Journal of Adolescent Research
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Why Do We Need a Social Psychiatry? Antonio Ventriglio, Susham Gupta and Dinesh Bhugra
The British Journal of Psychiatry (2016) 209, 1–2. doi: 10.1192/bjp.bp.115.175349 Editorial Why do we need a social psychiatry? Antonio Ventriglio, Susham Gupta and Dinesh Bhugra Summary interventions in psychiatry should be considered in the Human beings are social animals, and familial or social framework of social context where patients live and factors relationships can cause a variety of difficulties as well as they face on a daily basis. providing support in our social functioning. The traditional way of looking at mental illness has focused on abnormal Declaration of interest thoughts, actions and behaviours in response to internal D.B. is President of the World Psychiatric Association. causes (such as biological factors) as well as external ones such as social determinants and social stressors. We Copyright and usage contend that psychiatry is social. Mental illness and B The Royal College of Psychiatrists 2016. and difficulties at these levels can lead to psychopathological Antonio Ventriglio (pictured) is an honorary researcher at the Department of and behavioural dysfunctions. Social stressors can lead to changes Clinical and Experimental Medicine at the University of Foggia, Italy. Susham 5 Gupta is a consultant psychiatrist at the East London Mental Health in the cerebral structure and affect neuro-hormonal pathways. Foundation NHS Trust. Dinesh Bhugra is Emeritus Professor of Mental Health Even organic conditions such as dementia are said to be related to & Cultural Diversity at the Institute of Psychiatry, Psychology & Neuroscience, life events and social factors such as economic and educational status.5 King’s College London and is President of the World Psychiatric Association. -

The ICD-10 Classification of Mental and Behavioural Disorders Diagnostic Criteria for Research
The ICD-10 Classification of Mental and Behavioural Disorders Diagnostic criteria for research World Health Organization Geneva The World Health Organization is a specialized agency of the United Nations with primary responsibility for international health matters and public health. Through this organization, which was created in 1948, the health professions of some 180 countries exchange their knowledge and experience with the aim of making possible the attainment by all citizens of the world by the year 2000 of a level of health that will permit them to lead a socially and economically productive life. By means of direct technical cooperation with its Member States, and by stimulating such cooperation among them, WHO promotes the development of comprehensive health services, the prevention and control of diseases, the improvement of environmental conditions, the development of human resources for health, the coordination and development of biomedical and health services research, and the planning and implementation of health programmes. These broad fields of endeavour encompass a wide variety of activities, such as developing systems of primary health care that reach the whole population of Member countries; promoting the health of mothers and children; combating malnutrition; controlling malaria and other communicable diseases including tuberculosis and leprosy; coordinating the global strategy for the prevention and control of AIDS; having achieved the eradication of smallpox, promoting mass immunization against a number of other -

The ICD-10 Classification of Mental and Behavioural Disorders
The ICD-10 Classification of Mental and Behavioural Disorders Clinical descriptions and diagnostic guidelines World Health Organization -1- Preface In the early 1960s, the Mental Health Programme of the World Health Organization (WHO) became actively engaged in a programme aiming to improve the diagnosis and classification of mental disorders. At that time, WHO convened a series of meetings to review knowledge, actively involving representatives of different disciplines, various schools of thought in psychiatry, and all parts of the world in the programme. It stimulated and conducted research on criteria for classification and for reliability of diagnosis, and produced and promulgated procedures for joint rating of videotaped interviews and other useful research methods. Numerous proposals to improve the classification of mental disorders resulted from the extensive consultation process, and these were used in drafting the Eighth Revision of the International Classification of Diseases (ICD-8). A glossary defining each category of mental disorder in ICD-8 was also developed. The programme activities also resulted in the establishment of a network of individuals and centres who continued to work on issues related to the improvement of psychiatric classification (1, 2). The 1970s saw further growth of interest in improving psychiatric classification worldwide. Expansion of international contacts, the undertaking of several international collaborative studies, and the availability of new treatments all contributed to this trend. Several national psychiatric bodies encouraged the development of specific criteria for classification in order to improve diagnostic reliability. In particular, the American Psychiatric Association developed and promulgated its Third Revision of the Diagnostic and Statistical Manual, which incorporated operational criteria into its classification system. -

WPA NEWS January 2017 General Matters of WPA (Including Regional, International and World Congress Announcements)
WPAOfficial Quarterly NewsNEWS Bulletin of WPA JANUARY 2017 WWW.WPANET.ORG Message from the Secretary General Message from the President Dear Colleagues and Friends, Delighted to keep in touch with you! WPA had Dinesh Bhugra a very active period dur- ing the last three months. The Second World Mind Matters Day on 5th children and young people. Developed by The most important event September saw the launch of the WPA Report Dr Gordana Milavic and Professor Bennet Roy Abraham Kallivayalil was the WPA Internation- on Social Discrimination against individuals Leventhal and colleagues, it is available on the al Congress, Cape Town, with mental illness. This report was launched WPA website. November 18- 22, 2016. Theme: “Psychiatry: Inte- formally in the House of Lords in London. A Bill grative Care for the Community”. With more than of Rights for people with mental illness was also WPA-Lancet commission on Psychiatry report 2,000 delegates attending, it was one of the most out- launched. It has the support of 61 international is expected to be published by Lancet Psychiatry standing WPA Congresses ever held in Africa. The organisations and if your organisation has not early next year. WPA Executive Committee, the Council and the signed this please add your support. Board also met at Cape Town and considered sev- Recent Position Statements include one on eral matters concerning mental health and our Asso- Full details of the discrimination survey were environmental sustainability and on high quality ciation. Hearty congratulations to the South African published in a special issue of International training. Society of Psychiatrists, Bernard van Rensburg and Review of Psychiatry volume 28(4). -

Social Media and Its Connection to the Development of Eating Disorders
SOCIAL MEDIA AND ITS CONNECTION TO THE DEVELOPMENT OF EATING DISORDERS A thesis submitted to the Kent State University Honors College in partial fulfillment of the requirements for University Honors By Kara L. Kimevski December, 2017 Thesis written by Kara Kimevski Approved by _______________________________________________________________, Advisor ____________________________________________, Chair, Department of Psychology Accepted by ____________________________________________________, Dean, Honors College ii TABLE OF CONTENTS AKNOWLEDGMENTS………………………………………………………………….iv CHAPTER I. ABSTRACT…………………………………………………………………...1 II. INTRODUCTION………………………………………………………….....2 III. SOCIAL MEDIA……………………………………………………………...7 IV. EATING DISORDERS……………………………………………………...12 Types of Eating Disorders…………………………………………………...12 Health Effects of Eating Disorders……………………………………….….14 Comorbidity………………………………………………………………….15 Shame and Self-Criticism.…………………………………………………...16 V. SOCIAL MEDIA AND EATING DISORDERS……………………………18 Websites Promoting Eating Disorders……………………………………….18 Thinspiration…………………………………………………………………23 Tagging…………………………………………………………………..24 VI. THEORIES…………………………………………………………………..27 Uses and Gratification Approach…………………………………………….27 Cultivation Theory…………………………………………………………...29 Social Comparison Theory…………………………………………………..29 Social Identity Theory………………………………………………………..33 iii Objectification Theory……………………………………………………….34 Social Cognitive Theory……………………………………………………..35 VII. EFFECTS OF SOCIAL MEDIA ON DIFFERENT GROUPS……………...38 Women…………………….............................................................................38 -

Psychiatry and Narcology
Ministry of Health of Ukraine Ministry of Education and Science of Ukraine Kharkiv National Medical University V. N. Karazin Kharkiv National University PSYCHIATRY AND NARCOLOGY Tutorial for forieng medium students of higher medical schools and interns PSYCHIATRY AND NARCOLOGY: підручник для студентів медичних університетів та лікарів інтернів Recommended by KhNMU Academic Councile Protocol № 6 of 26.06.2020. Authors: Kozhyna H., Mishchenko Т., Maruta N., Gaichuk L., Haydabrus A., Korostiy V., Korovina L., Koshchii V., Leshchyna I., Minko O., Radchenko T., Semikina O., Sinaiko V., Shtryhol D., Skrynnyk O., Strelnikova I., Tieroshyna I., Vovk V., Zelenska K. Authors: Hanna M. Kozhyna Professor MD, PhD, DMSc Head of Department of Psychiatry, Narcology, Medical Psychology and Social Work Kharkiv National Medical University Tamara S. Mishchenko Professor MD, PhD, DMSc Head of Department of Clinical Neurology, Psychiatry and Narcology V. N. Karazin Kharkiv National University Nataliya O. Maruta Professor MD, PhD, DMSc Deputy Director on Scientific Work , Chief of Borberline Psychiatry Department of the Institute of Neurology, Psychiatry and Narcology of the NAMS of Ukraine Larysa M. Gaichuk MD, PhD, Associate Professor of the Department of Psychiatry, Narcology, Medical Psychology and Social Work Kharkiv National Medical University Andriy V. Haydabrus MD, PhD, Associate Professor of the Department of Clinical Neurology, Psychiatry and Narcology V. N. Karazin Kharkiv National University Volodymyr I. Korostiy Professor MD, PhD, DMSc, Professor of Department of Psychiatry, Narcology, Medical Psychology and Social Work Kharkiv National Medical University Liliia D. Korovina MD, PhD, Associate Professor of the Department of Psychiatry, Narcology, Medical Psychology and Social Work Kharkiv National Medical University Vladislava O.Koshchii MD, Assistant of Department of Psychiatry, Narcology, Medical Psychology and Social Work Kharkiv National Medical University Iryna V. -

Religions and Psychotherapies
Religions and Psychotherapies Edited by Prof. Dr. Klaus Baumann and Prof. Dr. Frank-Gerald B. Pajonk Printed Edition of the Special Issue Published in Religions www.mdpi.com/journal/religions Prof. Dr. Klaus Baumann and Prof. Dr. Frank-Gerald B. Pajonk (Eds.) Religions and Psychotherapies This book is a reprint of the Special Issue that appeared in the online, open access journal, Religions (ISSN 2077-1444) from 2011–2012 (available at: http://www.mdpi.com/journal/religions/special_issues/religions-psychotherapies). Guest Editors Klaus Baumann Caritaswissenschaft und Christliche Sozialarbeit, Theologische Fakultät Albert-Ludwigs-Universität Freiburg, Germany Frank-Gerald B. Pajonk Praxis Isartal, Kloster Schäftlarn, Germany Klinik für Psychiatrie und Psychotherapie, Georg-August Universität Göttingen, Germany Editorial Office MDPI AG Klybeckstrasse 64 Basel, Switzerland Publisher Shu-Kun Lin Managing Editor Jeremiah R. Zhang 1. Edition 2014 MDPI • Basel • Beijing • Wuhan • Barcelona ISBN 978-3-906980-77-5 (Hbk) ISBN 978-3-906980-78-2 (PDF) Articles in this volume are Open Access and distributed under the Creative Commons Attribution license (CC BY), which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited, which ensures maximum dissemination and a wider impact of our publications. The book taken as a whole is © 2014 MDPI, Basel, Switzerland, distributed under the terms and conditions of the Creative Commons by Attribution (CC BY-NC-ND) license (http://creativecommons.org/licenses/by-nc-nd/4.0/). III Table of Contents List of Contributors ............................................................................................................................. V Preface............................................................................................................................................. XV Editorial Religions 2014, 5(3), 871–875; doi:10.3390/rel5030871 ................................................................. -

What Research Is Needed in Social Psychiatry?
Moussaoui Annals of General Psychiatry 2010, 9(Suppl 1):S57 http://www.annals-general-psychiatry.com/content/9/S1/S57 MEETING ABSTRACT Open Access What research is needed in social psychiatry? Driss Moussaoui From 1st International Congress on Neurobiology and Clinical Psychopharmacology and European Psychiatric Association Conference on Treatment Guidance Thessaloniki, Greece. 19-22 November 2009 There is no such a thing as psychiatry without a social component. If the XIXth Century has been mostly dedicated to clinical descriptions and classification, if the XXth Century has been mostly therapeutic (psychotherapies, psychopharmacology and biological psychiatry), it is highly probable that the XXIst Century will be mostly oriented towards psycho-social psychiatry and mental health. Research will be an essential part of this evolution. There is also an urgent need of education of young promising psychiatrists, learning the complexity of inter- actions between the psycho-social aspect and the biolo- gical one in psychiatry, but also the necessity using of a rigorous methodology. There are plenty of topics which need to be investi- gated in social psychiatry. Some of the most important are: - Migration and mental health, especially on the see- mingly higher prevalence of schizophrenia among some groups of migrants; - Religion, spirituality and mental health; as a matter of fact, they will play an increasing role in the future in the expression of psychopathology, and in psycho-social phenomena such as violence, substance abuse... -Women’s mental health, especially peri-natal mental health and psychiatry; - Ethics and its relative relativity from one culture to another in psychiatric daily practice. Submit your next manuscript to BioMed Central and take full advantage of: Published: 22 April 2010 • Convenient online submission • Thorough peer review doi:10.1186/1744-859X-9-S1-S57 • No space constraints or color figure charges Cite this article as: Moussaoui: What research is needed in social psychiatry?. -
Preventive Social Psychiatry and Command Consultation: Who Is the Patient— the Soldier Or His Military Unit?
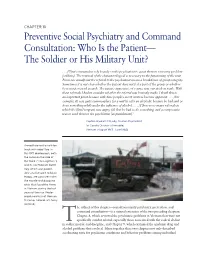
CHAPTER 10 Preventive Social Psychiatry and Command Consultation: Who Is the Patient— The Soldier or His Military Unit? . [U]nit commanders rely heavily on the psychiatrist to assist them in removing problem [soldiers]. The removal of the characterological is necessary to the functioning of the unit. From one standpoint the referral to the psychiatrist means a breakdown of group integrity. Sometimes it is not clear whether the patient does not feel a part of the group or whether he is not perceived as such. The passive aggressive, of course, was our stock in trade. With these referrals I had to consider whether the referral was honestly made. I think this is an important point because with time people’s secret motives become apparent. [For example, it] was quite commonplace for a unit to refer an alcoholic because he had said or done something while under the influence of alcohol. [T]here were many referrals in which the [first] sergeant was angry, felt that he had to do something, and a compromise was to send them to the psychiatrist [as punishment].1 Captain Harold SR Byrdy, Division Psychiatrist 1st Cavalry Division (Airmobile) Vietnam (August 1965–June 1966) Armed two-and-a-half-ton truck with rebel flag. In this 1971 photograph, both the name on the side of the truck (“The Fugitives”) and its Confederate battle flag, which was predict- ably a racist taunt to black troops, are consistent with the morale and discipline crisis that faced the Army in Vietnam during the last years of the war. Photo- graph courtesy of Norman M Camp, Colonel, US Army (Retired). -

Subject and Tasks of Psychiatry and Narcology. Organization of Care for Patients with Mental Disorders
UKRAINIAN MEDICAL STOMATOLOGICAL ACADEMY Department of Psychiatry, Narcologyand Medical Psychology Subject and tasks of psychiatry and narcology. Organization of care for patients with mental disorders. General principles of treatment, rehabilitation and examination of mental illnesses and disorders. Lecturer – Associate Professor Hryn Kateryna Viktorivna • Psychiatry is a medical discipline that deals with the recognition and treatment of mental illness. Psychiatry (translated from Greek - treatment of the soul: psuhe - soul, iatria - treatment) – one of the most important branches of clinical medicine, which studies human-specific diseases that impede adequate adaptation to the environment and are the cause of improper, often dangerous behavior . Psychiatry studies the principles of diagnosis, treatment, as well as the etiology, pathogenesis, prevalence of mental pathology and the system of psychiatric care. SUBJECT AND TASKS • Recognition of mental disorders means not only diagnosis but also study of the etiology, pathogenesis, course and consequences of mental illness. Treatment, in addition to the actual therapy, includes the organization of psychiatric and drug treatment, prevention, rehabilitation and social aspects of psychiatry. • The task of psychiatry - one of the branches of clinical medicine - is to study the origin and nature of mental illness, their clinical manifestations, treatment and prevention. The tasks of psychiatry are: 1) study of the prevalence, conditions and mechanisms of occurrence, nosological structure of -
Screening for Eating Disorders Utilizing the Minnesota Multiphasic Personality Inventory
Andrews University Digital Commons @ Andrews University Dissertations Graduate Research 1999 Screening for Eating Disorders Utilizing the Minnesota Multiphasic Personality Inventory Roseann M. Woodka Andrews University Follow this and additional works at: https://digitalcommons.andrews.edu/dissertations Part of the Nutritional and Metabolic Diseases Commons, and the Other Medical Sciences Commons Recommended Citation Woodka, Roseann M., "Screening for Eating Disorders Utilizing the Minnesota Multiphasic Personality Inventory" (1999). Dissertations. 1559. https://digitalcommons.andrews.edu/dissertations/1559 This Dissertation is brought to you for free and open access by the Graduate Research at Digital Commons @ Andrews University. It has been accepted for inclusion in Dissertations by an authorized administrator of Digital Commons @ Andrews University. For more information, please contact [email protected]. Thank you for your interest in the Andrews University Digital Library of Dissertations and Theses. Please honor the copyright of this document by not duplicating or distributing additional copies in any form without the author’s express written permission. Thanks for your cooperation. INFORMATION TO USERS This manuscript has been reproduced from the microfilm master. UMI films the text directly from the original or copy submitted. Thus, some thesis and dissertation copies are in typewriter face, while others may be from any type of computer printer. The quality of this reproduction is dependent upon the quality of the copy submitted. Broken or indistinct print, colored or poor quality illustrations and photographs, print bleedthrough, substandard margins, and improper alignment can adversely affect reproduction. In the unlikely event that the author did not send UMI a complete manuscript and there are missing pages, these will be noted. -

Social Systems Intervention and Crisis Resolution. Part 1: Assessment Christopher Bridgett & Paul Polak
Bridgett & Polak Advances in Psychiatric Treatment (2003), vol. 9, 424–431 Social systems intervention and crisis resolution. Part 1: Assessment Christopher Bridgett & Paul Polak Abstract Home treatment as an alternative to acute adult in-patient care is part of the National Health Service Plan for mental health services in the UK. As a form of crisis intervention, it benefits from an understanding of, and ways of working with, the social systems relevant to the patient in crisis. This article reviews relevant terminology and background theory, and considers the social factors associated with psychiatric admission. This is the first of a two-part article. Part 2 (Bridgett & Polak, interest to generic community mental health teams 2003, this issue) gives an account of social systems interventions and considers also the application of the approach in achieving (Department of Health, 2002b), specialist assertive early discharge from in-patient care. outreach teams (Department of Health, 2001a) and early-intervention teams (Department of Health, 2001c) and to approved social workers performing The National Health Service (NHS) Plan (Depart- assessments under the Mental Health Act 1983 ment of Health, 2000) set out an intention to establish (Dunn, 2001). 335 crisis resolution and home treatment teams in The theoretical background (Caplan, 1964, 1974; England by 2004, with the expectation that bed usage Polak, 1967, 1970) and practical procedures (Fish, in acute adult general psychiatry could be further 1971; Polak, 1971a, 1972) brought together here were reduced (Joy et al, 2001). The initiative also aimed to first explored and established 30 and more years make generally available a more acceptable and ago.