Mary's Story: a Curriculum for Teaching Medical Terminology
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Reference Sheet 1
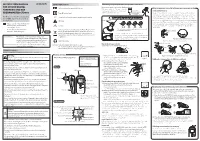
MALE SEXUAL SYSTEM 8 7 8 OJ 7 .£l"00\.....• ;:; ::>0\~ <Il '"~IQ)I"->. ~cru::>s ~ 6 5 bladder penis prostate gland 4 scrotum seminal vesicle testicle urethra vas deferens FEMALE SEXUAL SYSTEM 2 1 8 " \ 5 ... - ... j 4 labia \ ""\ bladderFallopian"k. "'"f"";".'''¥'&.tube\'WIT / I cervixt r r' \ \ clitorisurethrauterus 7 \ ~~ ;~f4f~ ~:iJ 3 ovaryvagina / ~ 2 / \ \\"- 9 6 adapted from F.L.A.S.H. Reproductive System Reference Sheet 3: GLOSSARY Anus – The opening in the buttocks from which bowel movements come when a person goes to the bathroom. It is part of the digestive system; it gets rid of body wastes. Buttocks – The medical word for a person’s “bottom” or “rear end.” Cervix – The opening of the uterus into the vagina. Circumcision – An operation to remove the foreskin from the penis. Cowper’s Glands – Glands on either side of the urethra that make a discharge which lines the urethra when a man gets an erection, making it less acid-like to protect the sperm. Clitoris – The part of the female genitals that’s full of nerves and becomes erect. It has a glans and a shaft like the penis, but only its glans is on the out side of the body, and it’s much smaller. Discharge – Liquid. Urine and semen are kinds of discharge, but the word is usually used to describe either the normal wetness of the vagina or the abnormal wetness that may come from an infection in the penis or vagina. Duct – Tube, the fallopian tubes may be called oviducts, because they are the path for an ovum. -

Recognizing When a Child's Injury Or Illness Is Caused by Abuse
U.S. Department of Justice Office of Justice Programs Office of Juvenile Justice and Delinquency Prevention Recognizing When a Child’s Injury or Illness Is Caused by Abuse PORTABLE GUIDE TO INVESTIGATING CHILD ABUSE U.S. Department of Justice Office of Justice Programs 810 Seventh Street NW. Washington, DC 20531 Eric H. Holder, Jr. Attorney General Karol V. Mason Assistant Attorney General Robert L. Listenbee Administrator Office of Juvenile Justice and Delinquency Prevention Office of Justice Programs Innovation • Partnerships • Safer Neighborhoods www.ojp.usdoj.gov Office of Juvenile Justice and Delinquency Prevention www.ojjdp.gov The Office of Juvenile Justice and Delinquency Prevention is a component of the Office of Justice Programs, which also includes the Bureau of Justice Assistance; the Bureau of Justice Statistics; the National Institute of Justice; the Office for Victims of Crime; and the Office of Sex Offender Sentencing, Monitoring, Apprehending, Registering, and Tracking. Recognizing When a Child’s Injury or Illness Is Caused by Abuse PORTABLE GUIDE TO INVESTIGATING CHILD ABUSE NCJ 243908 JULY 2014 Contents Could This Be Child Abuse? ..............................................................................................1 Caretaker Assessment ......................................................................................................2 Injury Assessment ............................................................................................................4 Ruling Out a Natural Phenomenon or Medical Conditions -

Nasolabial and Forehead Flap Reconstruction of Contiguous Alar
Journal of Plastic, Reconstructive & Aesthetic Surgery (2017) 70, 330e335 Nasolabial and forehead flap reconstruction of contiguous alareupper lip defects Jonathan A. Zelken a,b, Sashank K. Reddy c, Chun-Shin Chang a, Shiow-Shuh Chuang a, Cheng-Jen Chang a, Hung-Chang Chen a, Yen-Chang Hsiao a,* a Department of Plastic and Reconstructive Surgery, Chang Gung Memorial Hospital, College of Medicine, Chang Gung University, Taipei, Taiwan b Department of Plastic and Reconstructive Surgery, Breastlink Medical Group, Laguna Hills, CA, USA c Department of Plastic and Reconstructive Surgery, Johns Hopkins Hospital, Baltimore, MD, USA Received 4 May 2016; accepted 31 October 2016 KEYWORDS Summary Background: Defects of the nasal ala and upper lip aesthetic subunits can be Nasal reconstruction; challenging to reconstruct when they occur in isolation. When defects incorporate both Nasolabial flap; the subunits, the challenge is compounded as subunit boundaries also require reconstruc- Rhinoplasty; tion, and local soft tissue reservoirs alone may provide inadequate coverage. In such cases, Forehead flap we used nasolabial flaps for upper lip reconstructionandaforeheadflapforalarrecon- struction. Methods: Three men and three women aged 21e79 years (average, 55 years) were treated for defects of the nasal ala and upper lip that resulted from cancer (n Z 4) and trauma (n Z 2). Unaffected contralateral subunits dictated the flap design. The upper lip subunit was excised and replaced with a nasolabial flap. The flap, depending on the contralateral reference, determined accurate alar base position. A forehead flap resurfaced or replaced the nasal ala. Autologous cartilage was used in every case to fortify the forehead flap reconstruction. Results: Patients were followed for 25.6 months (range, 1e4 years). -

Mad-Cow’ Worries Intensify Becoming Prevalent.” Institute
The National Livestock Weekly May 26, 2003 • Vol. 82, No. 32 “The Industry’s Largest Weekly Circulation” www.wlj.net • E-mail: [email protected] • [email protected] • [email protected] A Crow Publication ‘Mad-cow’ worries intensify becoming prevalent.” Institute. “The (import) ban has but because the original diagnosis Canada has a similar feed ban to caused a lot of problems with our was pneumonia, the cow was put Canada what the U.S. has implemented. members and we’re hopeful for this on a lower priority list for testing. Under that ban, ruminant feeds situation to be resolved in very The provincial testing process reports first cannot contain animal proteins be- short order.” showed a possible positive vector North American cause they may contain some brain The infected cow was slaugh- for mad-cow and from there the and spinal cord matter, thought to tered January 31 and condemned cow was sent to a national testing BSE case. carry the prion causing mad-cow from the human food supply be- laboratory for a follow-up test. Fol- disease. cause of symptoms indicative of lowing a positive test there, the Beef Industry officials said due to pneumonia. That was the prima- test was then conducted by a lab Canada’s protocol regarding the ry reason it took so long for the cow in England, where the final de- didn’t enter prevention of mad-cow disease, to be officially diagnosed with BSE. termination is made on all BSE- food chain. they are hopeful this is only an iso- The cow, upon being con- suspect animals. -

Introduction Remove the Udder Removing the Pizzle (Penis)
fig . removing the udder, cut outwards through the skin fig 2. removing the pizzle Introduction This guide describes the carcass dressing procedures either side of the pizzle joining the cuts around the that are ideally carried out in a deer larder, after back of the scrotum. Continue the single central cut the gralloch has been performed in the field. The through the skin almost to the anus, taking care not Gralloch guide should be considered essential to damage the haunches. Pull the pizzle free where it companion reading. Both are linked to the Carcass runs over the pelvis, cutting the blood vessels. Use Inspection, Carcass Transport, Basic Hygiene, and the knife to free the pizzle where it turns forward Larder guides. inside the “V” of the pelvis. Leave outside the carcass (draped down the back if the carcass is suspended). Remove the udder It will be removed with the aitch bone, bladder, Fig 1. This is best done in the larder but a large udder remainder of the rectum and anus, later. can prevent access to the rear end and may have to be removed in the field before opening the stomach. Split the aitch bone Pinch the skin just in front of the udder and pulling Figs 3. and 4. Note that some venison processors on it all the time, cut around the udder, removing it would prefer that the aitch bone remains intact, whole, with the skin. Do not take the cut any further check before cutting. While causing the least possible rearwards until back in the larder. -
Instruction Manual for Citizen Digital Forehead And
INSTRUCTION MANUAL Symbol Explanations Measuring body temperature (temperature detection) Remove the probe cap and check the probe tip. FOR CITIZEN DIGITAL Refer to instruction manual before use. How to measure correctly in the ear measurement mode * When using it for the first time, open the FOREHEAD AND EAR battery cap and remove the insulation Open the Temperature basics battery cap to THERMOMETER CTD710 Type BF applied part sheet under the battery cap. remove the All objects radiate heat. This device consists of a probe with a built-in insulation sheet. infrared sensor that measures body temperature by detecting the heat Thank you very much for purchasing IP22 Classification for water ingress and particulate matter. radiated by the eardrum and surrounding tissue. Figure 4 shows the the CITIZEN digital forehead and ear Keeping the probe window clean tortuous anatomy of a normal ear canal. As shown in Figure 5, hold the thermometer. Warning Probe window ear and gently pull it back at an angle or pull it straight back to straighten out the ear canal. The shape of the ear canal differs from individual, check • Please read all of the information in before measurement. Accurate temperature measurements make it this instruction manual before Caution essential to straighten the ear canal so that the probe tip directly faces operating the device. the eardrum. • Be sure to have this instruction Indicates this device is subject to the Waste Electrical and Dirt in the probe window will impact the accuracy of temperature detection. External auditory manual to hand during use. 1902LA Electronic Equipment Directive in the European Union. -

Getting the Right Diagnosis Seeing Her Enhance the Team’S Quality Tion
Central PA Health Care Quality Unit March 2017 Volume 17, Issue 3 HCQU, M.C. 24-12, 100 N. Academy Ave., Danville, PA 17822 http://www.geisinger.org/hcqu (570) 271-7240 Fax: (570) 271-7241 Welcome to Centre Getting the County’s New HCQU Right Diagnosis Nurse! by Health After 50 | January 19, 2017 Have you ever turned your head and then had the world suddenly start to spin around you? This diz- zying sensation can be both disconcerting and poten- tially dangerous. Losing your equilibrium could cause you to fall and fracture a bone. If you’re an older adult, one likely reason for your dizziness is an inner-ear condition called benign paroxysmal positional vertigo (BPPV). The condition af- Welcome to our new HCQU em- fects up to 10 percent of adults by the time they turn ployee! In December, Marilyn Moser 80, according to researchers at the University of Con- accepted our offer of part time employ- necticut Health Center in a review published in the ment as the Centre County Regional Journal of the American Geriatrics Society. BPPV is re- Nurse for the HCQU replacing recently sponsible for about half the cases of dizziness in older retired Linda Dutrow. Marilyn has adults. eight years of experience in a wide va- As common as BPPV is, some primary care doc- riety of nursing. In her most recent tors may not immediately recognize the condition in position, Marilyn has provided educa- older patients, and diagnosis may be(Continued delayed onor page 5) tion to staff, families and clientele. -

Facial Pressure,Or Shortness of Breath
SINUS PAIN? If You Are Suffering From Headaches, Allergies, Facial Pressure, Or Shortness Of Breath, This Information Guide Might Just Help YOU Find Relief! How Can I Get Instant Lasting Relief From My Sinus Symptoms? SINUS SUFFERERS Find instant relief that lasts. If you suffer from headaches, cough, facial pain or tenderness, lack of energy, nasal congestion and discharge, sore throat and postnasal drip, loss of smell or bad breath, you are not alone. Over 30 million people in the United States each year complain of sinus issues. Sinus infections are one of the most common reasons for a visit to a healthcare provider. One out of five antibiotics in the United States are prescribed for sinus sufferers. Many times prescription drugs, or other methods only give temporary relief from sinus pain. If you’ve tried prescription drugs to relieve your sinus pain, and you are still suffering…you might have what is commonly referred to in medical terms as “sinusitis” If you are looking for a better and quicker way to get long-lasting relief, sinus surgery might be the solution for you. The good news is that you don’t need to suffer any longer. Why? Now, you can instantly solve your sinus issues with an in-office procedure calledBalloon Sinuplasty. You might be saying to yourself, “that sounds great, but what if I’m afraid of surgery?” The great news is that Balloon Sinuplasty is a minimally-invasive procedure that can be done in-office, so there is no need to go to the hospital. Most of the time, there is only minimal discomfort and recovery times are quick (often within 24 hours). -

Ear and Forehead Thermometer
Ear and Forehead Thermometer INSTRUCTION MANUAL Item No. 91807 19.PJN174-14_GA-USA_HHD-Ohrthermometer_DSO364_28.07.14 Montag, 28. Juli 2014 14:37:38 USAD TABLE OF CONTENTS No. Topic Page 1.0 Definition of symbols 5 2.0 Application and functionality 6 2.1 Intended use 6 2.2 Field of application 7 3.0 Safety instructions 7 3.1 General safety instructions 7 3.3 Environment for which the DSO 364 device is not suited 9 3.4 Usage by children and adolescents 10 3.5 Information on the application of the device 10 4.0 Questions concerning body temperature 13 4.1 What is body temperature? 13 4.2 Advantages of measuring the body tempera- ture in the ear 14 4.3 Information on measuring the body tempera- ture in the ear 15 5.0 Scope of delivery / contents 16 6.0 Designation of device parts 17 7.0 LCD display 18 8.0 Basic functions 19 8.1 Commissioning of the device 19 8.2 Warning indicator if the body temperature is 21 too high 2 19.PJN174-14_GA-USA_HHD-Ohrthermometer_DSO364_28.07.14 Montag, 28. Juli 2014 14:37:38 TABLE OF CONTENTS USA No. Topic Page 8.3 Backlighting / torch function 21 8.4 Energy saving mode 22 8.5 Setting °Celsius / °Fahrenheit 22 9.0 Display / setting time and date 23 9.1 Display of time and date 23 9.2 Setting time and date 23 10.0 Memory mode 26 11.0 Measuring the temperature in the ear 28 12.0 Measuring the temperature on the forehead 30 13.0 Object temperature measurement 32 14.0 Disposal of the device 33 15.0 Battery change and information concerning batteries 33 16.0 Cleaning and care 36 17.0 “Cleaning” warning indicator 37 18.0 Calibration 38 19.0 Malfunctions 39 20.0 Technical specification 41 21.0 Warranty 44 3 19.PJN174-14_GA-USA_HHD-Ohrthermometer_DSO364_28.07.14 Montag, 28. -

View of Urothelial and Metastatic Carcinoma Including Clinical Presentation, Diagnostic Testing, Treatment and Chiropractic Considerations Is Discussed
Daniels et al. Chiropractic & Manual Therapies (2016) 24:14 DOI 10.1186/s12998-016-0097-8 CASE REPORT Open Access Bladder metastasis presenting as neck, arm and thorax pain: a case report Clinton J. Daniels1,2,3*, Pamela J. Wakefield1,2 and Glenn A. Bub1,2 Abstract Background: A case of metastatic carcinoma secondary to urothelial carcinoma presenting as musculoskeletal pain is reported. A brief review of urothelial and metastatic carcinoma including clinical presentation, diagnostic testing, treatment and chiropractic considerations is discussed. Case presentation: This patient presented in November 2014 with progressive neck, thorax and upper extremity pain. Computed tomography revealed a destructive soft tissue mass in the cervical spine and additional lytic lesion of the 1st rib. Prompt referral was made for surgical consultation and medical management. Conclusion: Distant metastasis is rare, but can present as a musculoskeletal complaint. History of carcinoma should alert the treating chiropractic physician to potential for serious disease processes. Keywords: Chiropractic, Neck pain, Transitional cell carcinoma, Bladder cancer, Metastasis, Case report Background serious complication of UC is distant metastasis—with Urothelial carcinoma (UC), also known as transitional higher stage cancer and lymph involvement worsening cell carcinoma (TCC), accounts for more than 90 % of prognosis and cancer survival rate [10]. The 5-year all bladder cancers and commonly metastasizes to the cancer-specific survival rate of UC is estimated to be pelvic lymph nodes, lungs, liver, bones and adrenals or 78 % [10, 11]. brain [1, 2]. The spread of bladder cancer is mainly done Neck pain accounts for 24 % of all disorders seen by via the lymphatic system with the most frequent location chiropractors [12]. -

March 22, 2018
Packer Lambs Steady To Mostly Lower San Angelo slaughter lamb prices were $10-20 lower this week, feeder lambs steady. Goldthwaite wool lambs were $5 lower, light Dorper and Bar- bado lambs $5-10 lower, and medium and heavy hair lambs steady to $5 lower. Hamilton lambs sold steady. Fredericks- burg lambs were $5 lower. VOL. 70 - NO. 11 SAN ANGELO, TEXAS THURSDAY, MARCH 22, 2018 LIVESTOCKWEEKLY.COM $35 PER YEAR Lamb and mutton meat production for the week end- ing March 16 totaled three million pounds on a slaugh- ter count of 40,000 head compared with the previous week’s totals of 3.1 million pounds and 42,000 head. Imported lamb and mutton for the week ending March 10 totaled 2553 metric tons or approximately 5.63 million pounds, equal to 182 percent of domestic production for the same period. San Angelo’s feeder lamb market had medium and large 1-2 newcrop lambs weighing 40-60 pounds at $200-206, 60-90 pounds $192-218, 80- 100 pounds $192-218, oldcrop 60-90 pounds $184-196, and 100-105 pounds $166-172. Fredericksburg No. 1 wool lamb weighing 40-60 pounds were $200-240 and 60-80 pounds $200-230. Hamil- ton Dorper and Dorper cross lambs weighing 20-40 pounds sold for $180-260. Direct trade on feeder lambs last week was limited to Colo- rado, where 400 head weighing SOCIAL WARRIORS may take offense, but males-only 125-135 pounds brought $168. enclaves are still common in the livestock business. San Angelo choice 2-3 Whether bucks, bulls or billies, the Old Boys’ clubs are slaughter lambs weighing Range Sales a fi xture much of the year, giving way only during breed- 110-170 pounds brought ing season, itself a highly non-PC concept. -

The Ear, Nose, and Throat Exam Jeffrey Texiera, MD and Joshua Jabaut, MD CPT, MC, USA LT, MC, USN
The Ear, Nose, and Throat Exam Jeffrey Texiera, MD and Joshua Jabaut, MD CPT, MC, USA LT, MC, USN Midatlantic Regional Occupational and Environmental Medicine Conference Sept. 23, 2017 Disclosures ●We have no funding or financial interest in any product featured in this presentation. The items included are for demonstration purposes only. ●We have no conflicts of interest to disclose. Overview ● Overview of clinically oriented anatomy - presented in the format of the exam ● The approach ● The examination ● Variants of normal anatomy ● ENT emergencies ● Summary/highlights ● Questions Anatomy ● The head and neck exam consists of some of the most comprehensive and complicated anatomy in the human body. ● The ear, nose, and throat comprise a portion of that exam and a focused clinical encounter for an acute ENT complaint may require only this portion of the exam. Ears www.Medscape.com www.taqplayer.info Ear – Vestibular organ www.humanantomylibrary.com Nose/Sinus Anatomy Inferior Middle Turbinate Turbinate Septum Dorsum Sidewalls Ala Floor Tip www.ENT4Students.blogspot.com Columella Vestibule www.beautyepic.com Oral cavity and oropharynx (throat) www.apsubiology.org Neck www.rdhmag.com The Ear, Nose, and Throat exam Perform in a standardized systematic way that works for you Do it the same way every time, this mitigates risk of missing a portion of the exam Practice the exam to increase comfort with performance and familiarize self with variants of normal Describe what you are doing to the patient, describe what you see in your documentation Use your PPE as appropriate A question to keep in mind… ●T/F: The otoscope is the optimal tool for examining the tympanic membrane.