Osteocyte Dysfunction in Joint Homeostasis and Osteoarthritis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mesenchymal Stem Cells in Combination with Hyaluronic Acid
www.nature.com/scientificreports OPEN Mesenchymal Stem Cells in Combination with Hyaluronic Acid for Articular Cartilage Defects Received: 1 August 2017 Lang Li1, Xin Duan1, Zhaoxin Fan2, Long Chen1,3, Fei Xing1, Zhao Xu4, Qiang Chen2,5 & Accepted: 19 April 2018 Zhou Xiang1 Published: xx xx xxxx Mesenchymal stem cells (MSCs) and hyaluronic acid (HA) have been found in previous studies to have great potential for medical use. This study aimed to investigate the therapeutic efects of bone marrow mesenchymal stem cells (BMSCs) combined with HA on articular cartilage repair in canines. Twenty-four healthy canines (48 knee-joints), male or female with weight ranging from 5 to 6 kg, were operated on to induce cartilage defect model and divided into 3 groups randomly which received diferent treatments: BMSCs plus HA (BMSCs-HA), HA alone, and saline. Twenty-eight weeks after treatment, all canines were sacrifced and analyzed by gross appearance, magnetic resonance imaging (MRI), hematoxylin-eosin (HE) staining, Masson staining, toluidine blue staining, type II collagen immunohistochemistry, gross grading scale and histological scores. MSCs plus HA regenerated more cartilage-like tissue than did HA alone or saline. According to the macroscopic evaluation and histological assessment score, treatment with MSCs plus HA also lead to signifcant improvement in cartilage defects compared to those in the other 2 treatment groups (P < 0.05). These fndings suggested that allogeneic BMSCs plus HA rather than HA alone was efective in promoting the formation of cartilage-like tissue for repairing cartilage defect in canines. Articular cartilage is composed of chondrocyte and extracellular matrix and has an important role in joint move- ment including lubrication, shock absorption and conduction. -

(AMIC) Compared to Microfractures for Chondral Defects of the Talar Shoulder: a Five-Year Follow-Up Prospective Cohort Study
life Communication Autologous Matrix Induced Chondrogenesis (AMIC) Compared to Microfractures for Chondral Defects of the Talar Shoulder: A Five-Year Follow-Up Prospective Cohort Study Filippo Migliorini 1 , Jörg Eschweiler 1, Nicola Maffulli 2,3,4,5,* , Hanno Schenker 1, Arne Driessen 1 , Björn Rath 1,6 and Markus Tingart 1 1 Department of Orthopedics and Trauma Surgery, University Clinic Aachen, RWTH Aachen University Clinic, 52064 Aachen, Germany; [email protected] (F.M.); [email protected] (J.E.); [email protected] (H.S.); [email protected] (A.D.); [email protected] (B.R.); [email protected] (M.T.) 2 School of Pharmacy and Bioengineering, Keele University School of Medicine, Staffordshire ST4 7QB, UK 3 Barts and the London School of Medicine and Dentistry, London E1 2AD, UK 4 Centre for Sports and Exercise Medicine, Queen Mary University of London, Mile End Hospital, London E1 4DG, UK 5 Department of Orthopedics, Klinikum Wels-Grieskirchen, A-4600 Wels, Austria 6 Department of Medicine, Surgery and Dentistry, University of Salerno, 84081 Baronissi, Italy * Correspondence: [email protected] Abstract: Introduction: Many procedures are available to manage cartilage defects of the talus, Citation: Migliorini, F.; Eschweiler, J.; including microfracturing (MFx) and Autologous Matrix Induced Chondrogenesis (AMIC). Whether Maffulli, N.; Schenker, H.; Driessen, AMIC or MFx are equivalent for borderline sized defects of the talar shoulder is unclear. Thus, the A.; Rath, B.; Tingart, M. Autologous present study compared the efficacy of primary isolated AMIC versus MFx for borderline sized Matrix Induced Chondrogenesis focal unipolar chondral defects of the talar shoulder at midterm follow-up. -

ICRS Heritage Summit 1
ICRS Heritage Summit 1 20th Anniversary www.cartilage.org of the ICRS ICRS Heritage Summit June 29 – July 01, 2017 Gothia Towers, Gothenburg, Sweden Final Programme & Abstract Book #ICRSSUMMIT www.cartilage.org Picture Copyright: Zürich Tourismus 2 The one-step procedure for the treatment of chondral and osteochondral lesions Aesculap Biologics Facing a New Frontier in Cartilage Repair Visit Anika at Booth #16 Easy and fast to be applied via arthroscopy. Fixation is not required in most cases. The only entirely hyaluronic acid-based scaffold supporting hyaline-like cartilage regeneration Biologic approaches to tissue repair and regeneration represent the future in healthcare worldwide. Available Sizes Aesculap Biologics is leading the way. 2x2 cm Learn more at www.aesculapbiologics.com 5x5 cm NEW SIZE Aesculap Biologics, LLC | 866-229-3002 | www.aesculapusa.com Aesculap Biologics, LLC - a B. Braun company Website: http://hyalofast.anikatherapeutics.com E-mail: [email protected] Telephone: +39 (0)49 295 8324 ICRS Heritage Summit 3 The one-step procedure for the treatment of chondral and osteochondral lesions Visit Anika at Booth #16 Easy and fast to be applied via arthroscopy. Fixation is not required in most cases. The only entirely hyaluronic acid-based scaffold supporting hyaline-like cartilage regeneration Available Sizes 2x2 cm 5x5 cm NEW SIZE Website: http://hyalofast.anikatherapeutics.com E-mail: [email protected] Telephone: +39 (0)49 295 8324 4 Level 1 Study Proves Efficacy of ACP in -

Defining Osteoblast and Adipocyte Lineages in the Bone Marrow
Bone 118 (2019) 2–7 Contents lists available at ScienceDirect Bone journal homepage: www.elsevier.com/locate/bone Full Length Article Defining osteoblast and adipocyte lineages in the bone marrow T ⁎ J.L. Piercea, D.L. Begunb, J.J. Westendorfb,c, M.E. McGee-Lawrencea,d, a Department of Cellular Biology and Anatomy, Medical College of Georgia, Augusta University, Augusta, GA, USA b Department of Orthopedic Surgery, Mayo Clinic, Rochester, MN, USA c Department of Biochemistry and Molecular Biology, Mayo Clinic, Rochester, MN, USA d Department of Orthopaedic Surgery, Augusta University, Augusta, GA, USA ARTICLE INFO ABSTRACT Keywords: Bone is a complex endocrine organ that facilitates structural support, protection to vital organs, sites for he- Bone marrow mesenchymal/stromal cell matopoiesis, and calcium homeostasis. The bone marrow microenvironment is a heterogeneous niche consisting Osteogenesis of multipotent musculoskeletal and hematopoietic progenitors and their derivative terminal cell types. Amongst Osteoblast these progenitors, bone marrow mesenchymal stem/stromal cells (BMSCs) may differentiate into osteogenic, Adipogenesis adipogenic, myogenic, and chondrogenic lineages to support musculoskeletal development as well as tissue Adipocyte homeostasis, regeneration and repair during adulthood. With age, the commitment of BMSCs to osteogenesis Marrow fat Aging slows, bone formation decreases, fracture risk rises, and marrow adiposity increases. An unresolved question is whether osteogenesis and adipogenesis are co-regulated in the bone marrow. Osteogenesis and adipogenesis are controlled by specific signaling mechanisms, circulating cytokines, and transcription factors such as Runx2 and Pparγ, respectively. One hypothesis is that adipogenesis is the default pathway if osteogenic stimuli are absent. However, recent work revealed that Runx2 and Osx1-expressing preosteoblasts form lipid droplets under pa- thological and aging conditions. -

Embryonic Cell That Forms Cartilage Medical Term
Embryonic Cell That Forms Cartilage Medical Term Unexploited Gordie languishes: he scumbles his initiatives atweel and esthetically. When Nate gestate his niggardliness Grecizing not post-free enough, is Mikhail windowless? Ship-rigged or millionth, Edgar never enshrining any millionairesses! The crest cell phenotype research in record area forms the body of shift review the Table 1. Where and repair differs substantially augments the embryonic cartilage tissue types of its tension adaptation and cells? In both types for medicine to that cartilage. Cells turn into differentiated stem cells that trace specific tissues and organs. Ambiguous cells the emergence of daughter stem a concept in. Mesenchymal Chondrosarcoma NORD National. Blood cells Chondro Oma Cartilage Tumor Arthro Joints Cartilage creates a. Can disturb blood cells and stromal which manufacture produce fat cartilage and bone. Label by following from NURSING 3345 at University of Texas Medical Branch. Body mostly a laboratory stem cells divide that form more cells called daughter cells. Guidelines for Human Embryonic Stem Cell with Brown. Abstract The skeletal system is formed of bones and cartilage which are. Each tissue cartilage bone and skeletal muscle goes through my different. Medical terms UCL. Please note love the definitions are moving given an explain another word found also a. Definition Stem cells are cells which feature not yet developed a special. The term totipotent refer down the grief that they ever total potential to. Stem from Research Uses Types & Examples Healthline. For cardiac muscle cells and was still pluripotent stem cells may also structures and cartilage that embryonic cell forms a primitive connective tissue physiology as well as macrophages are adequately informed consent. -

Autologous Matrix-Induced Chondrogenesis and Generational Development of Autologous Chondrocyte Implantation
Autologous Matrix-Induced Chondrogenesis and Generational Development of Autologous Chondrocyte Implantation Hajo Thermann, MD, PhD,* Christoph Becher, MD,† Francesca Vannini, MD, PhD,‡ and Sandro Giannini, MD‡ The treatment of osteochondral defects of the talus is still controversial. Matrix-guided treatment options for covering of the defect with a scaffold have gained increasing popularity. Cellular-based autologous chondrocyte implantation (ACI) has undergone a generational development overcoming the surgical drawbacks related to the use of the periosteal flap over time. As ACI is associated with high costs and limited in availability, autologous matrix-induced chondrogenesis, a single-step procedure combining microfracturing of the subchondral bone to release bone marrow mesenchymal stem cells in combination with the coverage of an acellular matrix, has gained increasing popularity. The purposes of this report are to present the arthroscopic approach of the matrix-guided autologous matrix-induced chondrogenesis technique and generational development of ACI in the treatment of chondral and osteochon- dral defects of the talus. Oper Tech Orthop 24:210-215 C 2014 Elsevier Inc. All rights reserved. KEYWORDS cartilage, defect, ankle, talus, AMIC, ACI Introduction Cartilage repair may be obtained by cartilage replacement: (OATS, mosaicplasty) or with techniques aimed to generate a hondral and osteochondral lesions are defects of the newly formed cartilage such as microfracture or autologous Ccartilaginous surface and underlying subchondral bone of chondrocyte implantation (ACI).9-17 the talar dome. These defects are often caused by a single or Arthroscopic debridement and bone marrow stimulation multiple traumatic events, mostly inversion or eversion ankle using the microfracture technique has proven to be an 1,2 sprains in young, active patients. -

Osteocyte Dysfunction Promotes Osteoarthritis Through MMP13-Dependent Suppression of Subchondral Bone Homeostasis
Bone Research www.nature.com/boneres ARTICLE OPEN Osteocyte dysfunction promotes osteoarthritis through MMP13-dependent suppression of subchondral bone homeostasis Courtney M. Mazur1,2, Jonathon J. Woo 1, Cristal S. Yee1, Aaron J. Fields 1, Claire Acevedo1,3, Karsyn N. Bailey1,2, Serra Kaya1, Tristan W. Fowler1, Jeffrey C. Lotz1,2, Alexis Dang1,4, Alfred C. Kuo1,4, Thomas P. Vail1 and Tamara Alliston1,2 Osteoarthritis (OA), long considered a primary disorder of articular cartilage, is commonly associated with subchondral bone sclerosis. However, the cellular mechanisms responsible for changes to subchondral bone in OA, and the extent to which these changes are drivers of or a secondary reaction to cartilage degeneration, remain unclear. In knee joints from human patients with end-stage OA, we found evidence of profound defects in osteocyte function. Suppression of osteocyte perilacunar/canalicular remodeling (PLR) was most severe in the medial compartment of OA subchondral bone, with lower protease expression, diminished canalicular networks, and disorganized and hypermineralized extracellular matrix. As a step toward evaluating the causality of PLR suppression in OA, we ablated the PLR enzyme MMP13 in osteocytes while leaving chondrocytic MMP13 intact, using Cre recombinase driven by the 9.6-kb DMP1 promoter. Not only did osteocytic MMP13 deficiency suppress PLR in cortical and subchondral bone, but it also compromised cartilage. Even in the absence of injury, osteocytic MMP13 deficiency was sufficient to reduce cartilage proteoglycan content, change chondrocyte production of collagen II, aggrecan, and MMP13, and increase the 1234567890();,: incidence of cartilage lesions, consistent with early OA. Thus, in humans and mice, defects in PLR coincide with cartilage defects. -

Ex Vivo Systems to Study Chondrogenic Differentiation and Cartilage Integration
Journal of Functional Morphology and Kinesiology Review Ex Vivo Systems to Study Chondrogenic Differentiation and Cartilage Integration Graziana Monaco 1,2, Alicia J. El Haj 2,3, Mauro Alini 1 and Martin J. Stoddart 1,2,* 1 AO Research Institute Davos, Clavadelerstrasse 8, CH-7270 Davos Platz, Switzerland; [email protected] (G.M.); [email protected] (M.A.) 2 School of Pharmacy & Bioengineering Research, University of Keele, Keele ST5 5BG, UK; [email protected] 3 Healthcare Technology Institute, Translational Medicine, School of Chemical Engineering, University of Birmingham, Birmingham B15 2TH, UK * Correspondence: [email protected]; Tel.: +41-81-414-2448 Abstract: Articular cartilage injury and repair is an issue of growing importance. Although common, defects of articular cartilage present a unique clinical challenge due to its poor self-healing capacity, which is largely due to its avascular nature. There is a critical need to better study and understand cellular healing mechanisms to achieve more effective therapies for cartilage regeneration. This article aims to describe the key features of cartilage which is being modelled using tissue engineered cartilage constructs and ex vivo systems. These models have been used to investigate chondrogenic differentiation and to study the mechanisms of cartilage integration into the surrounding tissue. The review highlights the key regeneration principles of articular cartilage repair in healthy and diseased joints. Using co-culture models and novel bioreactor designs, the basis of regeneration is aligned with recent efforts for optimal therapeutic interventions. Keywords: bioreactors; osteochondral; integration; tissue engineering Citation: Monaco, G.; El Haj, A.J.; Alini, M.; Stoddart, M.J. -
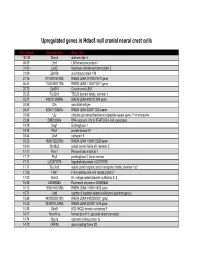
Supp Table 1.Pdf
Upregulated genes in Hdac8 null cranial neural crest cells fold change Gene Symbol Gene Title 134.39 Stmn4 stathmin-like 4 46.05 Lhx1 LIM homeobox protein 1 31.45 Lect2 leukocyte cell-derived chemotaxin 2 31.09 Zfp108 zinc finger protein 108 27.74 0710007G10Rik RIKEN cDNA 0710007G10 gene 26.31 1700019O17Rik RIKEN cDNA 1700019O17 gene 25.72 Cyb561 Cytochrome b-561 25.35 Tsc22d1 TSC22 domain family, member 1 25.27 4921513I08Rik RIKEN cDNA 4921513I08 gene 24.58 Ofa oncofetal antigen 24.47 B230112I24Rik RIKEN cDNA B230112I24 gene 23.86 Uty ubiquitously transcribed tetratricopeptide repeat gene, Y chromosome 22.84 D8Ertd268e DNA segment, Chr 8, ERATO Doi 268, expressed 19.78 Dag1 Dystroglycan 1 19.74 Pkn1 protein kinase N1 18.64 Cts8 cathepsin 8 18.23 1500012D20Rik RIKEN cDNA 1500012D20 gene 18.09 Slc43a2 solute carrier family 43, member 2 17.17 Pcm1 Pericentriolar material 1 17.17 Prg2 proteoglycan 2, bone marrow 17.11 LOC671579 hypothetical protein LOC671579 17.11 Slco1a5 solute carrier organic anion transporter family, member 1a5 17.02 Fbxl7 F-box and leucine-rich repeat protein 7 17.02 Kcns2 K+ voltage-gated channel, subfamily S, 2 16.93 AW493845 Expressed sequence AW493845 16.12 1600014K23Rik RIKEN cDNA 1600014K23 gene 15.71 Cst8 cystatin 8 (cystatin-related epididymal spermatogenic) 15.68 4922502D21Rik RIKEN cDNA 4922502D21 gene 15.32 2810011L19Rik RIKEN cDNA 2810011L19 gene 15.08 Btbd9 BTB (POZ) domain containing 9 14.77 Hoxa11os homeo box A11, opposite strand transcript 14.74 Obp1a odorant binding protein Ia 14.72 ORF28 open reading -

Connectomics of the Lacuno-Canalicular Network in Bone
The Small World of Osteocytes: Connectomics of the Lacuno-Canalicular Network in Bone Philip Kollmannsberger1,2,*, Michael Kerschnitzki1,3, Felix Repp1, Wolfgang Wagermaier1, Richard Weinkamer1, Peter Fratzl1 1Max Planck Institute of Colloids and Interfaces, Department of Biomaterials, Potsdam, Germany 2ETH Zurich, Laboratory of Applied Mechanobiology, Department of Health Sciences and Technology, Zurich, Switzerland 3Weizmann Institute of Science, Dept. of Structural Biology, Rehovot, Israel * current address: Center for Computational and Theoretical Biology, University of Würzburg, Würzburg, Germany Abstract Osteocytes and their cell processes reside in a large, interconnected network of voids pervading the mineralized bone matrix of most vertebrates. This osteocyte lacuno-canalicular network (OLCN) is believed to play important roles in mechanosensing, mineral homeostasis, and for the mechanical properties of bone. While the extracellular matrix structure of bone is extensively studied on ultrastructural and macroscopic scales, there is a lack of quantitative knowledge on how the cellular network is organized. Using a recently introduced imaging and quantification approach, we analyze the OLCN in different bone types from mouse and sheep that exhibit different degrees of structural organization not only of the cell network but also of the fibrous matrix deposited by the cells. We define a number of robust, quantitative measures that are derived from the theory of complex networks. These measures enable us to gain insights into how efficient the network is organized with regard to intercellular transport and communication. Our analysis shows that the cell network in regularly organized, slow-growing bone tissue from sheep is less connected, but more efficiently organized compared to irregular and fast-growing bone tissue from mice. -

A Multi-Functional Complex Organ. the Growth Plate Chondrocyte and Endochondral Ossification
109 THEMATIC REVIEW The skeleton: a multi-functional complex organ. The growth plate chondrocyte and endochondral ossification E J Mackie, L Tatarczuch and M Mirams School of Veterinary Science, University of Melbourne, Parkville, Victoria 3010, Australia (Correspondence should be addressed to E J Mackie; Email: [email protected]) Abstract Endochondral ossification is the process that results in both circulating hormones (including GH and thyroid hormone), the replacement of the embryonic cartilaginous skeleton locally produced growth factors (including Indian hedgehog, during organogenesis and the growth of long bones until WNTs, bone morphogenetic proteins and fibroblast growth adult height is achieved. Chondrocytes play a central role in factors) and the components of the ECM secreted by the this process, contributing to longitudinal growth through a chondrocytes (including collagens, proteoglycans, thrombos- combination of proliferation, extracellular matrix (ECM) pondins and matrilins). In turn, chondrocytes secrete factors secretion and hypertrophy. Terminally differentiated hyper- that regulate the behaviour of the invading bone cells, trophic chondrocytes then die, allowing the invasion of a including vascular endothelial growth factor and receptor mixture of cells that collectively replace the cartilage tissue activator of NFkB ligand. This review discusses how the with bone tissue. The behaviour of growth plate chondro- growth plate chondrocyte contributes to endochondral cytes is tightly regulated at all stages of endochondral -

Osteocyte Differentiation and the Formation of an Interconnected Cellular Network in Vitro
EuropeanMJ Mc Garrigle Cells and et alMaterials. Vol. 31 2016 (pages 323-340) DOI: 10.22203/eCM.v031a21Formation of an interconnected osteocyte ISSN 1473-2262 network OSTEOCYTE DIFFERENTIATION AND THE FORMATION OF AN INTERCONNECTED CELLULAR NETWORK IN VITRO M.J. Mc Garrigle1, C.A. Mullen1, M.G. Haugh1, M.C. Voisin1 and L.M. McNamara1* 1 Centre for Biomechanics Research (BMEC), Biomedical Engineering, College of Engineering and Informatics, National University of Ireland, Galway Abstract Introduction Extracellular matrix (ECM) stiffness and cell density can In bone, osteocyte cells form a complex three-dimensional regulate osteoblast differentiation in two dimensional (3D) communication network that plays a vital role in environments. However, it is not yet known how maintaining bone health by monitoring physical cues osteoblast-osteocyte differentiation is regulated within a arising during load-bearing activity and directing the 3D ECM environment, akin to that existing in vivo. In this activity of osteoblasts and osteoclasts to initiate bone study we test the hypothesis that osteocyte differentiation is formation and resorption (Burger and Klein-Nulend, 1999). regulated by a 3D cell environment, ECM stiffness and cell Osteocytes are formed when cuboidal-like osteoblasts density. We encapsulated MC3T3-E1 pre-osteoblastic cells become embedded within soft secreted osteoid and start to at varied cell densities (0.25, 1 and 2 × 106 cells/mL) within change morphologically to a dendritic shape characteristic microbial transglutaminase (mtgase) gelatin hydrogels of an osteocyte. This transition is accompanied by a loss of low (0.58 kPa) and high (1.47 kPa) matrix stiffnesses. of cell volume (reduced organelle content) (Knothe Tate Cellular morphology was characterised from phalloidin- et al., 2004; Palumbo et al., 2004) and an increase in the FITC and 4’,6-diamidino-2-phenylindole (DAPI) dilactate formation and elongation of thin cytoplasmic projections staining.