Neuroscience Based Nomenclature - Nbn Glossary*
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Treatment of Psychosis: 30 Years of Progress
Journal of Clinical Pharmacy and Therapeutics (2006) 31, 523–534 REVIEW ARTICLE Treatment of psychosis: 30 years of progress I. R. De Oliveira* MD PhD andM.F.Juruena MD *Department of Neuropsychiatry, School of Medicine, Federal University of Bahia, Salvador, BA, Brazil and Department of Psychological Medicine, Institute of Psychiatry, King’s College, University of London, London, UK phrenia. Thirty years ago, psychiatrists had few SUMMARY neuroleptics available to them. These were all Background: Thirty years ago, psychiatrists had compounds, today known as conventional anti- only a few choices of old neuroleptics available to psychotics, and all were liable to cause severe extra them, currently defined as conventional or typical pyramidal side-effects (EPS). Nowadays, new antipsychotics, as a result schizophrenics had to treatments are more ambitious, aiming not only to suffer the severe extra pyramidal side effects. improve psychotic symptoms, but also quality of Nowadays, new treatments are more ambitious, life and social reinsertion. We briefly but critically aiming not only to improve psychotic symptoms, outline the advances in diagnosis and treatment but also quality of life and social reinsertion. Our of schizophrenia, from the mid 1970s up to the objective is to briefly but critically review the present. advances in the treatment of schizophrenia with antipsychotics in the past 30 years. We conclude DIAGNOSIS OF SCHIZOPHRENIA that conventional antipsychotics still have a place when just the cost of treatment, a key factor in Up until the early 1970s, schizophrenia diagnoses poor regions, is considered. The atypical anti- remained debatable. The lack of uniform diagnostic psychotic drugs are a class of agents that have criteria led to relative rates of schizophrenia being become the most widely used to treat a variety of very different, for example, in New York and psychoses because of their superiority with London, as demonstrated in an important study regard to extra pyramidal symptoms. -

Dopamine D2 Receptor Occupancy by Perospirone: a Positron Emission Tomography Study in Patients with Schizophrenia and Healthy Subjects
Psychopharmacology (2010) 209:285–290 DOI 10.1007/s00213-010-1783-1 ORIGINAL INVESTIGATION Dopamine D2 receptor occupancy by perospirone: a positron emission tomography study in patients with schizophrenia and healthy subjects Ryosuke Arakawa & Hiroshi Ito & Akihiro Takano & Masaki Okumura & Hidehiko Takahashi & Harumasa Takano & Yoshiro Okubo & Tetsuya Suhara Received: 3 September 2009 /Accepted: 18 January 2010 /Published online: 27 March 2010 # Springer-Verlag 2010 Abstract striatum of healthy subjects was 74.8% at 1.5 h, 60.1% at Rationale Perospirone is a novel second-generation antipsy- 8 h, and 31.9% at 25.5 h after administration. chotic drug with high affinity to dopamine D2 receptor and Conclusion Sixteen milligrams of perospirone caused over short half-life of plasma concentration. There has been no 70% dopamine D2 receptor occupancy near its peak level, investigation of dopamine D2 receptor occupancy in patients and then occupancy dropped to about half after 22 h. The with schizophrenia and the time course of occupancy by time courses of receptor occupancy and plasma concentra- antipsychotics with perospirone-like properties. tion were quite different. This single dosage may be Objective We investigated dopamine D2 receptor occupan- sufficient for the treatment of schizophrenia and might be cy by perospirone in patients with schizophrenia and the useful as a new dosing schedule choice. time course of occupancy in healthy subjects. Materials and methods Six patients with schizophrenia Keywords Dopamine D2 receptor occupancy. taking 16–48 mg/day of perospirone participated. Positron Perospirone . Positron emission tomography . emission tomography (PET) scans using [11C]FLB457 were Schizophrenia . Time course performed on each subject, and dopamine D2 receptor occupancies were calculated. -
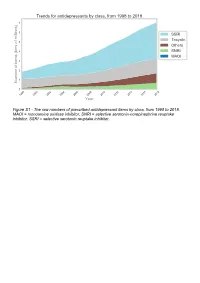
The Raw Numbers of Prescribed Antidepressant Items by Class, from 1998 to 2018
Figure S1 - The raw numbers of prescribed antidepressant items by class, from 1998 to 2018. MAOI = monoamine oxidase inhibitor, SNRI = selective serotonin-norepinephrine reuptake inhibitor, SSRI = selective serotonin reuptake inhibitor. Figure S2 - The raw numbers of prescribed antidepressant items for the ten most commonly prescribed antidepressants (in 2018), from 1998 to 2018. Figure S3 - Practice level percentile charts for the proportions of the ten most commonly prescribed antidepressants (in 2018), prescribed between August 2010 and November 2019. Deciles are in blue, with median shown as a heavy blue line, and extreme percentiles are in red. Figure S4 - Practice level percentile charts for the proportions of specific MAOIs prescribed between August 2010 and November 2019. Deciles are in blue, with median shown as a heavy blue line, and extreme percentiles are in red. Figure S5 - CCG level heat map for the percentage proportions of MAOIs prescribed between December 2018 and November 2019. MAOI = monoamine oxidase inhibitor. Figure S6 - CCG level heat maps for the percentage proportions of paroxetine, dosulepin, and trimipramine prescribed between December 2018 and November 2019. Table S1 - Antidepressant drugs, by category. MAOI = monoamine oxidase inhibitor, SNRI = selective serotonin-norepinephrine reuptake inhibitor, SSRI = selective serotonin reuptake inhibitor. Class Drug MAOI Isocarboxazid, moclobemide, phenelzine, tranylcypromine SNRI Duloxetine, venlafaxine SSRI Citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, -

Revision of Precautions Asenapine Maleate, Aripiprazole, Olanzapine
Published by Translated by Ministry of Health, Labour and Welfare Pharmaceuticals and Medical Devices Agency This English version is intended to be a reference material to provide convenience for users. In the event of inconsistency between the Japanese original and this English translation, the former shall prevail. Revision of Precautions Asenapine maleate, aripiprazole, olanzapine, quetiapine fumarate, clocapramine hydrochloride hydrate, chlorpromazine hydrochloride, chlorpromazine hydrochloride/promethazine hydrochloride/phenobarbital, chlorpromazine phenolphthalinate, spiperone, zotepine, timiperone, haloperidol, paliperidone, pipamperone hydrochloride, fluphenazine decanoate, fluphenazine maleate, brexpiprazole, prochlorperazine maleate, prochlorperazine mesilate, Pharmaceuticals and Medical Devices Agency Office of Safety I 3-3-2 Kasumigaseki, Chiyoda-ku, Tokyo 100-0013 Japan E-mail: [email protected] Published by Translated by Ministry of Health, Labour and Welfare Pharmaceuticals and Medical Devices Agency This English version is intended to be a reference material to provide convenience for users. In the event of inconsistency between the Japanese original and this English translation, the former shall prevail. propericiazine, bromperidol, perphenazine, perphenazine hydrochloride, perphenazine fendizoate, perphenazine maleate, perospirone hydrochloride hydrate, mosapramine hydrochloride, risperidone (oral drug), levomepromazine hydrochloride, levomepromazine maleate March 27, 2018 Non-proprietary name Asenapine maleate, -

Fatal Toxicity of Antidepressant Drugs in Overdose
BRITISH MEDICAL JOURNAL VOLUME 295 24 OCTOBER 1987 1021 Br Med J (Clin Res Ed): first published as 10.1136/bmj.295.6605.1021 on 24 October 1987. Downloaded from PAPERS AND SHORT REPORTS Fatal toxicity of antidepressant drugs in overdose SIMON CASSIDY, JOHN HENRY Abstract dangerous in overdose, thus meriting investigation of their toxic properties and closer consideration of the circumstances in which A fatal toxicity index (deaths per million National Health Service they are prescribed. Recommendations may thus be made that prescriptions) was calculated for antidepressant drugs on sale might reduce the number offatalities. during the years 1975-84 in England, Wales, and Scotland. The We used national mortality statistics and prescription data tricyclic drugs introduced before 1970 had a higher index than the to compile fatal toxicity indices for the currently available anti- mean for all the drugs studied (p<0-001). In this group the depressant drugs to assess the comparative safety of the different toxicity ofamitriptyline, dibenzepin, desipramine, and dothiepin antidepressant drugs from an epidemiological standpoint. Owing to was significantly higher, while that ofclomipramine, imipramine, the nature of the disease these drugs are particularly likely to be iprindole, protriptyline, and trimipramine was lower. The mono- taken in overdose and often cause death. amine oxidase inhibitors had intermediate toxicity, and the antidepressants introduced since 1973, considered as a group, had significantly lower toxicity than the mean (p<0-001). Ofthese newer drugs, maprotiline had a fatal toxicity index similar to that Sources ofinformation and methods of the older tricyclic antidepressants, while the other newly The statistical sources used list drugs under their generic and proprietary http://www.bmj.com/ introduced drugs had lower toxicity indices, with those for names. -

Association of Selective Serotonin Reuptake Inhibitors with the Risk for Spontaneous Intracranial Hemorrhage
Supplementary Online Content Renoux C, Vahey S, Dell’Aniello S, Boivin J-F. Association of selective serotonin reuptake inhibitors with the risk for spontaneous intracranial hemorrhage. JAMA Neurol. Published online December 5, 2016. doi:10.1001/jamaneurol.2016.4529 eMethods 1. List of Antidepressants for Cohort Entry eMethods 2. List of Antidepressants According to the Degree of Serotonin Reuptake Inhibition eMethods 3. Potential Confounding Variables Included in Multivariate Models eMethods 4. Sensitivity Analyses eFigure. Flowchart of Incident Antidepressant (AD) Cohort Definition and Case- Control Selection eTable 1. Crude and Adjusted Rate Ratios of Intracerebral Hemorrhage Associated With Current Use of SSRIs Relative to TCAs eTable 2. Crude and Adjusted Rate Ratios of Subarachnoid Hemorrhage Associated With Current Use of SSRIs Relative to TCAs eTable 3. Crude and Adjusted Rate Ratios of Intracranial Extracerebral Hemorrhage Associated With Current Use of SSRIs Relative to TCAs. eTable 4. Crude and Adjusted Rate Ratios of Intracerebral Hemorrhage Associated With Current Use of Antidepressants With Strong Degree of Inhibition of Serotonin Reuptake Relative to Weak eTable 5. Crude and Adjusted Rate Ratios of Subarachnoid Hemorrhage Associated With Current Use of Antidepressants With Strong Degree of Inhibition of Serotonin Reuptake Relative to Weak eTable 6. Crude and Adjusted Rate Ratios of Intracranial Extracerebral Hemorrhage Associated With Current Use of Antidepressants With Strong Degree of Inhibition of Serotonin Reuptake Relative to Weak This supplementary material has been provided by the authors to give readers additional information about their work. © 2016 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/ on 10/02/2021 eMethods 1. -

Antipsychotics
The Fut ure of Antipsychotic Therapy (page 7 in syllabus) Stepp,,hen M. Stahl, MD, PhD Adjunct Professor, Department of Psychiatry Universityyg of California, San Diego School of Medicine Honorary Visiting Senior Fellow, Cambridge University, UK Sppyonsored by the Neuroscience Education Institute Additionally sponsored by the American Society for the Advancement of Pharmacotherapy This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. Copyright © 2011 Neuroscience Education Institute. All rights reserved. Individual Disclosure Statement Faculty Editor / Presenter Stephen M. Stahl, MD, PhD, is an adjunct professor in the department of psychiatry at the University of California, San Diego School of Medicine, and an honorary visiting senior fellow at the University of Cambridge in the UK. Grant/Research: AstraZeneca, BioMarin, Dainippon Sumitomo, Dey, Forest, Genomind, Lilly, Merck, Pamlab, Pfizer, PGxHealth/Trovis, Schering-Plough, Sepracor/Sunovion, Servier, Shire, Torrent Consultant/Advisor: Advent, Alkermes, Arena, AstraZeneca, AVANIR, BioMarin, Biovail, Boehringer Ingelheim, Bristol-Myers Squibb, CeNeRx, Cypress, Dainippon Sumitomo, Dey, Forest, Genomind, Janssen, Jazz, Labopharm, Lilly, Lundbeck, Merck, Neuronetics, Novartis, Ono, Orexigen, Otsuka, Pamlab, Pfizer, PGxHealth/Trovis, Rexahn, Roche, Royalty, Schering-Plough, Servier, Shire, Solvay/Abbott, Sunovion/Sepracor, Valeant, VIVUS, Speakers Bureau: Dainippon Sumitomo, Forest, Lilly, Merck, Pamlab, Pfizer, Sepracor/Sunovion, Servier, Wyeth Copyright © 2011 Neuroscience Education Institute. All rights reserved. Learninggj Objectives • Differentiate antipsychotic drugs from each other on the basis of their pharmacological mechanisms and their associated therapeutic and side effects • Integrate novel treatment approaches into clinical practice according to best practices guidelines • Identify novel therapeutic options currently being researched for the treatment of schizophrenia Copyright © 2011 Neuroscience Education Institute. -

Prolactin Levels in Schizophrenic Patients Receiving Perospirone in Comparison to Risperidone
J Pharmacol Sci 91, 259 – 262 (2003) Journal of Pharmacological Sciences ©2003 The Japanese Pharmacological Society Short Communication Prolactin Levels in Schizophrenic Patients Receiving Perospirone in Comparison to Risperidone Takashi Togo1,2,*, Eizo Iseki2, Mika Shoji1, Ikuo Oyama1, Akihiko Kase1, Hirotake Uchikado2, Omi Katsuse2 and Kenji Kosaka2 1Yokohama Maioka Hospital, Yokohama 244-0813, Japan 2Department of Psychiatry, Yokohama City University School of Medicine, Yokohama 236-0004, Japan Received November 21, 2002; Accepted January 9, 2003 Abstract. Serum prolactin levels were investigated in 41 patients with schizophrenia who were receiving clinically effective doses of perospirone or risperidone for more than 4 weeks. In order to determine baseline prolactin levels, blood samples were obtained in the morning, 10 – 14 h after antipsychotic medication. Median levels were within normal limits in both female and male patients receiving perospirone, while risperidone induced significant elevation. These results suggest that in contrast to risperidone, where baseline prolactin levels were elevated 5.3-fold in female and 4.2-fold in male patients, baseline prolactin levels are not elevated after treatment with perospirone. However, these results should be cautiously interpreted, because drug-by-time interaction has previously been reported in antipsychotic-induced hyperprolactinemia. Keywords: prolactin, perospirone, schizophrenia Hyperprolactinemia is a common side effect that may well as the adverse effects of perospirone have not been arise from the use of antipsychotic agents (1, 2). Before fully investigated. In the present study, we have investi- the introduction of clozapine, it was assumed that all gated the baseline serum prolactin levels in patients antipsychotics cause extrapyramidal side effects and treated with clinically effective doses of perospirone in elevate prolactin levels by antagonizing dopamine D2 comparison to risperidone. -
Efficacy and Tolerability of Aripiprazole Versus D2 Antagonists in the Early
www.nature.com/npjschz REVIEW ARTICLE OPEN Efficacy and tolerability of aripiprazole versus D2 antagonists in the early course of schizophrenia: a systematic review and meta-analysis David D. Kim1,2, Alasdair M. Barr1,2, Lulu Lian1, Jessica W. Y. Yuen1, Diane Fredrikson3, William G. Honer2,3, Allen E. Thornton2,4 and ✉ Ric M. Procyshyn 2,3 Early intervention is essential for favorable long-term outcomes in schizophrenia. However, there is limited guidance in the scientific literature on how best to choose between dopamine D2 receptor (D2R) partial agonists and D2R antagonists in early stages of schizophrenia. The aim of this meta-analysis was to directly compare D2R partial agonists with D2R antagonists for efficacy and tolerability, using randomized controlled trials (RCTs) that involved participants diagnosed with first-episode psychosis, schizophrenia, or related psychotic disorders with a duration of illness ≤5 years. Fourteen RCTs, involving 2494 patients, were included in the meta-analysis. Aripiprazole was the only identified D2R partial agonist, and was not significantly different from pooled D2R antagonists for overall symptom reduction or all-cause discontinuation. However, aripiprazole was more favorable than pooled D2R antagonists for depressive symptoms, prolactin levels, and triglyceride levels. Specifically, aripiprazole was more favorable than paliperidone for triglyceride levels and more favorable than risperidone and olanzapine, but less favorable than ziprasidone, for weight gain. In addition, aripiprazole was less favorable for akathisia compared with second-generation D2R 1234567890():,; antagonists, in particular olanzapine and quetiapine, and less favorable for discontinuation due to inefficacy than risperidone. Lastly, aripiprazole was more favorable than haloperidol for various efficacy and tolerability outcomes. -

United States Patent (10 ) Patent No.: US 10,660,887 B2 Javitt (45 ) Date of Patent: *May 26 , 2020
US010660887B2 United States Patent (10 ) Patent No.: US 10,660,887 B2 Javitt (45 ) Date of Patent : *May 26 , 2020 (54 ) COMPOSITION AND METHOD FOR (56 ) References Cited TREATMENT OF DEPRESSION AND PSYCHOSIS IN HUMANS U.S. PATENT DOCUMENTS 6,228,875 B1 5/2001 Tsai et al. ( 71 ) Applicant : Glytech , LLC , Ft. Lee , NJ (US ) 2004/0157926 A1 * 8/2004 Heresco - Levy A61K 31/198 514/561 (72 ) Inventor: Daniel C. Javitt , Ft. Lee , NJ (US ) 2005/0261340 Al 11/2005 Weiner 2006/0204486 Al 9/2006 Pyke et al . 2008/0194631 Al 8/2008 Trovero et al. ( 73 ) Assignee : GLYTECH , LLC , Ft. Lee , NJ (US ) 2008/0194698 A1 8/2008 Hermanussen et al . 2010/0069399 A1 * 3/2010 Gant CO7D 401/12 ( * ) Notice : Subject to any disclaimer, the term of this 514 / 253.07 patent is extended or adjusted under 35 2010/0216805 Al 8/2010 Barlow 2011/0207776 Al 8/2011 Buntinx U.S.C. 154 ( b ) by 95 days . 2011/0237602 A1 9/2011 Meltzer This patent is subject to a terminal dis 2011/0306586 Al 12/2011 Khan claimer . 2012/0041026 A1 2/2012 Waizumi ( 21 ) Appl. No.: 15 /650,912 FOREIGN PATENT DOCUMENTS CN 101090721 12/2007 ( 22 ) Filed : Jul. 16 , 17 KR 2007 0017136 2/2007 WO 2005/065308 7/2005 (65 ) Prior Publication Data WO 2005/079756 9/2005 WO 2011044089 4/2011 US 2017/0312275 A1 Nov. 2 , 2017 WO 2012/104852 8/2012 WO 2005/000216 9/2013 WO 2013138322 9/2013 Related U.S. Application Data (63 ) Continuation of application No. -

New Zealand Data Sheet
1 PARNATE tranylcypromine film-coated tablets 10 mg New Zealand Data Sheet 1 PARNATE® (10 MG FILM-COATED TABLETS) PARNATE 10 mg film-coated tablets. 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Parnate 10 mg film-coated tablets: each tablet contains tranylcypromine sulfate equivalent to 10 mg of tranylcypromine. Excipients with known effect: each tablet contains sucrose 6 mg. For the full list of excipients, see section 6.1. 3 PHARMACEUTICAL FORM Parnate 10 mg film-coated tablets contain "geranium rose" coloured, biconvex, film-coated tablets. 4 CLINICAL PARTICULARS 4.1 Therapeutic indications Parnate is indicated for the treatment of symptoms of depressive illness especially where treatment with other types of anti-depressants has failed. It is not recommended for use in mild depressive states resulting from temporary situational difficulties. 4.2 Dose and method of administration Adults Begin with 20 mg a day given as 10 mg in the morning and 10 mg in the afternoon. If there is no satisfactory response after two weeks, add one more tablet at midday. Continue this dosage for at least a week. A dosage of 3 tablets a day should only be exceeded with caution. When a satisfactory response is established, dosage may be reduced to a maintenance level. Some patients will be maintained on 20 mg per day, some will need only 10 mg daily. If no improvement occurs, continued administration is unlikely to be beneficial. 1 2 PARNATE tranylcypromine film-coated tablets 10 mg When given together with a tranquilliser, the dosage of Parnate is not affected. When the medicine is given concurrently with electroconvulsive therapy, the recommended dosage is 10 mg twice a day during the series and 10 mg a day afterwards as maintenance therapy. -

Pharmacology Review(S)
CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 200603 PHARMACOLOGY REVIEW(S) Tertiary Pharmacology/Toxicology Review From: Paul C. Brown, Ph.D., ODE Associate Director for Pharmacology and Toxicology, OND IO NDA: 200603 Agency receipt date: 12/30/2009 Drug: Lurasidone hydrochloride Applicant: Sunovion Pharmaceuticals (Originally submitted by Dainippon Sumimoto Pharma America, Inc.) Indication: schizophrenia Reviewing Division: Division of Psychiatry Products Background: The pharm/tox reviewer and team leader concluded that the nonclinical data support approval of lurasidone for the indication listed above. Reproductive and Developmental Toxicity: Reproductive and developmental toxicity studies in rats and rabbits revealed no evidence of teratogenicity or embryofetal toxicity. The high doses in the rat and rabbit embryofetal toxicity studies were 3 and 12 times, respectively, the maximum recommended human dose (80 mg) based on a body surface area comparison. Carcinogenicity: Lurasidone was tested in 2 year rat and mouse carcinogenicity studies. These studies were reviewed by the division and the executive carcinogenicity assessment committee. The committee concluded that the studies were adequate and that there was a drug-related increase in mammary carcinomas in female rats at doses of 12 mg/kg and higher and a drug-related increase in mammary carcinomas and adenoacanthomas and pituitary pars distalis adenomas in female mice. The applicant also provided data from various studies showing that lurasidone significantly increases prolactin in several different species including rats and mice. Conclusions: I agree with the division pharm/tox conclusion that this application can be approved from a pharm/tox perspective. The division recommends that lurasidone be labeled with pregnancy category B.