Gastrointestinal Tract 5: the Anatomy and Functions of the Large Intestine
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Vestibule Lingual Frenulum Tongue Hyoid Bone Trachea (A) Soft Palate
Mouth (oral cavity) Parotid gland Tongue Sublingual gland Salivary Submandibular glands gland Esophagus Pharynx Stomach Pancreas (Spleen) Liver Gallbladder Transverse colon Duodenum Descending colon Small Jejunum Ascending colon intestine Ileum Large Cecum intestine Sigmoid colon Rectum Appendix Anus Anal canal © 2018 Pearson Education, Inc. 1 Nasopharynx Hard palate Soft palate Oral cavity Uvula Lips (labia) Palatine tonsil Vestibule Lingual tonsil Oropharynx Lingual frenulum Epiglottis Tongue Laryngopharynx Hyoid bone Esophagus Trachea (a) © 2018 Pearson Education, Inc. 2 Upper lip Gingivae Hard palate (gums) Soft palate Uvula Palatine tonsil Oropharynx Tongue (b) © 2018 Pearson Education, Inc. 3 Nasopharynx Hard palate Soft palate Oral cavity Uvula Lips (labia) Palatine tonsil Vestibule Lingual tonsil Oropharynx Lingual frenulum Epiglottis Tongue Laryngopharynx Hyoid bone Esophagus Trachea (a) © 2018 Pearson Education, Inc. 4 Visceral peritoneum Intrinsic nerve plexuses • Myenteric nerve plexus • Submucosal nerve plexus Submucosal glands Mucosa • Surface epithelium • Lamina propria • Muscle layer Submucosa Muscularis externa • Longitudinal muscle layer • Circular muscle layer Serosa (visceral peritoneum) Nerve Gland in Lumen Artery mucosa Mesentery Vein Duct oF gland Lymphoid tissue outside alimentary canal © 2018 Pearson Education, Inc. 5 Diaphragm Falciform ligament Lesser Liver omentum Spleen Pancreas Gallbladder Stomach Duodenum Visceral peritoneum Transverse colon Greater omentum Mesenteries Parietal peritoneum Small intestine Peritoneal cavity Uterus Large intestine Cecum Rectum Anus Urinary bladder (a) (b) © 2018 Pearson Education, Inc. 6 Cardia Fundus Esophagus Muscularis Serosa externa • Longitudinal layer • Circular layer • Oblique layer Body Lesser Rugae curvature of Pylorus mucosa Greater curvature Duodenum Pyloric Pyloric sphincter antrum (a) (valve) © 2018 Pearson Education, Inc. 7 Fundus Body Rugae of mucosa Pyloric Pyloric (b) sphincter antrum © 2018 Pearson Education, Inc. -

The Digestive System Overview of the Digestive System • Organs Are Divided Into Two Groups the Alimentary Canal and Accessory
C H A P T E R 23 The Digestive System 1 Overview of the Digestive System • Organs are divided into two groups • The alimentary canal • Mouth, pharynx, and esophagus • Stomach, small intestine, and large intestine (colon) • Accessory digestive organs • Teeth and tongue • Gallbladder, salivary glands, liver, and pancreas 2 The Alimentary Canal and Accessory Digestive Organs Mouth (oral cavity) Parotid gland Tongue Sublingual gland Salivary glands Submandibular gland Esophagus Pharynx Stomach Pancreas (Spleen) Liver Gallbladder Transverse colon Duodenum Descending colon Small intestine Jejunum Ascending colon Ileum Cecum Large intestine Sigmoid colon Rectum Anus Vermiform appendix Anal canal Figure 23.1 3 1 Digestive Processes • Ingestion • Propulsion • Mechanical digestion • Chemical digestion • Absorption • Defecation 4 Peristalsis • Major means of propulsion • Adjacent segments of the alimentary canal relax and contract Figure 23.3a 5 Segmentation • Rhythmic local contractions of the intestine • Mixes food with digestive juices Figure 23.3b 6 2 The Peritoneal Cavity and Peritoneum • Peritoneum – a serous membrane • Visceral peritoneum – surrounds digestive organs • Parietal peritoneum – lines the body wall • Peritoneal cavity – a slit-like potential space Falciform Anterior Visceral ligament peritoneum Liver Peritoneal cavity (with serous fluid) Stomach Parietal peritoneum Kidney (retroperitoneal) Wall of Posterior body trunk Figure 23.5 7 Mesenteries • Lesser omentum attaches to lesser curvature of stomach Liver Gallbladder Lesser omentum -

Dynamic Colon Model (DCM): a Cine-MRI Informed Biorelevant in Vitro Model of the Human Proximal Large Intestine Characterized by Positron Imaging Techniques
pharmaceutics Article Dynamic Colon Model (DCM): A Cine-MRI Informed Biorelevant In Vitro Model of the Human Proximal Large Intestine Characterized by Positron Imaging Techniques Konstantinos Stamatopoulos 1,* , Sharad Karandikar 2, Mark Goldstein 3, Connor O’Farrell 1, Luca Marciani 4 , Sarah Sulaiman 4 , Caroline L. Hoad 5, Mark J. H. Simmons 1 and Hannah K. Batchelor 6,7 1 School of Chemical Engineering, University of Birmingham, Edgbaston, Birmingham B15 2TT, UK; [email protected] (C.O.); [email protected] (M.J.H.S.) 2 Department of Surgery, University Hospitals Birmingham NHS Foundation Trust, Birmingham Heartlands Hospital, Bordesley Green East, Birmingham B9 5SS, UK; [email protected] 3 Department of Radiology, University Hospitals Birmingham NHS Foundation Trust, Birmingham Heartlands Hospital, Bordesley Green East, Birmingham B9 5SS, UK; [email protected] 4 Nottingham Digestive Diseases Centre and National Institute for Health Research (NIHR) Nottingham Biomedical Research Centre, Nottingham University Hospitals NHS Trust and University of Nottingham, Nottingham NG7 2UH, UK; [email protected] (L.M.); [email protected] (S.S.) 5 Sir Peter Mansfield Imaging Centre, University of Nottingham, Nottingham NG7 2QX, UK; [email protected] 6 Institute of Clinical Sciences, College of Medical and Dental Sciences, Medical School Building, University of Birmingham, Edgbaston, Birmingham B15 2TT, UK; [email protected] 7 Strathclyde Institute of Pharmacy and Biomedical Sciences, University of Strathclyde, 161 Cathedral Street, Glasgow G4 0RE, UK * Correspondence: [email protected] or [email protected]; Tel.: +44-0121-4145-354 Received: 8 June 2020; Accepted: 10 July 2020; Published: 13 July 2020 Abstract: This work used in vivo MRI images of human colon wall motion to inform a biorelevant Dynamic Colon Model (DCM) to understand the interplay of wall motion, volume, viscosity, fluid, and particle motion within the colon lumen. -

Motility in the Large Intestine Physiology > Digestive > Digestive
Motility in the Large Intestine Physiology > Digestive > Digestive HAUSTRAL CONTRACTIONS (Definition): Slow, segmenting movements that further mix chyme. • About every 30 minutes. • Occur in haustra: small pouches caused by the teniae coli (longitudinal smooth muscle ribbons that run along outside the entire length of the colon). Because they are shorter than the large intestine, the large intestine tucks between the teniae and form sacs • Primarily occur in ascending and transverse colons. • Produced by contractions of smooth muscle layer Steps 1. Chyme fills a haustrum 2. Distension in the haustrum. 3. Smooth muscle layer contracts 4. Contractions move chyme into the next haustrum and subsequent haustra, where the sequence begins again. #Note that haustral contractions play a relatively minor role in propelling fecal waste through the large intestine; their main function to further mix waste. Contractions also bring chyme in close contact with the large intestine mucosal layer to maximize water and electrolyte absorption • Hasutral contractions also occur in the descending and sigmoid colon to further concentrate stored fecal waste prior to elimination. MASS MOVEMENTS (Definition): slow, but powerful contractions of the large intestine that move undigested waste to the rectum for defecation via the anus. • Much like stronger and sustained peristaltic contractions. • 3-4 times a day. • Mainly in the transverse, descending, and sigmoid colons. • Produced by circular layer (smooth muscle) contractions Steps 1. Undigested waste in the transverse colon. 2. Triggered by the gastrocolic reflex (initiated following ingestion of a meal when food enters the stomach causes its distension) 3. Circular layer contracts in the transverse colon 4. Contractions move waste towards the rectum. -

Dr.Hameda Abdulmahdi College of Medicine /Dep. of Anatomy & Histology
Dr.Hameda abdulmahdi College of Medicine /Dep. of anatomy & histology 2nd stage Large Intestine The large intestine or bowel, which absorbs water and electrolytes and forms indigestible material into feces, has the following regions: the short cecum, with the ileocecal valve and the appendix; the ascending, transverse, descending, and sigmoid colon; and the rectum, where feces is stored prior to evacuation .The mucosa lacks villi and except in the rectum has no major folds. Less than one-third as long as the small intestine, the large intestine has a greater diameter (6-7 cm). The wall of the colon is puckered into a series of large sacs called haustra (L. sing. haustrum, bucket, scoop). The mucosa of the large bowel is penetrated throughout its length by tubular intestinal glands. These and the intestinal lumen are lined by goblet and absorptive cells, with a small number of enteroendocrine cells. The columnar absorptive cells or colonocytes have irregular microvilli and dilated intercellular spaces indicating active fluid absorption . Goblet cells producing lubricating mucus become more numerous along the length of the colon and in the rectum. Epithelial stem cells are located in the bottom third of each gland. The lamina propria is rich in lymphoid cells and in lymphoid nodules that frequently extend into the submucosa . The richness in MALT is related to the large bacterial population of the large intestine. The appendix has little or no absorptive function but is a significant component of MALT . The muscularis of the colon has longitudinal and circular layers but differs from that of the small intestine, with fibers of the outer layer gathered in three separate longitudinal bands called teniae coli . -

Aandp2ch25lecture.Pdf
Chapter 25 Lecture Outline See separate PowerPoint slides for all figures and tables pre- inserted into PowerPoint without notes. Copyright © McGraw-Hill Education. Permission required for reproduction or display. 1 Introduction • Most nutrients we eat cannot be used in existing form – Must be broken down into smaller components before body can make use of them • Digestive system—acts as a disassembly line – To break down nutrients into forms that can be used by the body – To absorb them so they can be distributed to the tissues • Gastroenterology—the study of the digestive tract and the diagnosis and treatment of its disorders 25-2 General Anatomy and Digestive Processes • Expected Learning Outcomes – List the functions and major physiological processes of the digestive system. – Distinguish between mechanical and chemical digestion. – Describe the basic chemical process underlying all chemical digestion, and name the major substrates and products of this process. 25-3 General Anatomy and Digestive Processes (Continued) – List the regions of the digestive tract and the accessory organs of the digestive system. – Identify the layers of the digestive tract and describe its relationship to the peritoneum. – Describe the general neural and chemical controls over digestive function. 25-4 Digestive Function • Digestive system—organ system that processes food, extracts nutrients, and eliminates residue • Five stages of digestion – Ingestion: selective intake of food – Digestion: mechanical and chemical breakdown of food into a form usable by -

Digestive System Part 3(The Large Intestine) the Large Intestine Is the Terminal Part of the Alimentary Canal
Digestive system part 3(The Large Intestine) The large intestine is the terminal part of the alimentary canal. The primary function of this organ is to finish absorption of nutrients and water, synthesize certain vitamins, form feces, and eliminate feces from the body. Structure The large intestine runs from the appendix to the anus. It frames the small intestine on three sides. Despite its being about one-half as long as the small intestine, it is called large because it is more than twice the diameter of the small intestine, about 3 inches. The large intestine is subdivided into four main regions: the cecum, the colon, the rectum, and the anus. The ileocecal valve, located at the opening between the ileum and the large intestine, controls the flow of chyme from the small intestine to the large intestine. Cecum The first part of the large intestine is the cecum, a sac-like structure that is suspended inferior to the ileocecal valve. It is about 6 cm (2.4 in) long, receives the contents of the ileum, and continues the absorption of water and salts. The appendix (or vermiform appendix) is a winding tube that attaches to the cecum. Although the 7.6-cm (3-in) long appendix contains lymphoid tissue, suggesting an immunologic function, this organ is generally considered vestigial. However, at least one recent report postulates a survival advantage conferred by the appendix: In diarrheal illness, the appendix may serve as a bacterial reservoir to repopulate the enteric bacteria for those surviving the initial phases of the illness. Moreover, its twisted anatomy provides a haven for the accumulation and multiplication of enteric bacteria. -
Digestive Functions
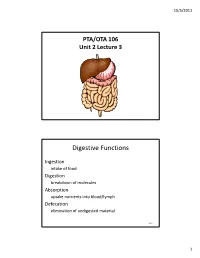
10/5/2011 PTA/OTA 106 Unit 2 Lecture 3 Digestive Functions Ingestion intake of food Digestion breakdown of molecules Absorption uptake nutrients into blood/lymph Defecation elimination of undigested material 25-2 1 10/5/2011 Stages of Digestion • Mechanical digestion – physical breakdown of food into smaller particles – teeth and churning action of stomach and intestines • Chemical digestion – series of hydrolysis reactions that break macromolecules into their monomers – enzymes from saliva, stomach, pancreas and intestines – results • polysaccharides into monosaccharides • proteins into amino acids • fats into glycerol and fatty acids 25-3 Figure 25.1 2 10/5/2011 Subdivisions of Digestive System • Digestive tract (GI tract) – 30 foot long tube extending from mouth to anus • Accessory organs – teeth, tongue, liver, gallbladder, pancreas, salivary glands 25-5 Lesser and Greater Omentum • Lesser - attaches stomach to liver • Greater - covers small intestines like an apron 25-6 3 10/5/2011 Stomach • Mechanically breaks up food, liquifies food and begins chemical digestion of protein and fat – resulting soupy mixture is called chyme • Does not absorb significant amount of nutrients – absorbs aspirin and some lipid-soluble drugs 25-8 4 10/5/2011 Gross Anatomy of Stomach • Muscular sac (internal volume from 50ml to 4L) – J - shaped organ with lesser and greater curvatures – regional differences • cardiac region just inside cardiac orifice • fundus - domed portion superior to esophageal opening • body - main portion of organ • pyloric region - narrow inferior end – antrum and pyloric canal • Pylorus - opening to duodenum – thick ring of smooth muscle forms a sphincter 25-9 Gross Anatomy of Stomach 25-10 5 10/5/2011 Liver, Gallbladder and Pancreas • All release important secretions into small intestine to continue digestion 25-11 Gross Anatomy of Liver • 3 lb. -
Digestive System Part
Business Reminder: No class Monday (Memorial Day) Midterm 2 is Tuesday 5/28/13 Optional review session tomorrow @ 5pm Homework due in Lab 1. PreLab 8 (1pt) 2. Replace a Missing Assignment (4 pts) Homework page 17 Digestive System Part 2 Digestive System Small intestine Major organ of digestion and absorption 2 - 4 m long; from pyloric sphincter to ileocecal valve Subdivisions Duodenum Jejunum Ileum Digestive System Small intestine Structural modifications Villi Intestinal glands Mucosa Submucosa Parotid gland Mouth (oral cavity) Sublingual gland Salivary Tongue Submandibular glands gland Esophagus Pharynx Stomach Pancreas Liver (Spleen) Gallbladder Transverse colon Duodenum Descending colon Small Jejunum Ascending colon intestine Ileum Cecum Large Sigmoid colon intestine Rectum Vermiform appendix Anus Anal canal Figure 23.1 Vein carrying blood to hepatic portal vessel Muscle layers Lumen Circular folds Villi (a) Figure 23.22a Microvilli (brush border) Absorptive cells Lacteal Goblet cell Blood Vilus capillaries Mucosa associated lymphoid tissue Enteroendocrine Intestinal crypt cells Muscularis Venule mucosae Lymphatic vessel Duodenal gland Submucosa (b) Figure 23.22b Microvilli Absorptive cell (b) Figure 23.3b Digestive System Chemical digestion in the small intestine Food entering SI = partially digested Intestinal juice Water, mucous Crypt cells produce lysozyme Microvilli (brush border) Absorptive cells Lacteal Goblet cell Blood Villus capillaries Mucosa associated lymphoid tissue Enteroendocrine Intestinal crypt -

Treatment in General Practice
704 APRIL 4, 1936 OF BRtTISM 704 APRIL4,RADIOGRAPHS1936 OF THE -ALIMENTARYALIMENTARY TRACTTRACT. WTHEK,EDICA.BRITISH~~~~~~~~~~~~~JUIJI.AmTOURtNAL TREATMENT IN GENERAL PRACTICE This article is onie of a series on the manlagemen1t of some diseases of the digestive system met with in general practice. Niche or Pocket.-This is a projection of the barium shadow INTERPRETATION OF RADIOGRAPHS into the wall of the viscus or through it, and is nearly always OF THE ALIMENTARY TRACT due to an ulcer. is BY Incisura.-This a contraction of the circular muscle fibres or a cicatricial contracture indenting the barium shadow. E. XV. TWINING, M.R.C.S., L.R.C.P., D.M.R.E.Camb. In rare cases it may be due to a band or adhesion. (With Special Diverticulum.-This is a protrusion of the mucous membrane Plate) through a small gap in the muscular walls. Occasionally (" false " diverticulum) there is a protrusion of all layers of Radiographs of the alimentary tract should be studied the walls. with certain considerations in mind: 1. They represent a fluid cast of the internal surface, Oesophageal Lesions and show only profiles of that surface if the viscus is full. Nearly always malignant, oesophageal stricture shows 2. The actual walls of the viscus are, of course, in- an abrupt narrowing, emptying below by an irregular visible. It will be found extremely helpful, in studying channel; the dilatation above the stricture is rarely radiographs of the alimentary tract, to sketch in the extreme, though the dilated lumen may reach a breadth estimated outline of the peritoneal surface. -

Colonic Motor Activity and Bowel Function
Gut: first published as 10.1136/gut.9.4.442 on 1 August 1968. Downloaded from Gut, 1968, 9, 442-456 Colonic motor activity and bowel function Part I Normal movement of contents J. A. RITCHIE From the Motility Unit of the Nuffield Department of Clinical Medicine, The Radcliffle Infirmary, Oxford, and the Nuffield Institute for Medical Research, Oxford There have been few detailed accounts of human and descending colon by x-ray cinematography colonic movements since the original radiological during periods of up to two and a half minutes. He observations on animals by Cannon (1901). described the movement of haustral contents as Holzknecht (1909) described as a 'mass peristalsis' being slow, intermittent and circular within the a wave of contraction that moved down a narrowed haustrum, with no sign of directional intention. section of colon from which the interhaustral folds Ritchie, Ardran, and Truelove (1962) observed the had temporarily disappeared. The remains of a secondary contraction of individual haustra in the bismuth meal were propelled in this way in seconds pelvic colon some four to eight seconds after their from the transverse colon to the pelvic colon, leaving distension by injected liquid, and distinguished what the gut empty behind it. Holzknecht saw no other appeared to be longitudinal and circular components changes in the outline of the gut wall and concluded of such contractions. Serial contraction of liquid- that the activity of the normal colon was limited .o and gas-filled haustra produced a segmental propul- such sudden, brief and occasional movements, sive movement away from the site of introduction of occurring perhaps three times in a day. -
Digestive System
Chapter 25 *Lecture PowerPoint The Digestive System *See separate FlexArt PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Introduction • Most nutrients we eat cannot be used in existing form – Must be broken down into smaller components before the body can make use of them • Digestive system—essentially a disassembly line – To break down nutrients into a form that can be used by the body – To absorb them so they can be distributed to the tissues • Gastroenterology—the study of the digestive tract and the diagnosis and treatment of its disorders 25-2 General Anatomy and Digestive Processes • Expected Learning Outcomes – List the functions and major physiological processes of the digestive system. – Distinguish between mechanical and chemical digestion. – Describe the basic chemical process underlying all chemical digestion, and name the major substrates and products of this process. 25-3 General Anatomy and Digestive Processes Cont. – List the regions of the digestive tract and the accessory organs of the digestive system. – Identify the layers of the digestive tract and describe its relationship to the peritoneum. – Describe the general neural and chemical controls over digestive function. 25-4 Digestive Function • Digestive system—the organ system that processes food, extracts nutrients from it, and eliminates the residue 25-5 Digestive Function • Five stages of digestion – Ingestion: selective intake of