21 December 2016
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Southern Conference Cross Country Record Book
Southern Conference Cross Country Record Book www.soconsports.com 1 Men’s Team & Individual Champions Year Site Team Champion, Score Individual Champion Time 1926 Athens, Ga. North Carolina 33 Galen Elliot, North Carolina 1927 Chapel Hill, N.C. North Carolina 17 Galen Elliot, North Carolina 26:26.0 1928 Atlanta, Ga. North Carolina 30 Bob Young, Georgia 24:30.8 1929 Chapel Hill, N.C. North Carolina 56 Bob Young, Georgia 26:58.2 1930 Chapel Hill, N.C. VMI 40 Ham Smith & H.A. Wise, VMI 28:03.4 1931 Chapel Hill, N.C. North Carolina 25 Clarence Jensen, North Carolina 27:10.2 1932 Chapel Hill, N.C. Duke 23 Jerry Bray & Bob Bird, Duke 27.21.6 1933 Chapel Hill, N.C. Duke 23 Dunaj, Washington & Lee 15:27.8 1934 Chapel Hill, N.C. North Carolina 31 Ed McRae, North Carolina 26.41.6 1935 Chapel Hill, N.C. Duke 26 Bill Morse, Duke 26:25.9 1936 Chapel Hill, N.C. North Carolina 32 Bill Morse, Duke 25:34.0 1937 Chapel Hill, N.C. North Carolina 27 Bill Hendrix, North Carolina 25:35.4 1938 Chapel Hill, N.C. North Carolina 28 Bill Hendrix, North Carolina 25:25.7 1939 Chapel Hill, N.C. North Carolina 18 Fred Hardy, North Carolina 26:29.8 1940 College Park, Md. North Carolina 33 Tommy Fields, Maryland 26:08.6 1941 College Park, Md. North Carolina 45 Wendell Lockwood, Duke 21:06.2 1942-45 NO MEET 1946 Chapel Hill, N.C. North Carolina 33 Jimmy Miller, North Carolina 20:00.3 1947 College Park, Md. -

Extras - Episode One
Extras - Episode One by Ricky Gervais & Stephen Merchant COLD OPEN FADE IN: We are watching a TV biopic of the life of Lord Nelson. It is England, 1805. Lady Hamilton is running across a lawn towards a carriage that is being loaded by manservants. ROSS KEMP as Horatio Nelson is standing nearby. LADY HAMILTON Horatio. Ross turns to face Lady Hamilton. ROSS Emma. What are you doing here? LADY HAMILTON I couldn't bear to let you go without saying goodbye. ROSS You shouldn't have come, Emma. People will talk. LADY HAMILTON Let them talk. I'm tired of hiding our love away. I'm not ashamed of how I feel. We cut behind the scenes to see ANDY MILLMAN waiting off camera, dressed as a footman. He is watching the action, waiting for his cue. ROSS Neither am I. But we both know we shouldn't be together. LADY HAMILTON Shouldn't? Who says we shouldn't? Behind the scenes, Andy is tapped on the shoulder. He walks forward and loads his crate onto the back of the carriage. We see him appear in the background of the film clip. ROSS My conscience. My conscience tells me everything I feel for you is wrong. But my heart, my heart says I can't live without you. Andy stands by the carriage. LADY HAMILTON Promise me you'll return. ROSS I promise. Because if Napoleon doesn't kill me, then being away from you surely will. 2. Ross and Lady Hamilton kiss passionately. From behind their heads we see Andy emerge, edging himself into the frame. -

Ben's Dad on Secret Life.Pdf
Ben's Dad On Secret Life All he really wanted was to sleep with Adrian Lee and continue his life like usual. Both Adrian and Ben thought that Ricky and Amy had done much more. 'Secrets & Lies' Post-Show Reveals Final Shocker: Is Ben Dead? – Watch 'Revenge' Recap: (SPOILER) Dies After Discovering A Huge Secret I think he is just in Jail some where far away since he did “kill” a child he has life in prison. In the season one episode The Secret Wedding of the American Teenager, Ben and Amy Ben's dad and Dylan's parents catch Dylan and her friends smoking. My dad and I picked it out, this past Weekend", Ben said, in agreement, looking around the interior of the vehicle with awe. "When I get my driver's license, we're. Adrian and Ben had a one night stand in The Rhythm of Life which resulted in Adrian's dad doesn't know about her pregnancy, but Adrian wants to tell her. Ben Affleck had an ancestor who was a slaveowner and he actively sought to keep so public as Ben Affleck the media loves dirt and they would make his life miserable. I did not own slaves, my dad did not own slaves, nor my grandfather. Ben's Dad On Secret Life >>>CLICK HERE<<< The Secret Life of the American Teenager The Suite Life of Zack and Cody Ben becomes a surprise dad to a baby girl when she's left on his doorstep. Seemingly good-natured painter Ben Crawford (MacGruber's Ryan Still, plenty of people have played cops with no back story and no life outside the got the same feeling about the youngest like she knows her dad is guilty because she. -

Download the Activity Sheet As A
Fill up your week with these free fun art activities! Every Monday, National Galleries of Scotland posts a new set of creative activities that have been designed for children of all ages to explore at their own pace. And, of course, grown-ups can join in too – especially with the mid-week #ArtTogether activities! These wee taster activities require absolutely NO ART MATERIALS – just a little bit of imagination and a lot of creativity. They aim to develop creativity skills, such as problem solving, imagination, curiosity and open-mindedness. Please keep in mind that there are no wrong answers - this is all about looking, chatting, making and enjoying your time together at home! Visit nationalgalleries.org to see the activities, artist videos, zoom in on artworks and more – or work your way through these PDF versions! We’d love to see the great art you make at home, and to hear how you’re getting on so please share your photos on our Facebook page or by using #HomeArt on Twitter or Instagram! HOME IS WHERE THE ART IS Week Three: ‘Everything is going to be alright’ Cold War Steve, Harold, the Ghost of Lost Futures, 2019 The inspiration for this week is the collage ‘Harold, the Ghost of Lost futures’ by the artist Cold War Steve. He created the work by collecting images of celebrities and creating a surreal scene which you would never see in real life! His real name is Christopher Spencer. Choose your own ‘artist’ name before you start this week's activities! HOME IS WHERE THE ART IS Week Three: ‘Everything is going to be alright’ 1. -

Report Title Here Month Here
Alcohol & Soaps Drinkaware Media Analysis September 2010 © 2010 Kantar Media 1 CONTENTS •Introduction 3 •Executive Summary 5 •Topline results 7 •Coronation Street 16 •Eastenders 23 •Emmerdale 30 •Hollyoaks 37 •Appendix 44 Please use hyperlinks to quickly navigate this document. © 2010 Kantar Media 2 INTRODUCTION •Kantar Media Precis was commissioned to conduct research to analyse the portrayal of alcohol and tea in the four top British soap operas aired on non-satellite television, Coronation Street, Eastenders, Emmerdale and Hollyoaks. The research objectives were as follows: •To explore the frequency of alcohol use on British soaps aired on non-satellite UK television •To investigate the positive and negative portrayal of alcohol •To explore the percentage of interactions that involve alcohol •To explore the percentage of each episode that involves alcohol •To assess how many characters drink over daily guidelines •To explore the relationship between alcohol and the characters who regularly/excessively consume alcohol •To look further into the link between the location of alcohol consumption and the consequences depicted •To identify and analyse the repercussions, if any, of excessive alcohol consumption shown •To explore the frequency of tea use on British soaps aired on non-satellite UK television •Six weeks of footage was collected for each programme from 26th July to 6th September 2010 and analysed for verbal and visual instances of alcohol and tea. •In total 21.5 hours was collected and analysed for Emmerdale, 15.5 hours for Coronation Street, 15.5 hours for Hollyoaks and 13 hours for Eastenders. © 2010 Kantar Media 3 INTRODUCTION cont. •A coding sheet was formulated in conjunction with Drinkaware before the footage was analysed which enabled us to track different types of beverages and their size (e.g. -

20 February 2015
20 FEBRUARY 2015 30 years to the day EastEnders was first broadcast, one of EastEnders true icons, Kathy Beale returned to the show in a LIVE scene in last night’s episode in the UK, which will air in Australia on the 4th March on UKTV at 6.15pm. Last seen in 2000 before returning to South Africa, viewers believed that Kathy was killed in a car crash. However when Kathy comes home to Walford later this year, viewers will learn where Kathy has been and why she has stayed away so long… Played by Gillian Taylforth, Kathy appeared in the very first episode of EastEnders on the 19th February 1985. As one of the original cast, Gillian soon found herself at the heart of some of the soaps most memorable episodes, creating a character that has never been forgotten in EastEnders history. Storylines included her relationship and subsequent turbulent marriage to Phil Mitchell and the rape of Kathy by Wilmott Brown. Kathy’s return has been shrouded in secrecy. To keep her return under wraps the scenes were shot live on location to prevent her being seen prior to her episode transmitting. Talking about her return to EastEnders, Gillian said “When Dominic approached me with his plan, I was so shocked I got into my car and burst into tears! ‘Kathy’ has always been so close to my heart and it’s absolutely wonderful to be returning to the show and reprising the role” Dominic Treadwell-Collins, Executive Producer said “I have always made my feelings on Kathy Beale and Gillian Taylforth very clear – she is part of EastEnders history, mother to Ian and Ben and one of the most important and iconic television characters on British television. -

1.1 My Qualifications I Am Alfie Moon, MBCS. I Work As a Director for The
1.1 My Qualifications I am Alfie Moon, MBCS. I work as a Director for The Queen Victoria PH plc, an IT business Management Consultancy. I have worked for The Queen Victoria PH since 1997 and prior- to that I was a Director of Angie's Den. As a consultant my primary fields of activity are project and organisational effectiveness reviews, in a variety of technical environments and the production of expert reports under Civil Procedure Rules. I am a member of the British Computer Society. I have worked full-time in the IT industry since 1963. Over this period I have been a programmer, designer, analyst, team leader, project manager and line manager responsible for several hundred staff. I have always, professionally and personally, been an advocate for, and a user of, the PC and internet environment. I have written code, reviewed organisational intra/internets and developed web sites. 1.2 The Charges I have taken the charges from the Indictment and have addressed the 18 counts individually in the section on findings. Note that these charges all address the possession of indecent photographs of children, not of making them. I have not addressed the issue of whether such photographs were made by Dermis Watts. 1.3 Questions addresses I was given the following instructions and have responded as indicated in italics • Nothing that the prosecution expert computer witness asserts in his witness statement should be taken at face value. The evidence presented by Grant Mitchell and DC Phil Mitchell has been reviewed and verified by examination of the floppy disks and computer hard disk. -

SATURDAY 22ND JULY 06:00 Breakfast 10:00 Saturday Kitchen
SATURDAY 22ND JULY All programme timings UK All programme timings UK All programme timings UK 06:00 Breakfast 08:25 ITV News 09:50 The Goldbergs 06:00 British Forces News 10:00 Saturday Kitchen Live 08:30 Weekend 10:15 Real Housewives of Cheshire 06:30 Walks Around Britain 11:30 Nadiya's British Food Adventure 09:25 The Home Game 11:05 Buffy the Vampire Slayer 07:00 Flying Through Time 12:00 Bargain Hunt 10:25 The Voice Kids Final 11:55 The Joy of Techs 07:30 Wish Me Luck 13:00 BBC News 12:10 ITV News 12:20 Scrubs 08:30 Dogfights 13:15 Athletics: Diamond League Monaco 12:25 Chelsea v Arsenal Live 12:45 Scrubs 09:30 UFO Highlights 14:55 Tipping Point 13:05 Shortlist 10:30 Hogan's Heroes 14:15 Escape to the Country 16:00 The Chase 13:10 Baby Daddy 11:00 Hogan's Heroes 15:00 Flog It! 17:00 Little Big Shots USA 13:35 Baby Daddy 11:30 Hogan's Heroes 15:30 Kung Fu Panda 2 18:00 ITV News London 13:55 The Big Bang Theory 12:00 Hogan's Heroes 16:50 Shrek the Third 18:10 ITV News 14:20 The Big Bang Theory 12:35 Hogan's Heroes 18:15 BBC News 18:20 You've Been Framed! XXL 14:45 The A-Team 13:00 UFO 18:25 BBC London News 19:20 Catchphrase 15:35 The Middle 14:00 Defending the Nation 18:35 Pointless Celebrities Stephen Mulhern hosts the popular game show in 16:00 Binky and JP's Baby: Born in Chelsea 14:30 Get Smart 19:25 Pitch Battle which three players compete to guess the 16:50 Four Weddings 15:00 Get Smart It is the live final. -
SSE QUIZ Round 1 - OLDER OR YOUNGER (Questions & Answers)
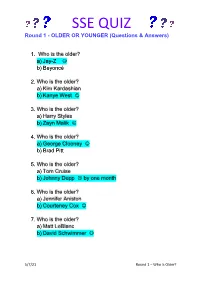
SSE QUIZ Round 1 - OLDER OR YOUNGER (Questions & Answers) 1. Who is the older? a) Jay-Z b) Beyoncé 2. Who is the older? a) Kim Kardashian b) Kanye West 3. Who is the older? a) Harry Styles b) Zayn Malik 4. Who is the older? a) George Clooney b) Brad Pitt 5. Who is the older? a) Tom Cruise b) Johnny Depp by one month 6. Who is the older? a) Jennifer Aniston b) Courteney Cox 7. Who is the older? a) Matt LeBlanc b) David Schwimmer 5/7/21 Round 1 – Who Is Older? SSE QUIZ 8. Who is the older? a) Boris Johnson b) David Cameron 9. Who is the older? a) Harry Maguire b) Harry Kane 10. Who is the older? a) Steve McFadden ( Phil Mitchell, EastEnders) b) Ross Kemp ( Grant Mitchell, EastEnders) 11. Who is the Older? a) June Brown (Dot Cotton, EastEnders) b) William Roach ( Coronation Street) 12. Who is the older? a) Jeff Hordley (Cain Dingle, Emmerdale) b) Mark Charnock (Marlon Dingle, Emmerdale) 13. Who is the older? a) Christopher Chittell (Eric Pollard, Emmerdale) b) Lesley Dunlop (Brenda Walker, Emmerdale) 14. Who is the older? a) Paul McCartney b) Ringo Starr 5/7/21 Round 1 – Who Is Older? SSE QUIZ ROUND 2 - GENERAL KNOWLEDGE (Questions and Answers) 1. Which month of the year has the least number of days? a) February b) March 2. What is a group of lions called? a) Herd b) Pride 3. What do camels store in their humps? a) Water b) Fat 4. What is the slowest animal in the world? a) Three-toed sloth b) Slow worm 5. -

Thesis Final Draft.Pages
CORE Metadata, citation and similar papers at core.ac.uk Provided by Glasgow Theses Service Bell, Stuart (2016) "Don't Stop": Re-Thinking the Function of Endings in Narrative Television. PhD thesis http://theses.gla.ac.uk/7282/ Copyright and moral rights for this thesis are retained by the author A copy can be downloaded for personal non-commercial research or study, without prior permission or charge This thesis cannot be reproduced or quoted extensively from without first obtaining permission in writing from the Author The content must not be changed in any way or sold commercially in any format or medium without the formal permission of the Author When referring to this work, full bibliographic details including the author, title, awarding institution and date of the thesis must be given. Glasgow Theses Service http://theses.gla.ac.uk/ [email protected] “Don’t Stop…” Re-thinking the Function of Endings in Narrative Television Stuart Bell (MA, MLitt) Submitted in fulfilment for the requirements for the degree of Doctor Of Philosophy School of Culture and Creative Arts College of Arts University of Glasgow November 2015 (c) Stuart Bell, November 2015 !1 Abstract “Don’t Stop…” Re-thinking the Function of Endings in Television This thesis argues that the study of narrative television has been limited by an adherence to accepted and commonplace conceptions of endings as derived from literary theory, particularly a preoccupation with the terminus of the text as the ultimate site of cohesion, structure, and meaning. Such common conceptions of endings, this thesis argues, are largely incompatible with the realities of television’s production and reception, and as a result the study of endings in television needs to be re-thought to pay attention to the specificities of the medium. -

How Britain Worked Free
FREE HOW BRITAIN WORKED PDF Guy Martin | 256 pages | 05 Nov 2012 | Ebury Publishing | 9780753540848 | English | London, United Kingdom Long Live Britain review - Time Out London By entering your email address you agree to our Terms of Use and Privacy Policy and consent to receive emails from Time Out about news, events, offers and partner promotions. Thanks for subscribing! Look out for your first newsletter in your inbox soon! Heads up! Most were created in the nineteenth century, when the hedonism of the Georgian and Regency eras gradually gave way to the self-denial of the uptight Victorian period, while a fashion for seventeenth-century Dutch How Britain Worked ensured that tavern scenes were all the rage in British art. People used to get through the How Britain Worked phenomenal amounts of port. People were completely pickled in it. This was in the lead up to the Gin Act which, later incurtailed the number of unlicensed drinking establishments. Hogarth was moralising but he was a narrative artist as How Britain Worked. The whole thing is completely over the top, but it has to be to make its point. There are at least a hundred How Britain Worked scenes going on: drunken schoolmasters, drunken famililes, people drunk in the streets, people too drunk to work in the factories and mills in the background. It sounds a bit like overjustification, but he was quite damaged by drink because his father, who was also an artist, died in a drinking competition, just completely blew up and dropped dead, when George was very young. -

Amy Oliver Email : [email protected]
Amy Oliver Email : [email protected] 11th March 2010 Dear Amy Oliver, Freedom of Information request – RFI20100300 Thank you for your request to the BBC of 26th February 2010, seeking the following information under the Freedom of Information Act 2000: 1. How much was the final technical budget for the live version of Eastenders on Friday February 19 2010 and did the actual event exceed this? 2. How many cameras were used to film the live version of Eastenders on Friday February 19 2010? 3. How many crew members were there involved on the live version of Eastenders on Friday February 19 2010? 3. How much were the artists' fees for the live version of Eastenders on Friday February 19 2010. 4. Were the artists' fees higher for the live version of Eastenders on February 19 2010 than they are for regular episodes? 5. Please provide a breakdown of the following artists fees for the live version of Eastenders: Peggy Mitchell - Barbara Windsor Jack Branning - Scott Maslen Ronnie Mitchell - Samantha Womack Stacey Slater - Lacey Turner Janine Butcher - Charlie Brookes Max Branning - Jake Wood Bradley Branning - Charlie Clements Ian Beale - Adam Woodyatt Phil Mitchell - Steve McFadden 6. How much did the after/wrap party cost following the live version of Eastenders on February 19 2010? 7. What is the per episode cost of a regular episode of Eastenders. 8. How much did the live version of Eastenders on February 19 2010 cost the licence fee payer in total? The information you have requested in questions numbered 1-5, 7 and 8 are excluded from the Act because it is held for the purposes of ‘journalism, art or literature.’ The BBC is therefore not obliged to provide this information to you and will not be doing so on this occasion.