Table of Contents Acknowledgements
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

State Zone Commissionerate Name Division Name Range Name
Commissionerate State Zone Division Name Range Name Range Jurisdiction Name Gujarat Ahmedabad Ahmedabad South Rakhial Range I On the northern side the jurisdiction extends upto and inclusive of Ajaji-ni-Canal, Khodani Muvadi, Ringlu-ni-Muvadi and Badodara Village of Daskroi Taluka. It extends Undrel, Bhavda, Bakrol-Bujrang, Susserny, Ketrod, Vastral, Vadod of Daskroi Taluka and including the area to the south of Ahmedabad-Zalod Highway. On southern side it extends upto Gomtipur Jhulta Minars, Rasta Amraiwadi road from its intersection with Narol-Naroda Highway towards east. On the western side it extend upto Gomtipur road, Sukhramnagar road except Gomtipur area including textile mills viz. Ahmedabad New Cotton Mills, Mihir Textiles, Ashima Denims & Bharat Suryodaya(closed). Gujarat Ahmedabad Ahmedabad South Rakhial Range II On the northern side of this range extends upto the road from Udyognagar Post Office to Viratnagar (excluding Viratnagar) Narol-Naroda Highway (Soni ni Chawl) upto Mehta Petrol Pump at Rakhial Odhav Road. From Malaksaban Stadium and railway crossing Lal Bahadur Shashtri Marg upto Mehta Petrol Pump on Rakhial-Odhav. On the eastern side it extends from Mehta Petrol Pump to opposite of Sukhramnagar at Khandubhai Desai Marg. On Southern side it excludes upto Narol-Naroda Highway from its crossing by Odhav Road to Rajdeep Society. On the southern side it extends upto kulcha road from Rajdeep Society to Nagarvel Hanuman upto Gomtipur Road(excluding Gomtipur Village) from opposite side of Khandubhai Marg. Jurisdiction of this range including seven Mills viz. Anil Synthetics, New Rajpur Mills, Monogram Mills, Vivekananda Mill, Soma Textile Mills, Ajit Mills and Marsdan Spinning Mills. -
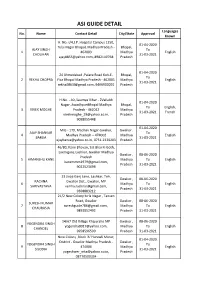
ASI Registered Tourist Guide List, MP
ASI GUIDE DETAIL Languages No. Name Contact Detail City/State Approval Known H. No.-I/4,J.P. Hospital Campus 1250, 01-04-2020 Tulsi Nagar Bhopal, Madhya Pradesh - Bhopal, AJAY SINGH To 1 462003 Madhya English CHOUHAN 31-03-2021 [email protected], 8982140768 Pradesh 01-04-2020 24 Ahmedabad ,Palace Road Koh-E- Bhopal, To 2 REKHA CHOPRA Fiza Bhopal Madhya Pradesh - 462001 Madhya English 31-03-2021 [email protected], 9406900091 Pradesh H.No. - 40 ,Saumya Vihar - 2Vallabh 01-04-2020 Nagar, AwadhpuriBhopal Madhya Bhopal, To English, 3 VIVEK MOGHE Pradesh - 462022 Madhya 31-03-2021 French [email protected], Pradesh 9098055448 01-04-2020 MIG - 179, Madhav Nagar Gwalior, Gwalior , AJAY SHANKAR To 4 Madhya Pradesh – 474002 Madhya English BARUA 31-03-2021 [email protected], 0751-2320203 Pradesh 46/80, Kane Bhavan, Sat Bhai Ki Goth, Laxmiganj, Lashkar, Gwalior Madhya Gwalior , 08-06-2020 Pradesh 5 HIMANSHU KANE Madhya To English [email protected], Pradesh 31-03-2021 9022523698 23 Jivaji Ganj Lane, Lashkar, Teh, Gwalior , 08-06-2020 RACHNA Gwalior Dist., Gwalior, MP 6 Madhya To English SHRIVASTAVA [email protected], Pradesh 31-03-2021 9368883212 21/2 New Colony birla Nagar , Tansen Road, Gwalior Gwalior , 08-06-2020 SURESH KUMAR 7 [email protected] , Madhya To English CHAURASIA 9893052492 Pradesh 31-03-2021 14/67 Old Village Khajuraho MP Gwalior , 08-06-2020 YOGENDRA SINGH 8 [email protected], Madhya To English CHANDEL 9958596599 Pradesh 31-03-2021 New Colony ,Block 'A' Hurawli Morar, 01-04-2020 District - Gwalior Madhya Pradesh - Gwalior , YOGENDRA SINGH To 9 474006 Madhya English SISODIA 31-03-2021 [email protected], Pradesh 08770500334 ASI GUIDE DETAIL Languages No. -

LIST of MINING PROJECTS - MPSEAC PENDING S.No
LIST OF MINING PROJECTS - MPSEAC PENDING S.No. Case No Category Name of Project Proponent Activity 1 59/2008 1(a) Agrawal Mineral process, Manganese ore mine 5.00 ha. Gwari-wadhana, 1(a) NagpurRoad , Chhindwara M.P. Teh-Sausar, Distt-Chhindwara M.P. 2 70/20081 1(a) M/s Ismail & Sons MissionChowk, Lime stone mine 10-748 ha. Village Bhatgaon (a) Katni M.P. Sunehra Teh-Murwada Katni M.P. 3 99/2008 1(a) M/s Nirmala Minerals Dubiyara Iron Ore Mine 32.375 ha. at 1(a) PathalewardKatni M.P. DubiyaraTalluka-Sihora Jabalpur M.P. 4 104/2008 1(a) Anand mining corporation Dubiyara-Tikaria Iron ore mine 26.00 ha at Village 1(a) Pathakward, Katni- M.P. Dubiyara Tikaria Jabalpur 5 411/2009 1(a) Shri Kishore Kumar Station Road , Limestone & Dolomite mine 5.605 ha. 6200 TPA 1(a) Katni-M.P. at Village- Chandan Teh- Murwara, Distt-Katni- M.P. 6 412/2009 1(a) M/s Kamal lime Industries Station Lime stone & Dolomite mine 7.205 11500 TPA at 1(a) Road Katni-M.P. Village ChandanTeh-Murwara Katni-M.P. 7 434/2009 1(a) Smt. Rekha Sharma 192, Second Laterite, clay and Red ochre deposit mine 6.83 ha. 1(a) Floor, Rachna Nagar Bhopal-M.P. at village Salebhar Teh- Bahoriband, Distt-Katni- M.P. 8 472/2009 1(a) N.M. Dubash Stone & Lime Co. Pvt Lime stone & Dolomite mine 7.42 ha. production 1(a) Ltd Station Raod, Maihar Satna capacity 1.6 lakhs TPA at village Kachhgawan, –M.P. -

Nagar Palika Parishad, Hatta District - Damoh (M.P.)
79°33'45"E 79°34'30"E 79°35'15"E 79°36'0"E 79°36'45"E 79°37'30"E Nagar Palika Parishad, Hatta District - Damoh (M.P.) Map Title Basemap of Municipal Council Area Without Ward Boundary TDM01215 N X " 0 ' 9 ° 4 Legend 2 a) n an (P # N j " n 0 a ' g Important Landmarks 9 n ° a 4 2 m A To National Highway SDM0081 X ! ! ! ! ! State Highway ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Major Road ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Other Road ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Bridge / Culvert ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Municipal Boundary ! ! 9 ! 4 ! ! - ! ! ! H j ! ! ! S j ! ! ! ! ! ! ! ! ! ! ! ! Drainage / Nala ! ! ! ! ! ! ! ! # ! ! 9 -4 ! ! H S Ganga Jhiriya ! ! ! ! Pond / Tank / Reservoir ! OHT ! ! # Nagar ! ! Palika Mukti ! ! # ! # Govt. ! ! Dham Hospital ! ! Gauri Sankar Mandir # Mangal ! ! Road ! ! Bhavan ! # ! ! # ! ! Sheetla ! ! Dadda Mata ! ! Mandir Kala Manch # ! ! River # Swami Vivekanand Maha Vidyalya ! ! ! Tal ! N " ! Uddeshwari Mandir (Timber Mart) ! 5 ! Gopal Ji ! ! # ! ! ! ! ! # ! 1 ! ! ! ! ! ! ' ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Talaiya ! ! ! 8 ! Dam ! ° ! ! ! 4 Maanpur Jod Road ! ! Sarswati 2 # ! ! shisu # ! ! Jain Mandir # Mandir ! # ! ! ! ! ! Laxmi Narayan Mandir ! Surai ! ! ! ! ! ! ! ! ! ! ! ! ! Ghat ! ! ! ! # ! ! ! ! ! ! N ! ! ! " ! ! 5 ! ! 1 # ! ! ' Chandi Mata Mandir ! ! # 8 Ratan Bajariya ° ! ! ! ! ! ! ! ! 4 -

Madhya Pradesh)
SOCIAL SAFEGUARD COMPLIANCE REPORT June 2013 IND: RURAL CONNECTIVITY INVESTMENT PROGRAM Batch 2 Roads (Madhya Pradesh) Prepared by the Ministry of Rural Development, Government of India for the Asian Development Bank ABBREVIATIONS ADB : Asian Development Bank APs : Affected Persons BPL : Below Poverty Line FFA : Framework Financing Agreement GOI : Government of India GRC : Grievances Redressal Committee IA : Implementing Agency MFF : Multitranche Financing Facility MORD : Ministry of Rural Development MOU : Memorandum of Understanding NC : Not Connected NGO : Non-Government Organization NRRDA : National Rural Road Development Agency MGNREGA : Mahatma Gandhi National Rural Employment Guarantee Act MPRRDA : Madhya Pradesh Rural Road Development Agency PIU : Project Implementation Unit PIC : Project Implementation Consultants PFR : Periodic Finance Request PMGSY : Pradhan Mantri Gram Sadak Yojana RCIP : Rural Connectivity Investment Program ST : Scheduled Tribes TA : Technical Assistance TOR : Terms of Reference TSC : Technical Support Consultants VAP : Vulnerable Affected Person WHH : Women Headed Households GLOSSARY Affected Persons (APs): Affected persons are people (households) who may lose their land or source of livelihood due top the project. It may be all or part of their physical and non-physical assets, irrespective of legal or ownership titles. Encroacher: A person, who has trespassed government land, adjacent to his/her own land or asset, to which he/she is not entitled, by deriving his/her livelihood there. Such act is called “Encroachment.” Gramsabha Resolution: A resolution drawn up by unanimous and collective decision of villagers. The resolution drawn up for the purpose of the project refers to identification of the affected persons, extent of their losses by unique identification and signed consent of the affected persons to donate voluntarily the identified assets for the project purpose. -

Permission for Laying of 200 Dia DI K7 Water Supply Pipeline by MP
UTA Wests TTA Ue LUT (asa Uftaet sik asrnt dares, Het TAT ) NATIONAL HIGHWAYS AUTHORITY OF INDIA (Ministry of Road Transport and Highways, Govt. of India) gata rater / REGIONAL OFFICE am $-2/167, ate aicirh, sateria tea Ver H ure, wlave (w. ) 462016 BHARATMALA E-2/167, Arera Colony, Near Habibganj Railway Station, Bhopal (M.P.) 462016 ROAD TO PROSPERITY GeHTa/Phone : 0755-2426638, the /Fax : 0755-2426698, $-Oe1/E-mail : [email protected] NHAI/RO-MP/CHHP/Jal Nigam/Pipe line/2021/ Uf & | 2- Date: 21.01.2021 Invitation of Public Comments Sub: Permission for laying of 200 dia DI K7 water supply pipeline by MP Jalnigam Maryadit PIU Tikamgarh under Niwari-Prathvipur multi Village Rural water supply scheme District Tikamgarh from km 39+100 (Near Thone/Urdora village) to km 40+250 (Near Thone/Urdora) 1.2km and km 8+150 (Near Orchha Tigela) to km 10.000 (near Orchha Tigela) 1.9 km in length along National Highway 76/75. Ref: — 1.This office letter no. 41791 dated 20.01.2021. 2.PD, PiU-Chhatarpur letter no, CHHP/26010/4/Jal Nigam/Pipe Line/2019/5628 dated 08.01.2021. This is in supersession to this office letter no. 41791 dated 20.01.2021, The Project Director, PIU- Chhatarpur NHAI vide their letter dated 08.01.2021 has submitted the proposal for Permission for laying of 200 dia DI K7 water supply pipeline by MP Jalnigam Maryadit PIU Tikamgarh under Niwari-Prathvipur multi Village Rural water supply scheme District Tikamgarh from km 39+100 (Near Thone/Urdora village) to km 40+250 (Near Thone/Urdora) 1.2km and km 8+150 (Near Orchha Tigela) to km 10.000 (near Orchha Tigela) 1.9 km in length along National Highway 76/75. -
District Census Handbook, Chhatarpur, Parts X (A) & X
• CENSUS OF INDIA 1971 SERIES 10 MADHYA PRADESH DISTRICT CENSUS HANDBOOK PARTS X(A) & X(B) VILLAGE AND TOWN DIRECTORY VILLAGE AND TOWN-WISE PRIMARY CENSUS ABSTRACT CHHATARPUR DISTRICT A. K. PANDYA OF THE INDIAN ADMI]'.;)STRATIVE SERVICE DIRECTOR OF CENSUS OPERATIONS. MADHYA PRADESH PUBLISHED BY THE GOVERNMENT OF MADHYA PRADESH 1976 CONTENTS Pagt' 1. Preface i-ii 2. List of Abbreviations 1 3. Alphabetical List of Villages 3-15 ( j ) Laundi Tahsil 3-6 ( ii) Chhatarpur Tah,il 6-10 ( iii) Bijawar Tah~il 10··15 PART A 1. Explanatory Note 19-31 2. Village Directory (Amenities and Land-use) 32-83 ( i) Laundi Tahsil 32-45 ( ii) Chhatarpur Tahsil 46-63 ( iii) Bijawar Tahsil 64-83 3. Appendix to Village Directory 84-85 4. Town Directory 86-92 ( i) Status, Growth History and Functional Category of Towns 86 ( ii) Physical Aspects and Location of Towns 87 ( iii) Civic Finance 88 ( iv) Civic and other Amenities 89 ( v) Medical, Educational, Recreational and Cultural Facilities in Towns 90 ( vi) Trade, Commerce, Industry and B,l11king 91 (vii) Population by Religion and Scheduled Castes! Scheduled Tribes in Towns 92 5. Appendix to Town Directory 93 PART B 1. Explanatory Note 97·98 Z. Figures at a Glance 99 3. Primary Census Abstract 100-195 District Abstract 100-103 Laundi Tahsil 104·125 (Rural) 104-125 (Urban) Chhatarpur Tah~il 126-163 (Rural) 126-155 (Urban) 154-163 Bijawar Tahsil 164-195 (Rural) 164-193 (Urban) 194-195 1971 CENSUS PUBLICATIONS, MADHYA PRADESH (All the Census Publications of this Stat(· \\ill hear series No. -

Mineral Resource Department District Chhatarpur
DISTRICT SURVEY REPORT CHHATARPUR MADHYA PRADESH MINERAL RESOURCE DEPARTMENT DISTRICT CHHATARPUR IN COMPLIANCE OF MINISTRY OF ENVIRONMENT, FOREST AND CLIMATE CHANGE, NOTIFICATION DATED15.01.2016 CONTENTS Pages 1. Introduction 3-4 2. Overview of Mining Activity in the District 5-7 3. The List of Mining Leases in the District with location, 8-11 area and period of validity 4. General Profile of the District 12-15 5. Land Utilization Pattern in the district: Forest, Agriculture, 16 Horticulture, Mining 6. Physiographic of the District 17 7. Geology and Mineral Wealth 18-29 8. Conclusion 20 09. References 21 1. INTRODUCTION Chhatarpur was founded in 1785 and is named after the Bundela Rajput leader Chhatrasal, the founder of Bundelkhand independence, and contains his cenotaph. The state was ruled by his descendants until 1785. At that time the Ponwar clan of the Rajputs took control of Chhatarpur. The state was guaranteed to Kunwar Sone Singh Ponwar in 1806 by the British Raj. In 1854 Chhatarpur would have lapsed to the British government for want of direct heirs under the doctrine of lapse, but was conferred on Jagat Raj as a special act of grace. The Ponwar Rajas ruled a princely state with an area of 1,118 square miles (2,900 km2), and population of 156,139 in 1901, which was part of the Bundelkhand agency of Central India. In 1901 the town of Chhatarpur had a population of 10,029, a high school and manufactured paper and coarse cutlery. The state also contained the British cantonment of Nowgong. After the independence of India in 1947, the Rajas of Chhatarpur acceded to India, and Chhatarpur, together with the rest of Bundelkhand, became part of the Indian state of Vindhya Pradesh. -

Brief Industrial Profile of Tikamgarh District Madhya Pradesh Carried
lR;eso t;rs Government of India Ministry of MSME Brief Industrial Profile of Tikamgarh District Madhya Pradesh Carried out by MSME - Development Institute (Ministry of MSME, Govt. of India,) 10, Polo ground Industrial Estate, Indore-452015(MP) Phone: 0731-2490149, 2421730 Fax: 0731-2421037 E-mail: [email protected] Web- www.msmeindore.nic.in 1 Contents S. No. Topic Page No. 1. General Characteristics of the District 03 1.1 Location & Geographical Area 03 1.2 Topography 03 1.3 Availability of Minerals. 03 1.4 Forest 03 1.5 Administrative set up 04 2. District at a glance 05-06 2.1 Existing Status of Industrial Area in the District Tikamgarh 07 3. Industrial Scenario Of Tikamgarh 07 3.1 Industry at a Glance 08 3.2 Year Wise Trend Of Units Registered 08 3.3 Details Of Existing Micro & Small Enterprises & Artisan Units 09 In The District 3.4 Large Scale Industries / Public Sector undertakings 09 3.5 Major Exportable Item 09 3.6 Growth Trend 10 3.7 Vendorisation / Ancillarisation of the Industry 10 3.8 Medium Scale Enterprises 10 3.8.1 List of the units in Tikamgarh & near by Area 10 3.8.2 Major Exportable Item 11 3.9 Service Enterprises 11 3.9.2 Potentials areas for service industry 11 3.10 Potential for new MSMEs 11 4. Existing Clusters of Micro & Small Enterprise 11 5. General issues raised by industry association during the course of 12 meeting 6 Prospects of training Programmes during 2012-13 12 7. Action plan for MSME Schemes during 2012-13 13 8. -

Ken- Betwa Link Project, Phase-I
VOLUME - III KEN- RESETTLEMENT AND REHABILITATON: PROJECT AFFECTED FAMILIES BETWA ECONOMIC REHABILITATION PLAN (PAFERP) LINK PROJECT, PHASE-I Submitted to NATIONAL WATER DEVELOPMENT AGENCY (NWDA) Prepared by RESETTLEMENT AND REHABILITATON PLAN AGRICULTURAL FINANCE CORPORATION LTD, (R&R) MUMBAI, INDIA December, 2014 INDIA NATIONAL WATER DEVELOPMENT AGENCY (A Govt. of India society under Ministry of Water Resources) COMPREHENSIVE ENVIRONMENT IMPACT ASSESSMENT STUDY OF PROPOSED KEN-BETWA LINK PROJECT PHASE-I VOLUME – III RESETTLEMENT AND REHABILITATON: PROJECT AFFECTED FAMILIES ECONOMIC REHABILITATION PLAN (PAFERP) as per “The Right to Fair Compensation and Transparency in Land Acquisition, Rehabilitation and Resettlement Act 2013”. CONTENTS Chapter No. Title Page(s) I Introduction 1-3 II Socio – Economic Status in Command Area 4-18 III Socio-Economic Environment in Submergence Area 19-27 IV Resettlement and Economic Rehabilitation Plan 28-39 V Training 40-43 VI Organization and Management 44-49 VII Monitoring and Evaluation 50-53 VIII Implementation Schedule 54-55 IX Project Cost 56-57 Annexures Annexure Title Page No. No. II.1 Existing Cropping Pattern in the Command Area 58 II.2 Existing Crop Production in the Command Area 59 II.3 Agriculture Input Pattern and Economics of Cultivation in the 60-63 Command Area III.1 Demography Population of Project Affected Families 64 III.3 Caste-wise distribution of Households and its Population in the 65 Project Submergence Areas IV.1 Details of Land Acquisition of Daudhan dam, Link Canal, LBC 66-67 system and power houses CHAPTER - I INTRODUCTION Background 1.01 While the projects are the building blocks for development, the irrigation reservoir projects at times result in submersion of houses and house sites rendering people homeless besides causing loss of valuable agricultural land affecting the over all social fabric of the affected people. -

District Survey Report
DISTRICT SURVEY REPORT CHAPTER-I INTRODUCTION- Ministry of environment, forest and climate change vide notification dated 15th January 2016, New Delhi has made mandatory for mining of minor minerals irrespective of the area of mining lease, to obtain environmental clearance before mining, in this respect state govt. has set up two bodies DEIAA and DEAC which will meet once in every month and the members of this committee will recommend/scrutnize the mining plan/environmental clearance of the minor minerals. This will be done on the basis of district survey report in which all the important factors shall be taken into consideration regarding land use, reserves, mineral-availability, deposition, infrastructure, distance prohibition, annual deposition and time taken for replenishment etc, This district survey report will be an important too for the guidance, assessment and sanction for giving environment clearance to the said mine plan of the minor mineral or if any correction or so is needed in the said mine plan. The district lies between longitude 23045' N to 250 09'N and latitude 79045'E to 800 45'E of sagar division. It is the northern most part of the division. It is covered by toposheet no. 55M, 54P, 63C, 63D and 64A. It is located 70 km. west from WC Rly station Satna, by all fair weather road NH-75 and nearest airport at a distance of 40km. from district HQ. 1 2 An area of 246951 Hect. i.e., about 35% of the area of the district is covered under the government forests. Administratively, the forests are divided into two divisions and 14 ranges. -

ANSWERED ON:21.11.2007 PENDING LAKE CONSERVATION PROJECTS Singh Shri Chandrabhan Bhaiya
GOVERNMENT OF INDIA ENVIRONMENT AND FORESTS LOK SABHA UNSTARRED QUESTION NO:635 ANSWERED ON:21.11.2007 PENDING LAKE CONSERVATION PROJECTS Singh Shri Chandrabhan Bhaiya Will the Minister of ENVIRONMENT AND FORESTS be pleased to state: (a) whether proposals worth Rs.1.36 crores for Benisagar in Panna district and Puraina Pond in Damoh district under the National Pond and Lake conservation Project sent by the Government of Madhya Pradesh to the Union Government are pending; (b) if so, the time by when these proposals are likely to be accorded approval; (c) whether proposals of various schemes pertaining to other districts of Madhya Pradesh are also under consideration of Ministry of Environment and Forests; and (d) if so, the State-wise details thereof? Answer MINISTER OF THE STATE IN THE MINISTRY OF ENVIRONMENT & FORESTS (SHRI NAMO NARAIN MEENA) (a) to (d) The Lake Conservation Authority of Madhya Pradesh had submitted the proposals on 'Conservation and Management Plan of Beni Sagar Lake' in Panna District and 'Conservation & Management Plan of Purena Talab' in District Damoh (MP) to this Ministry for consideration under the National Lake Conservation Plan, a Centrally Sponsored Scheme for restoration of polluted and degraded lakes in urban & semi-urban areas. In order to consider the proposals under National Lake Conservation Plan, the Ministry had identified certain lakes through a study. The State Governments were asked to consider these lakes for prioritization. The Benisagar Lake was neither identified by this Ministry nor included in the priority of the State Government for consideration under the National Lake Conservation Plan. The proposal for Purena Talab was found deficient in respect of certain key technical issues.