Dermatoglyphic Evaluation of Mentally Retarded Adolescents From
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Payment Locations - Muthoot
Payment Locations - Muthoot District Region Br.Code Branch Name Branch Address Branch Town Name Postel Code Branch Contact Number Royale Arcade Building, Kochalummoodu, ALLEPPEY KOZHENCHERY 4365 Kochalummoodu Mavelikkara 690570 +91-479-2358277 Kallimel P.O, Mavelikkara, Alappuzha District S. Devi building, kizhakkenada, puliyoor p.o, ALLEPPEY THIRUVALLA 4180 PULIYOOR chenganur, alappuzha dist, pin – 689510, CHENGANUR 689510 0479-2464433 kerala Kizhakkethalekal Building, Opp.Malankkara CHENGANNUR - ALLEPPEY THIRUVALLA 3777 Catholic Church, Mc Road,Chengannur, CHENGANNUR - HOSPITAL ROAD 689121 0479-2457077 HOSPITAL ROAD Alleppey Dist, Pin Code - 689121 Muthoot Finance Ltd, Akeril Puthenparambil ALLEPPEY THIRUVALLA 2672 MELPADAM MELPADAM 689627 479-2318545 Building ;Melpadam;Pincode- 689627 Kochumadam Building,Near Ksrtc Bus Stand, ALLEPPEY THIRUVALLA 2219 MAVELIKARA KSRTC MAVELIKARA KSRTC 689101 0469-2342656 Mavelikara-6890101 Thattarethu Buldg,Karakkad P.O,Chengannur, ALLEPPEY THIRUVALLA 1837 KARAKKAD KARAKKAD 689504 0479-2422687 Pin-689504 Kalluvilayil Bulg, Ennakkad P.O Alleppy,Pin- ALLEPPEY THIRUVALLA 1481 ENNAKKAD ENNAKKAD 689624 0479-2466886 689624 Himagiri Complex,Kallumala,Thekke Junction, ALLEPPEY THIRUVALLA 1228 KALLUMALA KALLUMALA 690101 0479-2344449 Mavelikkara-690101 CHERUKOLE Anugraha Complex, Near Subhananda ALLEPPEY THIRUVALLA 846 CHERUKOLE MAVELIKARA 690104 04793295897 MAVELIKARA Ashramam, Cherukole,Mavelikara, 690104 Oondamparampil O V Chacko Memorial ALLEPPEY THIRUVALLA 668 THIRUVANVANDOOR THIRUVANVANDOOR 689109 0479-2429349 -

Accused Persons Arrested in Kottayam District from 17.05.2020To23.05.2020
Accused Persons arrested in Kottayam district from 17.05.2020to23.05.2020 Name of Name of the Name of the Place at Date & Arresting Court at Sl. Name of the Age & Cr. No & Sec Police father of Address of Accused which Time of Officer, which No. Accused Sex of Law Station Accused Arrested Arrest Rank & accused Designation produced 1 2 3 4 5 6 7 8 9 10 11 Cr. No. 646/20 ERUMANGALATH H, U/S MINI CIVIL 18.05.20 KOTTAYAM 1 PHILIP JOSEPH JOSEPH 62 KUMARANALLOOR 2336,269,188 SREEJITH T BAILED STATION 12:02 Hrs WEST PS PO, KOTTAYAM IPC & 4(2)(a) OF KEPDO Cr. No. 646/20 BHAGAVATHY U/S MUHAMMED PARAMBIL H, MINI CIVIL 18.05.20 KOTTAYAM 2 ABDUL KHADER 52 2336,269,188 SREEJITH T BAILED BASHEER KARAPPUZHA PO, STATION 12:02 Hrs WEST PS IPC & 4(2)(a) KOTTAYAM OF KEPDO Cr. No. 646/20 KALAALAYAM H, U/S UNNIKRISHNA MINI CIVIL 18.05.20 KOTTAYAM 3 BHASKARAN 58 PADINJAREMURY 2336,269,188 SREEJITH T BAILED N STATION 12:02 Hrs WEST PS BHAGOM, VAIKOM IPC & 4(2)(a) OF KEPDO Cr. No. 646/20 VILLATHARA H, U/S MINI CIVIL 18.05.20 KOTTAYAM 4 SASI GOPALAKRISHNAN 44 NAGAMBADOM, 2336,269,188 SREEJITH T BAILED STATION 12:02 Hrs WEST PS KOTTAYAM IPC & 4(2)(a) OF KEPDO Cr. No. 646/20 KOMALAPURAM H, U/S AVARMMA, MINI CIVIL 18.05.20 KOTTAYAM 5 SAJEEVAN RAKHAVAN NAIR 50 2336,269,188 SREEJITH T BAILED PERUMBADAVU, STATION 12:02 Hrs WEST PS IPC & 4(2)(a) KOTTAYAM OF KEPDO Cr. -

Kerala Library Association-Kottayam Region
KERALA LIBRARY ASSOCIATION-KOTTAYAM REGION REPORT Presented at the Annual General Body mting held on 29 August 2020. Dear Professional partners, I am privileged to present before you the Report of the Kerala Library Association Kottayam Region for the year 2018-2020. The last Annual General Body meeting of KLA Kottayam region was held on 18 April 2018 in the Mahatma Gandhi University Library, Kottayam. The meeting was presided over by Sri. Tomy Joseph, Regional President of KLA. In addition to the members, the Dr K.P. Vijaya Kumar, President of KLA and Dr Suresh Kumar, Secretary, KLA were present at the meeting. OFFICE BEARERS 2018-2020 President Secretary Sri. Tomy Joseph Sri. Vimal Kumar V. Librarian, St. Thomas College, Pala Technical Assistant, Mahatma Gandhi University, Kottayam. Executive Committee Members Sri. Unnikrishnan S. Sri. Justin Thomas Assistant Librarian, Librarian, M G University, Kottayam St Joseph’s College of Engineering, Pala Smt. Mini G. Pillai Sri. Jasimudeen S. Deputy Librarian Librarian, MG University Library St. Stephen’s College, Uzhavoor. Smt. Savithry T.K. Phone: 09895786534 Technical Assistant, MG University Library Special Invitees Dr V.K. Thomas Smt. Laila T. Abraham Varakil Parambil House Former Deputy Librarian, MG University, Kottayam Kollappally, Kottayam Sri. Johny John Nidheeri Smt. Kavitha Chandran Former Librarian HOD in-charge Devamatha College, Kuravilangad Dept. of Library and Information Science Mahatma Gandhi University Sri. Suku J. Sri. Sajan Varghese Deputy Librarian, M G University, Kottayam Librarian Marthoma College, Thiruvalla. Auditor Smt. Annu George, Deputy Librarian, M G University, Kottayam ACTIVITIES OF THE REGIONAL COMMITTEE Programmes and events KLA Kottayam region has organized following programmes in association with various institutions till now. -
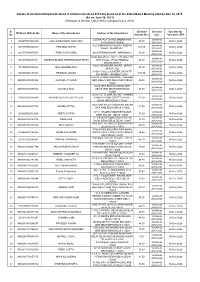
Details of Unclaimed/Unpaid Dividend
Details of Unclaimed/Unpaid Dividend (1st Interim Dividend 2019-20) declared at the 252nd Board Meeting held on Nov 12, 2019 (As on June 30, 2021) (Pursuant to Section 124(2) of the Companies Act, 2013) Sl. Dividend Dividend Due date for DP/Client ID/Folio No. Name of the Shareholder Address of the Shareholder No. Amount (Rs.) year Transfer to IEPF LODHAVALA CHAWL MANEKWADI 1st Interim 1 1204470001016189 MILI HARSHADRAI ANDHARIA 48.90 16-Dec-2026 BHAVNAGAR 000000 2019-2020 A-28,SONGANGA COLONY SEEPAT 1st Interim 2 1201130000028478 PRATIMA GUPTA 163.00 16-Dec-2026 ROAD BILASPUR 1 2019-2020 1st Interim 3 1201770100457678 PREM LATA GARG 220 PATRAM NAGAR NARWANA 2 48.90 16-Dec-2026 2019-2020 MAIN BAZAR AT. POST. SHIVRAJPUR 1st Interim 4 1301670000531511 HARSHALKUMAR HARISHKUMAR SHAH DIST. HALOL (PUNCHMAHAL) 48.90 16-Dec-2026 2019-2020 SHIVRAJPUR 3 3/262 VIDYADHAR NAGAR, JAIPUR 1st Interim 5 1301760000090292 ANIL KHANDELWAL 48.90 16-Dec-2026 JAIPUR 3020 2019-2020 H NO-42 VILL-LALBAZAR DALPATTI 1st Interim 6 1302340000199113 PRAMOD JALUKA 179.30 16-Dec-2026 PO-JHARIA DHANBAD 82811 2019-2020 D-41 III FLOOR SARASWATI GARDEN 1st Interim 7 IN30039414505106 KANWAL JIT KAUR NEW DELHI NEW DELHI NEW DELHI 48.90 16-Dec-2026 2019-2020 110001 65/25 NEW ROHTAK ROAD NEW 1st Interim 8 IN30094010287523 SUSHILA DEVI DELHI NEW DELHI NEW DELHI 48.90 16-Dec-2026 2019-2020 110005 1224/5 1ST FLOOR SUCHET CHAMBS 1st Interim 9 1100001100016546 MITHUN SECURITIES PVT LTD NAIWALA BANK STREET KAROL 81.50 16-Dec-2026 2019-2020 BAGH NEW DELHI 110005 1065 GALI RAJA UGGERSAIN -
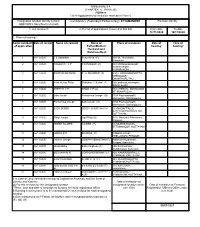
(CHAPTER V , PARA 25) FORM 9 List of Applications for Inclusion
ANNEXURE 5.8 (CHAPTER V , PARA 25) FORM 9 List of Applications for inclusion received in Form 6 Designated location identity (where Constituency (Assembly/£Parliamentary): ETTUMANOOR Revision identity applications have been received) 1. List number@ 2. Period of applications (covered in this list) From date To date 16/11/2020 16/11/2020 3. Place of hearing * Serial number$ Date of receipt Name of claimant Name of Place of residence Date of Time of of application Father/Mother/ hearing* hearing* Husband and (Relationship)# 1 16/11/2020 T S Sasankan Sukumaran (F) 10/314, Thoranathu, Aymanam, , 2 16/11/2020 PRASANTH V P P D PRASAD (F) 189 VENGALIKKALAM, KUMARAKOM , KUMARAKOM, , 3 16/11/2020 SWATHY KRISHNA P G PRADEEP (F) 4/314 PADINJAREKUTTU, NEENDOOR, ONAMTHURUTHU, , 4 16/11/2020 Kiran Kurian Philip Shibymon C Kurian (F) 550, padinjattumbhagam, Athirampuzha, , 5 16/11/2020 KEERTHI C P KIRAN C P (O) 553 CHERIVIL, MANNANAM, ATHIRAMPUZHA, , 6 16/11/2020 Babu Jacob Ponnamma Joseph (O) 510A Pazhayampallil, Mannanam, Athirampuzha, , 7 16/11/2020 Ponnamma Joseph Babu Jacob (H) 510A Pazhayampallil, Mannanam, Athirampuzha, , 8 16/11/2020 SUBY BOBBY BOBBY CHERIYAN (H) 233/MADAPPALLIL, SREEKANDAMANGALAM, KOTTAYAM, , 9 16/11/2020 Philip Joseph Sigi Philip (O) B412 Maniyalil, Ettumanoor, Kottayam, , 10 16/11/2020 AMEER NAJEEB NAJEEB (F) 13,NAJEEB MANZIL, ETTUMANOOR, KOTTAYAM, , 11 16/11/2020 GOKUL K R SIVADAS (F) 1 REMALAYAM, THELLAKOM, PEROOR, , 12 16/11/2020 Naveen Joseph JOSEPH SEBASTIAN (F) Pathinanchil parambil, Karippa, Arpookara, , 13 16/11/2020 -

Fj Eng 1788-2013.Pdf
MATHECKAL FAMILY JOURNAL - A REFERENCE MANUAL( AD 1788- 2013) By MATHECKAL KUDUMBAM November 26, 2014 AD 2013: 225th Birth Anniversary of Mathunni Matheckal (A Tribute to The Patriarch of Matheckal Family, Arakuzha) MATHECKEL FAMILY JOURNAL - A REFERENCE MANUAL (AD 1788 - 2013) To read Matheckal Family Journal online in English and Malayalam and access Database visit website: www.matheckalfamily.org But the hour will come - in fact it is here already - when true worshippers will worship the Father in sprit and truth: this is the kind of worshipper the Father wants. God is spirit, and those who worship must worship in spirit and truth - John 4:23-24 MATHECKAL FAMILY JOURNAL - A REFERENCE MANUAL (AD 2013) (ON THE 225TH BIRTH ANNIVERSARY OF ITS FOUNDER MATHUNNI MATHECKEN) I am the Vine, you are the branches. Whoever remains in me, with me in him, bears fruit in plenty; for cut off from me you can do nothing . Remain in my love.- (John 15: 5-6, 10) Acknowledgement Matheckal Family Journal - A Reference Manual (1788-2013) has seen the light of the day due to the collective contribution of several persons who patronised by way of providing sources of data, update of data, clear cut guidelines and policies in formu- lating the purpose,content, historical perspectives to meet the contemporary needs of perpection-a pristine understanding to foresee the aspirational needs of the future gen- erations of the Mathackal families to enable them evolve an appropriate roadmap for themselves . A comprehensive data base of the Matheckal family and a family website is a reality today. -
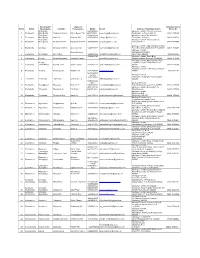
Sl.No. Block Location Mobile E-Mail Address of Akshaya Centre 1 Erattupetta Chennadu Kavala Sajida Beevi. T.M [email protected]
Panchayath/ Name of Akshaya Centre Sl.No. Block Municipality Location Entrepreneur Mobile E-mail Address of Akshaya Centre Phone No Erattupetta 9961985088, Akshaya e centre, Chennadu Kavala, 1 Erattupetta Municipality Chennadu Kavala Sajida Beevi. T.M 9447507691, [email protected] Erattupetta, Kottayam-686121 04822-275088 Erattupetta 9446923406, Akshaya e centre, Nadackal P O, 2 Erattupetta Municipality Hutha Jn. Shaheer PM 9847683049 [email protected] Erattupetta, Kottayam 04822-329714 Erattupetta Akshaya e centre, Thottumukku Jn., 3 Erattupetta Municipality Thottumukku Jn. Rasiya M Shereef 9847095886 [email protected] Erattupetta P O 04828-277550 Akshaya e centre, Opp. Melukavumattom 4 Erattupetta Melukavu Melukavu Mattom Anoop Mohan 9447515722 [email protected] Post office,Melukavumattom P O,686652 04822-220402 Akshaya e-centre, Minimol Antony Punnathaniyil Building 5 Erattupetta Moonnilavu Moonnilavu 9446861799 [email protected] Moonnilavu-686596 48222-86266 9745402710 Akshaya e centre, Chalil Bldg, 6 Erattupetta Poonjar Panachikkappara Aniamma Suresh [email protected] Panachikkapara, Poonjar P O-686581 04822-276506 Akshaya e centre, Panchayathu office Poonjar Complex,Poonjar Thekkekkara P O- 7 Erattupetta Thekkekkara Poonjar Town Shymol Jacob 9745402710 [email protected] 686582 04822-276506 Akshaya e centre, Panchayat Junction, Theekoy, Kottayam- 8 Erattupetta Teekkoy Panchayat Jn. Sulfath K H 9400233778 [email protected] 686581 48222-81145 9847093283 Suresh- Akshaya e-centre, 8547672267 Thalanadu, Thalanadu -

Andhra Pradesh
STATE DISTRICT BRANCH ADDRESS CENTRE IFSC CONTACT1 CONTACT2 CONTACT3 MICR_CODE BALAJI COMPLEX OPP. RAGHAVA THEATRE JAILKHANA CHITTOOR ROAD CHITTOOR – CIR@FED ANDHRA (ANDHRA 517 001 ANDHRA ERALBANK PRADESH CHITTOOR PRADESH) PRADESH CHITTOOR FDRL0001673 .CO.IN D.NO.6-7-587 0877 - A.K.NILAYAM 2231361 SRIPURAM COLONY TRP@FED ANDHRA ISKCON ROAD ERALBANK PRADESH CHITTOOR TIRUPATI TIRUPATI - 517 501 TIRUPATI FDRL0001683 .CO.IN AYYAPPA TOWERS (PHASE II), D. NO. 5 - 1 - 76, MAIN ROAD, OPP. TWO TOWN POLICE STATION, KAKINADA - 533001, EAST GODAVARI DURGA ANDHRA EAST DISTRICT, ANDHRA PRASADA KNA@FEDERA 0884 PRADESH GODAVARI KAKINADA PRADESH KAKINADA FDRL0001626 RAO K LBANK.CO.IN 2363611 SWAROOP GEORGE P, E DOOR NO: 60506, MAIL:RMD MAIN ROAD, @FEDERA OPP.SHYAMALA LBANK.CO. TALKIES, IN PH NO.: RAJAMUNDRY, 533 0883- ANDHRA EAST 101, ANDHRA RAJAHMUN 2461457(M PRADESH GODAVARI RAJAHMUNDRY PRADESH DRY FDRL0001341 ) 0863 – 2332277, 2332278 6-14-36, 14TH LANE GTR@FED ANDHRA ARUNDELPET ERALBANK PRADESH GUNTUR GUNTUR GUNTUR – 522 002 GUNTUR FDRL0001671 .CO.IN GOPAKUM AR P, E MAIL:HYD @FEDERA P B NO. 230, ORIENT LBANK.CO. ESTATE, ABIDS IN PH NO.: ROAD, HYDERABAD, 040- ANDHRA 500 001, ANDHRA HYDERABA 23205381( PRADESH HYDERABAD HYDERABAD PRADESH D FDRL0001124 CM) GROUND FLOOR, D.NO. 16-11- 20/6/6/1/1, OPP. TV TOWER, GAFOOR BAGH, SALEEM NAGAR COLONY, MALAKPET, HYDERABAD - HYDG@FE ANDHRA HYDERABAD / 500036, ANDHRA HYDERABA 040 DERALBA PRADESH HYDERABAD MALAKPET PRADESH D FDRL0001826 24540022 040 24540000 NK.CO.IN NO 301 III FLOOR 040 DEGA TOWERS 23303305 RAJBHAVAN -
![Kottayam/12-13/9351[57597]](https://docslib.b-cdn.net/cover/3116/kottayam-12-13-9351-57597-2613116.webp)
Kottayam/12-13/9351[57597]
Free tenders for Socket by Bharat Sanchar Nigam Limited-4406130316 57597 Auction Details Auction No MSTC/SRO/BSNL KOTTAYAM/5/AGM(EP -1) Kottayam/12 -13/9351[57597] Opening Date & Time 09-01-2013::11:00:00 Closing Date & Time Scheduled Time 09-01-2013::16:30:00 Closed At 09-01-2013::16:30:00 Inspection From Date 30-12-2012 Inspection Closing Date 08 -01 -2013 Seller Details Seller/Company Name BSNL KOTTAYAM Location AGM(EP-1) Kottayam Street pulimoodu junction City kottayam - 686001 Country INDIA Telephone 2563344 Fax 2304101 Email [email protected] Contact Person Sri.Cyril.C.Polackal LOT NO[PCB GRP]/LOT NAME LOT DESC QUANTITY ED/(ST/VAT) LOCATION 1.AB Post with Socket - 55 no 2.AB Post without Socket - 55 no 3.AB Post as is where is - 60 no Lot No: 01 As Applicable / Contact : SDE Phones Kumarakom 0481 1 LOT Telephone Exchange,Kumarakom State :Kerala 2525200 9447120344 5% Lot Name: AB Posts 1.Desktop PCs - 208 nos 2.Printers - 193nos 3.Monitors - 260 nos Lot No: 02 As Applicable / Telephone Exchange PCB GRP :[ E-Waste ] Contact : SDE Computer Kottayam .0481 1 LOT 2301300 9447192271 5% Building,Thirunakkara,Kottayam State :Kerala Lot Name: PC equipments 1.1000 AH Battery -48 cells Located at : Telephone Exchange,Puthuppally Contact : SDE Manarcadu,0481- 2370000,9446078970 2.200 AH VRLA Battery - 24 cells Located at :Telephone Exchange,Kuttickal 3.200 AH 2V VRLA Battery - 24 cells Located at : Telephone Exchange,Velloor 4.80AH VRLA Battery - 6 cells Located at : Telephone Exchange,Pampady Lot No: 03 5.40 AH Battery - 3 cells PCB GRP -

Dermatoglyphics in Medicine T
Bristol Medico-Chirurgical Journal. Vol 86 Dermatoglyphics in Medicine T. J. David, M.B., Ch.B. Bristol Royal Infirmary HISTORY the present "disease approach" to dermatoglyphics; The first known observations of dermal ridges were that is the study of dermatoglyphics in one particular made by Nehemiah Grew (1641-1712) who wrote in disease. So far the most important findings have been the Philosophical Transactions of 1684 "For if any one made by a "dermatoglyphic approach"; that is the will but take the pains, with an indifferent Glass, to study of a single dermatoglyphic parameter in different survey the Palm ot his Hand very well washed with a diseases, and a notable recent example is the result Ball; he may perceive innumerable little Ridges, of of the Total Ridge Count (see below) in anomalies of equal bigness and distance, and everywhere running the sex chromosome complement. parallel one with another. And especially upon the ends The permanence of fingerprints throughout life was and first Joynts of the Fingers and Thumb, upon the first established by Sir Francis Galton (Galton, 1892). top of the Ball, and near the root of the Thumb a little Although it is not known exactly when fingerprint pat- above the Wrist. In all which places, they are very terns are formed during intra-uterine life, certain intra- regularly disposed into spherical Triangles and Ellip- uterine growth disturbances affecting the extremities tics. Upon these Ridges stand the Pores, all in even (e.g. thalidomide phocomelia, dominant ectrodactyly, Rows, and of that magnitude, as to be visible to a and ectrodactyly due to hypoxia) will be accompanied very good Eye without a Glass." Marcello Malpighi by abnormal dermatoglyphics (Jancar, 1967). -

Club Health Assessment MBR0087
Club Health Assessment for District 306 A1 through June 2017 Status Membership Reports LCIF Current YTD YTD YTD YTD Member Avg. length Months Yrs. Since Months Donations Member Members Members Net Net Count 12 of service Since Last President Vice No Since Last for current Club Club Charter Count Added Dropped Growth Growth% Months for dropped Last Officer Rotation President Active Activity Fiscal Number Name Date Ago members MMR *** Report Reported Email ** Report *** Year **** Number of times If below If net loss If no report When Number Notes the If no report on status quo 15 is greater in 3 more than of officers that in 12 within last members than 20% months one year repeat do not have months two years appears appears appears in appears in terms an active appears in in brackets in red in red red red indicated Email red Clubs less than two years old 129130 Aluthgama Bentota Centennial 10/13/2016 Active 15 22 7 15 100.00% 0 0 0 N/R 127414 Ambalangoda City 05/05/2016 Cancelled(8*) 0 0 22 -22 -100.00% 22 1 0 None N/R 129153 Galkissa Centennial 10/11/2016 Active 55 56 1 55 100.00% 0 0 0 N/R 129248 Moratuwa Uyana Centennial 11/10/2016 Active 20 20 0 20 100.00% 0 7 T N/R 130668 Panadura Centennial 04/10/2017 Newly 22 22 0 22 100.00% 0 2 2 N/R Chartered 127315 Ratmalana 05/04/2016 Active 17 8 11 -3 -15.00% 20 1 0 T,M N/R 129154 Weligama Centennial 10/11/2016 Active 23 23 0 23 100.00% 0 0 N/R 130797 Weligama Mirissa Centennial 05/15/2017 Newly 21 21 0 21 100.00% 0 1 2 S N/R Chartered Clubs more than two years old 108907 AHUNGALLA DIAMOND 07/13/2010 -

Download Syllabus for M.Sc. in Anthropology
Syllabus for M. Sc. in Anthropology From Academic session 2020-21 onwards Department of Anthropology Central University of Orissa Koraput Page 0 of 70 M.Sc. in ANTHROPOLOGY As per UGC Gazette notification dated 4th July, 2018; ‘Credit’ means the Unit award, gained as learning outcome, by a learner by study efforts required to acquire the prescribed level of learning in respect of that Unit; Explanation: It is hereby clarified that a study effort for one credit means time required by a learner to understand the contents equivalent to 15 hours classroom teaching., or one hour teaching in a week. In this syllabus some courses are 4 credit weightage, and some are 2 credit weightage. For the easy assessment to calculate percentage, though all courses are marked 100 marks, but the weightage of course content is more for 4 credit course then two credit course. Semester-I Semester-I: General Anthropology Course Course Code Title Credits Full Mark No. 1 ANT – C 311 Biological Anthropology -I 4 100 2 ANT – C 312 Socio-Cultural Anthropology 4 100 3 ANT – C 313 Archaeological Anthropology 4 100 & Museology 4 ANT – C 314 Research Methods 4 100 5 ANT – C 315 Tribes in India 2 100 6 ANT – C 316 General Practical – I 2 100 Semester-II Semester-II: General Anthropology Course Course Code Title Credits Full Mark No. 7 ANT – C 321 Biological Anthropology -II 4 100 8 ANT – C 322 Theories of Society and 4 100 Culture 9 ANT – C 323 Pre- and Proto- History of 4 100 India, Africa and Europe 10 ANT – C 324 Indian Anthropology 4 100 11 ANT – C 325 Peasants in India 2 100 12 ANT – C 326 General Practical – II 2 100 Students can perform summer internship programme during summer vacation, which will be treated as Audit Course and will be reflected in the Grade Sheet.