De nakomelingen van Bernhard Wibben Generatie 1 1. Bernhard Wibben. Hij is getrouwd met Taleke. Zij kregen 1 kind: Hermann Wibben, volg 2. Bernhard is overleden. Generatie 2 2. Hermann Wibben, zoon van Bernhard Wibben en Taleke, is geboren rond 1645 in Wahn, Germany. Hij is getrouwd op 30 oktober 1666 in Sögel, Duitsland met Hempe Manings. Zij kregen 4 kinderen: Talle Wibben, volg 3. Bernhard Wibben, volg 4. Jan Wibben, volg 5. Hermann Wibben, volg 6. Hermann is overleden. Generatie 3 3. Talle Wibben, dochter van Hermann Wibben en Hempe Manings, is geboren op 3 april 1667 in Wahn, Germany. Talle is overleden. 4. Bernhard Wibben, zoon van Hermann Wibben en Hempe Manings, is geboren op 28 februari 1669 in Wahn, Germany. Bernhard is overleden. 5. Jan Wibben, zoon van Hermann Wibben en Hempe Manings, is geboren op 26 oktober 1671 in Lohe, Graafschap Lingen, Duitsland. Hij is getrouwd met NN NN. Zij kregen 3 kinderen: Geerd Anton Wibben, volg 7. Enne Wibben, volg 8. Herman Wibben, volg 9. Jan is overleden op 37 jarige leeftijd op 13 september 1709 in Lohe, Graafschap Lingen, Duitsland. 6. Hermann Wibben, zoon van Hermann Wibben en Hempe Manings, is geboren op 28 augustus 1679 in Lohe, Graafschap Lingen, Duitsland. Hermann is overleden. https://www.genealogieonline.nl/stamboom-cees-eekhout-en-cobie-pronk/ 1 De nakomelingen van Bernhard Wibben Cees Eekhout Generatie 4 7. Geerd Anton Wibben, zoon van Jan Wibben en NN NN, is geboren op 24 november 1700 in Lohe, Graafschap Lingen, Duitsland. -

Characterization of the Ergosterol Biosynthesis Pathway in Ceratocystidaceae
Journal of Fungi Article Characterization of the Ergosterol Biosynthesis Pathway in Ceratocystidaceae Mohammad Sayari 1,2,*, Magrieta A. van der Nest 1,3, Emma T. Steenkamp 1, Saleh Rahimlou 4 , Almuth Hammerbacher 1 and Brenda D. Wingfield 1 1 Department of Biochemistry, Genetics and Microbiology, Forestry and Agricultural Biotechnology Institute (FABI), University of Pretoria, Pretoria 0002, South Africa; [email protected] (M.A.v.d.N.); [email protected] (E.T.S.); [email protected] (A.H.); brenda.wingfi[email protected] (B.D.W.) 2 Department of Plant Science, University of Manitoba, 222 Agriculture Building, Winnipeg, MB R3T 2N2, Canada 3 Biotechnology Platform, Agricultural Research Council (ARC), Onderstepoort Campus, Pretoria 0110, South Africa 4 Department of Mycology and Microbiology, University of Tartu, 14A Ravila, 50411 Tartu, Estonia; [email protected] * Correspondence: [email protected]; Fax: +1-204-474-7528 Abstract: Terpenes represent the biggest group of natural compounds on earth. This large class of organic hydrocarbons is distributed among all cellular organisms, including fungi. The different classes of terpenes produced by fungi are mono, sesqui, di- and triterpenes, although triterpene ergosterol is the main sterol identified in cell membranes of these organisms. The availability of genomic data from members in the Ceratocystidaceae enabled the detection and characterization of the genes encoding the enzymes in the mevalonate and ergosterol biosynthetic pathways. Using Citation: Sayari, M.; van der Nest, a bioinformatics approach, fungal orthologs of sterol biosynthesis genes in nine different species M.A.; Steenkamp, E.T.; Rahimlou, S.; of the Ceratocystidaceae were identified. -

Performance of the Insulin-Only Ilet Bionic Pancreas and The
e118 Diabetes Care Volume 44, June 2021 Performance of the Insulin-Only Luz E. Castellanos,1 Courtney A. Balliro,1 Jordan S. Sherwood,1 Rabab Jafri,1 iLet Bionic Pancreas and the Mallory A. Hillard,1 Evelyn Greaux,1 Rajendranath Selagamsetty,2 Hui Zheng,3 Bihormonal iLet Using Firas H. El-Khatib,2 Edward R. Damiano,2,4 and Dasiglucagon in Adults With Type Steven J. Russell1 1 Diabetes in a Home-Use Setting Diabetes Care 2021;44:e118–e120 | https://doi.org/10.2337/dc20-1086 Reductions in blood glucose levels in with insulin lispro (Eli Lilly) or aspart (Table 1). The mean CGM glucose and people with diabetes are often achieved (Novo Nordisk), the bihormonal iLet for time in range (70–180 mg/dL) were 149 at the expense of increased hypoglyce- 7dayswithdasiglucagon(4mg/mL) ±13mg/dLand72±8%,respectively,in mia. A novel approach is to automati- and insulin lispro or aspart, or both, us- the insulin-only period, and 139 ± 11 cally deliver microdose glucagon when ing the same glucose target (110 mg/ mg/dL and 79 ± 9%, respectively, in the automation of insulin delivery alone is dL), in random order. There were no re- bihormonal period. The mean daily car- not sufficient to prevent hypoglycemia. strictions on diet or exercise. The prima- bohydrates consumed to prevent or The approach requires a bihormonal de- ry outcomes were prespecified iLet treat hypoglycemia were 16 ± 13 g and vice and a stable form of glucagon or operational thresholds. The key second- 18 ± 21 g in the insulin-only and bihor- glucagon analog. -
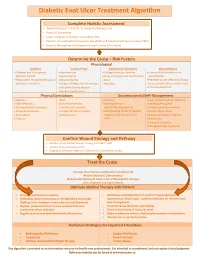
Diabetic Foot Ulcer Treatment Algorithm
Diabetic Foot Ulcer Treatment Algorithm Complete Holistic Assessment Medical/Surgical History & Co-morbidity Management Physical Examination Lower Leg (LLA) including monofilament test Perform Arterial Brachial Pressure Index (ABPI) and Toe Brachial Pressure Index (TBPI) Diabetic Management (Glycemic and Lipid Control & Nutrition) Determine the Cause – Risk Factors Physiological Diabetes Vascular Flow Autoimmune Disorders Wound History Diabetes and sub-optimal Hypertension Collagen vascular diseases History of foot infections or glycemic control Heart disease Immunosuppressant medications osteomyelitis Neuropathic changes with lack of Hyperlipidemia Gout Presence of toe infections (fungal protective sensation History of deep vein thrombosis Vasculitis or bacterial), callous and/or corns Peripheral artery disease Previous ulceration Venous Insufficiency Physical Limitations Socioeconomic/Self-Management Obesity Gait Smoking Lack of awareness for self-care Foot deformity Nutritional deficits Inadequate foot Inadequate hygiene Decreased level of activity Limited joint mobility wear/offloading devices Unsafe home environment Visual disturbances Congenital abnormalities Lack/Inability to afford diabetic Alcohol/drug abuse Amputation Osteoporosis supplies, foot care and foot Decreased Cognitive Ability Trauma wear Depression Financial insecurity Decreased level of activity Confirm Wound Etiology and Pathway Results of LLA, Monofilament Testing and ABPI/ TBPI Results of wound assessment Diagnostic -
Download the Program
The first International Congress of Neuroimmunology was held in Stresa, Italy, in 1982 and wasThe organized first International by Drs. Peter Congress O. Behan of Neuroimmunology and Federico Spreafico. was held The in secondStresa, Italy,International in Congress1982 and of wasNeuroimmunology organized by Drs. was Peter held O.in Philadelphia,Behan and Federico PA, and Spreafico. was organised The second by C.S. Raine andInternational Dale E. McFarlin. Congress It was of atNeuroimmunology this meeting in Philadelphiawas held in inPhiladelphia, 1987 that itPA, was and decided was to startorganised an international by C.S. Raine society, and the Dale International E. McFarlin. Society It was ofat Neuroimmunology,this meeting in Philadelphia and an election wasin 1987held forthat a it panel was decided of officers. to start C.S. anRaine international was elected society, President, the International John Newson-Davis Society Vice President,of Neuroimmunology, Robert Lisak andTreasurer an election and Kenethwas held Johnson for a panel Secretary, of officers. together Cedric with S. an InternationalRaine was Advisoryelected President,Board. The John Society Newson-Davis was incorporated Vice President,in 1988. Subsequent Robert Lisak meetings wereTreasurer in Jerusalem and Kenneth 1991 (Oder Johnson Abramsky Secretary, and togetherHaim Ovadia), with Amsterdaman International 1994 (KeeAdvisory Lucas), Board. Montreal 1998 (Jack Antel and Trevor Owens), Edinburgh 2001 (John Greenwood,The Society Sandra was Amor,incorporated David Baker, in 1988.John -

YAP1 and the Hippo Signaling Pathway Regulate Progenitor Proliferation
YAP1 and the Hippo Signaling Pathway Regulate Progenitor Proliferation Inaugural-Dissertation to obtain the academic degree Doctor rerum naturalium (Dr. rer. nat.) submitted to the Department of Biology, Chemistry and Pharmacy, Freie Universität Berlin submitted by Dipl.-Biochem. Karin Schlegelmilch born in Berlin, Germany 2013 I conducted my doctoral studies from July 2009 until February 2013 at the Boston Children’s Hospital/ Department for Stem Cell and Regenerative Biology of Harvard University in Boston, USA under the supervision of Assistant Prof. Dr. Fernando D. Camargo. 1st Reviewer: Assistant Prof. Dr. Fernando D. Camargo, Harvard University, Boston, USA 2nd Reviewer: Prof. Dr. Petra Knaus, Freie Universität Berlin, Berlin, Germany Date of defense: Acknowledgements Most importantly, I would like to thank Assistant Professor Fernando Camargo for giving me the great opportunity to work in his laboratory, for always being there for stimulating discussions and providing guidance and support. I would also like to thank Professor Petra Knaus. Without her support and commitment, my PhD thesis abroad would not have been possible. I thank my whole family and in particular my parents, Sigrid and Walter Schlegelmilch, who have supported me in my decisions all my life. I am moreover truly grateful to my brother Ingo Schlegelmilch for all his encouragement. I am immensely grateful to Jan Riethmayer for supporting me in every possible way throughout my PhD, it means so much to me and made all the difference. I am especially thankful to have met my amiga Ingrid Carvacho during the time at Children’s Hospital. Thanks so much for always being there for me and finding the right words.