Scurvy, Starvation, and Flea Infestation – a Case Report from 21St Century Europe
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Scurvy Due to Selective Diet in a Seemingly Healthy 4-Year-Old Boy Andrew Nastro, MD,A,G,H Natalie Rosenwasser, MD,A,B Steven P
Scurvy Due to Selective Diet in a Seemingly Healthy 4-Year-Old Boy Andrew Nastro, MD,a,g,h Natalie Rosenwasser, MD,a,b Steven P. Daniels, MD,c Jessie Magnani, MD,a,d Yoshimi Endo, MD,e Elisa Hampton, MD,a Nancy Pan, MD,a,b Arzu Kovanlikaya, MDf Scurvy is a rare disease in developed nations. In the field of pediatrics, it abstract primarily is seen in children with developmental and behavioral issues, fDivision of Pediatric Radiology and aDepartments of malabsorptive processes, or diseases involving dysphagia. We present the Pediatrics and cRadiology, NewYork-Presbyterian/Weill Cornell Medical Center, New York, New York; bDivision of case of an otherwise developmentally appropriate 4-year-old boy who Pediatric Rheumatology and eDepartment of Radiology, developed scurvy after gradual self-restriction of his diet. He initially Hospital for Special Surgery, New York, New York; and d presented with a limp and a rash and was subsequently found to have anemia Division of Neonatal-Perinatal Medicine, University of Michigan, Ann Arbor, Michigan gDepartment of Pediatrics, and hematuria. A serum vitamin C level was undetectable, and after review of NYU School of Medicine, New York, New York hDepartment of the MRI of his lower extremities, the clinical findings supported a diagnosis of Pediatrics, Bellevue Hospital Center, New York, New York scurvy. Although scurvy is rare in developed nations, this diagnosis should be Dr Nastro helped conceptualize the case report, considered in a patient with the clinical constellation of lower-extremity pain contributed to writing the introduction, initial presentation, hospital course, and discussion, and or arthralgias, a nonblanching rash, easy bleeding or bruising, fatigue, and developed the laboratory tables while he was anemia. -

Infantile Scurvy: Its History
Arch Dis Child: first published as 10.1136/adc.10.58.211 on 1 August 1935. Downloaded from INFANTILE SCURVY: ITS HISTORY BY G. F. STILL, M.D., F.R.C.P. Consulting Physician to the Hospital for Sick Children, Great Ormond Street. As early as the sixteenth century and still more in the seventeenth century the clinical picture of scurvy was acquring a distinctness which it had never had before in the minds of medical men. In 1534 Euricius Cordus, a physician of eminence, as well as a poet, had written on the scurvy, and five years later the Professor of Medicine (and of Greek !) at the University of Ingolstadt, Johannes Agricola, devoted part of his writings to this subject. There is no reason to assume that scurvy came into existence at that time; indeed, it is quite certain that it must have occurred as soon as man discovered ways of subsisting without fresh meat and milk and the fruits of the earth, and especially when his journeyings by sea became extended so that he was more dependent upon long- preserved foods. Writers in the seventeenth century-which was particularly prolific in works on scurvy-still anxious to maintain the Hippocratic tradition, were at pains to show that Hippocrates had referred to scurvy, without naming it, as an affection of the gums or mouth associated with enlargement of the spleen, and that Galen, more explicitly, had described it under the names of O-ro/LaKa'Ky and o-_KEkTUvp/i1, by emphasizing the oral manifestations and the weakness and difficulty in walking due to that http://adc.bmj.com/ affection: and they had no doubt that Pliny had meant scurvy when he described (Nat. -

Maternal Vitamin Deficiencies Causing Bone Disorders and Fractures in Infants
Colin R Paterson et al. Medical Research Archives vol 7 issue 10. Medical Research Archives RESEARCH ARTICLE Maternal vitamin deficiencies causing bone disorders and fractures in infants Authors Colin R Paterson Formerly Reader in Medicine, University of Dundee, UK Elspeth C Paterson Fellow of the Royal College of Obstetricians and Gynaecologists, UK Correspondence: Dr Colin Paterson, Temple Oxgates, Longforgan, Dundee DD2 5HS, Scotland Email: [email protected] Abstract Recent publications have again drawn attention to long bone fractures in newborn infants with severe vitamin D deficiency due to maternal subnutrition. This is a reminder of the complete dependence of an infant on maternal nutrition; the bones that fracture in early infancy are formed during gestation. This review covers previous reports of congenital rickets including the difficulties in diagnosis, not least because there may be none of the usual radiological hallmarks of rickets. It also outlines ways of making a retrospective diagnosis of vitamin D deficiency after the infant’s biochemical findings have become normal. It is likely that similar considerations apply to vitamin C deficiency. Although overt scurvy is uncommon it is clear that vitamin C subnutrition is widespread even in Western countries. Vitamin C has many roles but among them is its requirement in the formation of collagen. Thus it is not surprising that fractures and intracranial bleeding are well-recognised features of vitamin C deficiency. Maternal subnutrition of vitamin D and vitamin C are important conditions in the wide differential diagnosis of unexplained fractures and fracture-like lesions in infancy. Keywords: Rickets, Scurvy, Vitamin D deficiency, Vitamin C deficiency , Fractures, Non- accidental injury, Classical metaphyseal lesions, Congenital vitamin deficiencies Copyright 2019 KEI Journals. -

PELLAGRA and Its Prevention and Control in Major Emergencies ©World Health Organization, 2000
WHO/NHD/00.10 Original: English Distr.: General PELLAGRA and its prevention and control in major emergencies ©World Health Organization, 2000 This document is not a formal publication of the World Health Organization (WHO), and all rights are reserved by the Organization. The document may, however, be freely reviewed, abstracted, quoted, reproduced or translated, in part or in whole, but not for sale or for use in conjunction with commercial purposes. The views expressed in documents by named authors are solely the responsibility of those authors. Acknowledgements The Department of Nutrition for Health and Development wishes to thank the many people who generously gave of their time to comment on an earlier draft version of this document. Thanks are due in particular to Rita Bhatia (United Nations High Commission for Refugees), Andy Seal (Centre for International Child Health, Institute of Child Health, London), and Ken Bailey, formerly of the Department of Nutrition for Health and Development; their suggestions are reflected herein. In addition, Michael Golden (University of Aberdeen, Scotland) provided inputs with regard to the Angola case study; Jeremy Shoham (London School of Hygiene and Tropical Medicine) completed and updated the draft version and helped to ensure the review’s completeness and technical accuracy; and Anne Bailey and Ross Hempstead worked tirelessly to prepare the document for publication. This review was prepared by Zita Weise Prinzo, Technical Officer, Department of Nutrition for Health and Development. i Contents -

Scurvy May Occur Even in Children with No Underlying Risk Factors
Gallizzi et al. Journal of Medical Case Reports (2020) 14:18 https://doi.org/10.1186/s13256-020-2341-z CASE REPORT Open Access Scurvy may occur even in children with no underlying risk factors: a case report Romina Gallizzi*, Mariella Valenzise, Stefano Passanisi, Giovanni Battista Pajno, Filippo De Luca and Giuseppina Zirilli Abstract Background: Since ancient times, scurvy has been considered one of the most fearsome nutritional deficiency diseases. In modern developed countries, this condition has become very rare and is only occasionally encountered, especially in the pediatric population. Underlying medical conditions, such as neuropsychiatric disorders, anorexia nervosa, celiac disease, Crohn disease, hemodialysis, and severe allergies to food products may enhance the risk of developing scurvy. Case presentation: We report the case of an otherwise healthy 3-year-old white boy who developed scurvy due to a selective restrictive diet derived from his refusal to try new food. He presented to our clinic with asthenia and refusal to walk. During hospitalization he developed severe anemia and hematochezia. A diagnosis of scurvy was assessed on the basis of nutritional history, clinical features, radiographic findings, and laboratory findings. Supplementation of ascorbic acid enabled a prompt resolution of symptoms. Conclusions: Scurvy is caused by vitamin C deficiency. Cutaneous bleeding, mucosal bleeding, and anemia represent typical manifestations of the disease. These symptoms are directly connected to ascorbic acid involvement in collagen biosynthesis. Some radiographic findings can be useful for the diagnosis. Treatment aims to normalize serum levels of vitamin C in order to counteract the deprivation symptoms. The present case report demonstrates that scurvy may sporadically occur in pediatric patients, even in individuals with no predisposing medical conditions and/or potential risk factors. -

MENT of SCURVY, Quickly the Active Tendency May Be Abolished
811 lumbar segments of the cord. Major Jones states that this of germinated beans which had weighed 4 oz. in the dry distribution of hypersesthesia is found in malaria and trench state, half being taken at dinner and half at tea. In fever, and in no other disease. If these findings are con- respect of other forms of treatment, such as tonics and local firmed it may be of great help in the diagnosis of these treatment to the mouth, no difference was made between the chronic subjects of trench fever, who are apt sometimes to two wards. be considered as " lead swingers " or, at least, exaggerators, A certain amount of prejudice against the beans had to be when they are really suffering from a definite and disabling contended with. Though perfectly good to eat, it cannot be condition. said that they always looked appetising, and some with a The question of how long this chronic trench fever may datk husk had a disagreeable sour taste. These dis- last cannot yet be settled. The longest duration that I have advantages might have been masked by mixing the beans yet noticed is a little over one year, but it is probable that it in a general stew, but it was thought better to serve them may go on for much longer than this. Patients are usually apart in order to ensure some accuracy of dosage and that in with various not very ill-only low general health, pains-I the cooking should be limited to the shortest possible time. and so they are soon transferred to a convalescent camp, or Apparently, however, the greatest difficulty was based on put in low categories, where their slight fever is apt to be the fact that these beans are regarded as pig food by some overlooked. -

Scurvy Due to Selective Diet in a Seemingly Healthy 4-Year-Old Boy Andrew Nastro, MD,A,G,H Natalie Rosenwasser, MD,A,B Steven P
Scurvy Due to Selective Diet in a Seemingly Healthy 4-Year-Old Boy Andrew Nastro, MD,a,g,h Natalie Rosenwasser, MD,a,b Steven P. Daniels, MD,c Jessie Magnani, MD,a,d Yoshimi Endo, MD,e Elisa Hampton, MD,a Nancy Pan, MD,a,b Arzu Kovanlikaya, MDf Scurvy is a rare disease in developed nations. In the field of pediatrics, it abstract primarily is seen in children with developmental and behavioral issues, fDivision of Pediatric Radiology and aDepartments of malabsorptive processes, or diseases involving dysphagia. We present the Pediatrics and cRadiology, NewYork-Presbyterian/Weill Cornell Medical Center, New York, New York; bDivision of case of an otherwise developmentally appropriate 4-year-old boy who Pediatric Rheumatology and eDepartment of Radiology, developed scurvy after gradual self-restriction of his diet. He initially Hospital for Special Surgery, New York, New York; and d presented with a limp and a rash and was subsequently found to have anemia Division of Neonatal-Perinatal Medicine, University of Michigan, Ann Arbor, Michigan gDepartment of Pediatrics, and hematuria. A serum vitamin C level was undetectable, and after review of NYU School of Medicine, New York, New York hDepartment of the MRI of his lower extremities, the clinical findings supported a diagnosis of Pediatrics, Bellevue Hospital Center, New York, New York scurvy. Although scurvy is rare in developed nations, this diagnosis should be Dr Nastro helped conceptualize the case report, considered in a patient with the clinical constellation of lower-extremity pain contributed to writing the introduction, initial presentation, hospital course, and discussion, and or arthralgias, a nonblanching rash, easy bleeding or bruising, fatigue, and developed the laboratory tables while he was anemia. -

Thiamine Deficiency and Its Prevention and Control in Major Emergencies ©World Health Organization, 1999
WHO/NHD/99.13 Original: English Distr: General Thiamine deficiency and its prevention and control in major emergencies ©World Health Organization, 1999 This document is not a formal publication of the World Health Organization (WHO), and all rights are reserved by the Organization. The document may, however, be freely reviewed, abstracted, quoted, reproduced or translated, in part or in whole, but not for sale or for use in conjunction with commercial purposes. The views expressed in documents by named authors are solely the responsibility of those authors. Acknowledgements The Department of Nutrition for Health and Development of the World Health Organization (WHO), wishes to thank all those who generously gave their time to comment on an earlier draft version, especially Rita Bhatia, United Nations High Commission for Refugees (UNHCR), Andy Seal, Centre for International Child Health, Institute of Child Health (ICH), London, and Kenneth Bailey from the Department of Nutrition for Health and Development, WHO, whose suggestions are reflected herein. Grateful acknowledgement is due to Professor Prakash S. Shetty, Head, Public Health Nutrition Unit, Department of Epidemiology & Population Health, London School of Hygiene and Tropical Medicine, for his tireless efforts to ensure the review’s completeness and technical accuracy and also to Carol Aldous for preparing the document for publication. This review was prepared by Zita Weise Prinzo, Technical Officer, in WHO’s Department of Nutrition for Health and Development. i Contents Acknowledgements ...........................................i List of Tables and Figures .....................................vi Thiamine deficiency: Definition .................................ix Introduction ................................................. 1 Scope ....................................................... 1 Background .................................................. 1 Recent outbreaks of thiamine deficiency ............................ 1 In the general population ................................... -

Unexpected Scurvy Presenting with Proptosis: a Case Report Jelvin T
The Medical City Journal © 2018 Case Report Unexpected Scurvy Presenting with Proptosis: A Case Report Jelvin T. Co*, Timothy Joseph S. Orillaza and Romelito Jose G. Galsim Department of Radiology, The Medical City, Ortigas Avenue, Pasig City * Contact Details: [email protected] ABSTRACT: Scurvy is a state of dietary deficiency of ascorbic acid, or vitamin C as it is more commonly known. Since the discovery of the link between scurvy and vitamin C, it has become a rare condition. We present a 5 y.o. Filipino female with proptosis. An intraorbital neoplastic process was primarily entertained. Only after magnetic resonance imaging (MRI) revealed bilateral supraorbital subperiosteal hematoma formation was scurvy considered and empiric treatment of vitamin C supplementation started, yielding significant improvement. Given the multiple tools that we have in the information age, MRI plays a role in helping diagnose an easily treatable condition. Keywords: hemorrhage, MRI, proptosis, scurvy INTRODUCTION The patient’s birth, past medical, developmental and Since the discovery of the link between scurvy and vi- personal/social histories were unremarkable. The patient’s tamin C deficiency, scurvy has become an uncommon con- feeding history was noted to be completely deficient in dition in all age groups1. Cases of scurvy may still be found fruits and vegetables, with note of vomiting when eating the in industrialized societies, frequently among the extreme latter. Pertinent physical examination of the patient revealed ages of the population2. The initial presenting features of bilateral proptosis with tenderness, generalized abdominal scurvy are nonspecific, ranging from fatigue to musculoske- pain, gum swelling and body weakness. -

Degrees of Scurvy As Well As Rickets Are to Be Seen in Bottle-Fed Children
386 SPECIAL ARTICLE: MEDICINE IN CANADIAN ARCrIC Canad. M. A. J. Sept. 1, 1959, vol. 81 N.W.T. One would expect vitamin C deficiency to be prevalent in the North, since so many Arctic explorers died of scurvy, but it is actually never seen in people eating adequate amounts of fresh MEDICAL OBSERVATIONS AND meat. Slight degrees, manifested as ready bleeding PROBLEMS IN THE of the gums, occur occasionally after periods of CANADIAN ARCTIC* relative scarcity of fresh meat. Despite the long dark winters and inadequate ultraviolet radiation OTTO SCHAEFER, M.D.,t Edmonton, at all times, vitamin D deficiencies do not occur in Alta. Arctic peoples who live predominantly on native PART II food and whose children are breast-fed. Severe degrees of scurvy as well as rickets are to be seen NUTRITION AND NUTRITIONAL DEFICIENCIES in bottle-fed children, who are not given vitamin EsKIMos as well as Northern Indians used to live, supplements. as hunters on a diet consisting almost exclusively We had an orphan girl in Pangnirtung, who was of meat, fsh and fat. The only source of carbo- reared by the missionary's wife on powdered milk hydrates of practical importance was large amounts 25 years ago. The girl ended up with a rachitic of berries collected by their women and children in contracted pelvis. I had eventually to deliver her the short sinmers. Indians used to dry enough large first son by Cesarean section, the first berries for an all-year-round supply of this im- Eskimo-to my knowledge-born that way within portant vitamin and mineral source, while Eskimos the Arctic, under most trying conditions. -
Scurvy Masquerading As Reactive Arthritis
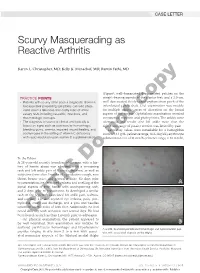
CASE LETTER Scurvy Masquerading as Reactive Arthritis Karen L. Christopher, MD; Kelly K. Menachof, MD; Ramin Fathi, MD (Figure); well-demarcated desquamated patches on the PRACTICE POINTS weight-bearing aspects of the plantar feet; and a 2.0-cm, • Patients with scurvy often pose a diagnostic dilemma well-demarcated, thinly raised erythematous patch of the because their presenting symptoms can lead physi- inferolateral penile shaft. Oralcopy examination was notable cians down a laborious and costly road of unnec- for multiple discrete areas of ulceration on the lateral essary tests including vasculitic, infectious, and aspects of the tongue. Ophthalmic examination revealed rheumatologic workups. conjunctival injection and photophobia. The ankles were • The diagnosis of scurvy is clinical and typically is edematous and tender (the left ankle more than the based on signs such as perivascular hemorrhage, right), and range of passive motion was limited by pain. bleeding gums, anemia, impaired wound healing, and Laboratory values were remarkable for a hemoglobin ecchymoses in the setting of vitamin C deficiency count of 13.1 g/dL (reference range, 14.2–18 g/dL), erythrocyte with rapid resolution upon vitamin C supplementation. not sedimentation rate of 31 mm/h (reference range, 0–10 mm/h), To the Editor: Do A 28-year-old recently homeless white man with a his- tory of heroin abuse was admitted with a worsening rash and left ankle pain of 1 week’s duration, as well as subjective fever after 3 weeks of a productive cough, sore throat, hoarse voice, and general malaise. Six days prior to presentation, he developed redness and swelling of the A dorsal aspects of both hands with accompanying rash, and 2 days prior to presentation he developed a similar rash on the legs with associated left ankle pain, redness, and swelling. -

Meeting the Challenges of Micronutrient Deficiencies in Emergency-Affected Populations
Proceedings of the Nutrition Society (2002), 61, 251-257 DOL10.1079/PNS2002151 © The Authors 2002 Meeting the challenges of micronutrient deficiencies in emergency-affected populations Z. Weise Prinzo* and B. de Benoist Department of Nutrition for Health and Development, World Health Organization, 1211 Geneva 27, Switzerland Micronutrient deficiencies occur frequently in refugee and displaced populations. These deficiency diseases include, in addition to the most common Fe and vitamin A deficiencies, scurvy (vitamin C deficiency), pellagra (niacin and/or tryptophan deficiency) and beriberi (thiamin deficiency), which are not seen frequently in non-emergency-affected populations. The main causes of the outbreaks have been inadequate food rations given to populations dependent on food aid. There is no universal solution to the problem of micronutrient deficiencies, and not all interventions to prevent the deficiency diseases are feasible in every emergency setting. The preferred way of preventing these micronutrient deficiencies would be by securing dietary diversification through the provision of vegetables, fruit and pulses, which may not be a feasible strategy, especially in the initial phase of a relief operation. The one basic emergency strategy has been to include a fortified blended cereal in the ration of all food-aid-dependent populations (United Nations High Commissioner for Refugees/World Food Programme, 1997). In situations where the emergency-affected population has access to markets, recommendations have been to increase the general ration to encourage the sale and/or barter of a portion of the ration in exchange for locally-available fruit and vegetables (World Health Organization, 1999a,b, 2000). Promotion of home gardens as well as promotion of local trading are recommended longer-term options aiming at the self-sufficiency of emergency-affected households.