FSNAU Nutrition Update, May-June 2011
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Protection Cluster Update Weekly Report
Protection Cluster Update Funded by: The People of Japan Weeklyhttp://www.shabelle.net/article.php?id=4297 Report 29 th July 2011 European Commission IASC Somalia •Objective Protection Monitoring Network (PMN) Humanitarian Aid This update provides information on the protection environment in Somalia, including apparent violations of Human Rights and International Humanitarian Law as reported in during the last week through the IASC Somalia Protection Cluster monitoring systems. Incidents mentioned in this report are not exhaustive. They are intended to highlight credible reports in order to inform programming and advocacy by the humanitarian community and national authorities. General Overview A combination of famine, drought, lawlessness and conflict during the last two weeks continues to raise the number of multi layered direct and indirect protection related cases in South Central Somalia. The United Nations officially declared famine in parts of Bakool and Lower Shabelle regions, declaring that Somalia is experiencing the worst drought in decades. 1 Currently in some parts of Bakool and Lower Shabelle, acute malnutrition tops 50 percent and death rates exceed six per 10,000 populations per day. 2 In other parts of southern Somalia, the humanitarian crisis is escalating as aid agencies struggle with funding constraints and access to Al Shabaab controlled areas. Although Al Shabaab recently lifted a ban on aid agencies, the group has since retracted the statement and has continued to restrict humanitarian aid access in many areas under their control. 3 Hence many aid agencies have reported that they are still unable to reach an estimated 2.2 million Somalis facing starvation in many Al Shabaab controlled areas. -

Somalia Type of Report: Semi-Annual, Annual Or Final: Semi- Annual Year of Report: 15 June 2020
PBF PROJECT PROGRESS REPORT COUNTRY: SOMALIA TYPE OF REPORT: SEMI-ANNUAL, ANNUAL OR FINAL: SEMI- ANNUAL YEAR OF REPORT: 15 JUNE 2020 Project Title: Supporting Reconciliation and State-Building Processes Project Number from MPTF-O Gateway: 00114146 If funding is disbursed into a national Type and name of reciPient organizations: or regional trust fund: Country Trust Fund UNDP (Convening Agency) Regional Trust Fund UNSOM Name of ReciPient Fund: ResPonsible Parties Implementing the Project include; (1) Ministry of Interior, Federal Affairs and Reconciliation of Federal Government of Somalia (MoIFAR-FGS) (2) Ministry of Constitution and Federal Affairs- Jubaland State of Somalia (MoCFA-JSS) (3) Ministry of Reconciliation and Federal Affairs - Galmudug State of Somalia (MoRFA-GSS) (4) Office of the President, Southwest State (OOP- SWS) (5) Office of the President, Hirshabelle State (OOP- HSS) (6) The Ministry of Interior, Federalism and Democratization, Puntland State (MoIFAD-PLS) Date of first transfer: 31st December 2018 Project end date: 31st August 2020 Is the current project end date within 6 months? Yes Check if the Project falls under one or more PBF priority windows: Gender promotion initiative Youth promotion initiative Transition from UN or regional peacekeeping or special political missions Cross-border or regional project Total PBF apProved project budget (by reciPient organization): ReciPient Organization Amount UNDP: $ USD 2,598,173 $ $ $ Total: $ USD 2,598,173 Approximate implementation rate as percentage of total project budget: -

EHA Weekly14-20 May 2011
WHO Somalia P.O. Box: 63565 - Nairobi, Kenya - [email protected] - T: +254 20 7623197/8/9 and +254 20 7622840 Emergency Humanitarian Action Weekly Highlights 14 – 20 May 2011 BULLETIN HIGHLIGHTS • From 1-15 May 2011, 933 weapon related- injuries were reported by three major hospi- tals in Mogadishu, 398 cases or 43% were children under the age of five. During April 2011, only 3.5% were children younger than five among the reported casualties. • From 14-15 May 2011, WHO in collaboration with Puntland and Galmudug ministries of health trained more than 40 health workers on AWD/cholera prevention, case detection and management. The health workers are from 9 districts of Galgaduud and Mudug and are now fully skilled to assist an estimated population of 780 000 people1. Update on major public health concerns: • Trends of acute watery diarrhoea (AWD)/cholera The cholera transmission season is ongoing. Some areas in most regions of Somalia have received sporadic rainfall. Due to water shortages, WHO observes that there is a likelihood of a risk in transmis- sion of waterborne diseases as communities tend to utilize water from contaminated sources. Investigation of a number of rumors have confirmed the existence of AWD cases though not severe. Since week 12, and following a confirmed cholera outbreak in Mogadishu, 2268 AWD/cholera cases including 1782 (79%) cases under the age of five with 77 related deaths have been reported from Banadir Hospital in Mogadishu (see graph 1). Children under the age of Graph 2. Low er Shabelle region w eekly AWD two bear the greatest burden of AWD accounting for Cases cases 59% of all reported cases. -

Somalia Energy Sector Needs Assessment and Investment Programme November 2015 Somalia - Energy Sector Needs Assessment and Investment Programme
Somalia Energy Sector Needs Assessment and Investment Programme November 2015 Somalia - Energy Sector Needs Assessment and Investment Programme Copyright © 2015 African Development Bank Group Immeuble du Centre de commerce International d’Abidjan CCIA Avenue Jean-Paul II 01 BP 1387 Abidjan 01, Côte d'Ivoire Phone (Standard): +225 20 26 10 20 Internet: www.afdb.org Rights and Permissions All rights reserved. The text and data in this publication may be reproduced as long as the source is cited. Reproduction for commercial purposes is forbidden. Legal Disclaimer The findings, interpretations and conclusions expressed in this report are those of the author/s and are not necessarily those of the African Development Bank. In the preparation of this document, every effort has been made to offer the most current, correct and clearly expressed information possible. Nonetheless, inadvertent errors can occur, and appli - cable laws, rules and regulations may change. The African Development Bank makes its documentation available wi - thout warranty of any kind and accepts no responsibility for its accuracy or for any consequences of its use. Cover design: AfDB Cover photos: Image © AU-UN IST PHOTO/Ilyas A. Abukar; Image © NIGEL CARR ii Somalia - Energy Sector Needs Assessment and Investment Programme Table of contents Foreword v Ackonwledgements vii Abbreviations and acronyms ix Executive summary xi 1. Introduction and background 1 1.1. Introduction 1 1.2. Objectives/scope 3 1.3. Brief description of the current energy sector 3 1.4. Sector organisation and policies 4 1.5. Reliance on the private sector 5 1.6. Four main issues facing Somalia’s energy sector 6 2. -
Somalia Agric Report DRAFT.Indd
Photo credits: Cover & Inside ©FAO Somalia SOMALIA: Rebuilding Resilient and Sustainable Agriculture Copyright © 2018 by International Bank for Reconstruction and Development/The World Bank and the Food and Agriculture Organization of the United Nations ISBN 978-92-5-130419-8 (FAO) Disclaimer: The designations employed and the presentation of material in this information product do not imply the expression of any opinion whatsoever on the part of the Food and Agriculture Organization of the United Nations (FAO) concerning the legal or development status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. The mention of specific companies or products of manufacturers, whether or not these have been patented, does not imply that these have been endorsed or recommended by FAO in preference to others of a similar nature that are not mentioned. The views expressed in this information product are those of the author(s) and do not necessarily reflect the views or policies of FAO. The findings, interpretations, and conclusions expressed in this work do not necessarily reflect the views of The World Bank, its Board of Executive Directors, or the governments and members represented by either institution. The World Bank does not guarantee the accuracy of the data included in this work. The boundaries, colors, denominations, and other information shown on any map in this work do not imply any judgment on the part of The World Bank concerning the legal status of any territory or the endorsement or acceptance of such boundaries. FAO and The World Bank encourage the use, reproduction and dissemination of material in this information product. -

Week-25 Ending 24 June 2018 Part -I Highlights Highlights
Somalia Weekly Update Week-25 Ending 24 June 2018 Part -I Highlights Highlights • VDPV type 2 and type 3 were detected from 2 AFP cases, 3 Contacts and 3 Community samples collected from Bulloburti, Warshakeh and Jemmame West districts of Central and South Somalia. • EPID no: SOM/HRN/BBT/18/002 and the 3 contacts have cVDPV3 The index: • Location of case: JAMECO MUBARAK village –BULO BURTI District-Hiran Region- Central zone • Date Stool collection 1st and 2nd: 13th and 14th May 2018 • Accessibility of the area: The village is inaccessible since 2015 and no SIA activity • Age and OPV dose status [if case]:72 months female, 0 Dose of • Sequencing results: PV-2 VDPV with 43nt difference and 17 nt difference from Sabin • Closest match: genetically linked to the VDPV3 sequence for ES/SOM/BAN/HMW/KAWMA-1/18/006 (Kawma ENV site, emergence group SOM-BAN- Warshaikh 2) • EPID no: SOM/MSH/WRS/18/003 and the contact SOM-MSH-WRS-18-001-C3 The index: • Location of case: Bohi village –Warsheikh District-Middle Shaballe-- Central zone • Date Stool collection 1st and 2nd: 30st and 31th May 2018 • Accessibility of the area: The village is accessible • Age and OPV dose status [if case]:39 months female, 0 Dose of • Sequencing results: PV-3 VDPV with 19nt difference from Sabin • Closest match: The PV3 VDPV is genetically linked to the VDPV3 sequence for ES/SOM/BAN/HMW/KAWMA-1/18/006 (Kawma ENV site, emergence group SOM- BAN-2). The new PV3 viruses are classified immediately are cVDPV3 • EPID no: SOM/LJB/JMW/18/CC1/001 and SOM/LJB/JMW/18/CC1/003 (Community -

Pdf | 303.36 Kb
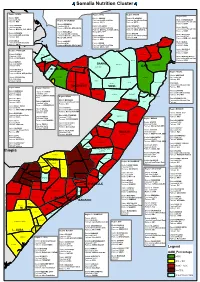
Somalia Nutrition Cluster Region: ADWAL Regiion:: SOOL Region: SANAG Region:BARI District: BAKI Diissttrriicctt:: AIINABO District: EL AFWEIN Caseload 1,018 Region: W. GALBEED Casselload IInsuffffiiciientt Datta Caseload Insufficient Data District: ISKUSHUBAN Partners: WVI Parrttnerrss:: SRCS Partners: SRCS Caseload Insufficient Data District: BERBERA Partners: HADO District BOROMA Caseload 1,616 Diissttrriicctt LAS ANOD District ERIGAVO District GARDO Caseload 7,129 Partners: MOH SL ,HPA, SRCS Casselload IInsuffffiiciientt Datta Caseload Insufficient Data Caseload Insufficient Data Partners: MOH SL, SCI, SRCS Parrttnerrss:: MOH SL,, SCODO,,SRCS,, Partners: SRCS, MOH SL Partners: HADO District HARGEISA Merrcy USA,, APD District LUGHAYA District BADAN Caseload 1,192 District BOSSASO Caseload Insufficient Data Partners: MOH SL , WVI, HPA, Diissttrriicctt TALEH Caseload Insufficient Data Partners: WVI i Caseload 3,119 t Mercy USA, SRCS Casselload IInsuffffiiciientt Datta Partners: APD Partners: BHM , SCI, HADO u Parrttnerrss:: APD District ZEILA o District GABILEY District ALULA Caseload Insufficient Data ALULA b Caseload 169 Diissttrriicctt HUDUN Caseload 662 Partners: SRCS ji ZEILA Partners: MOH SL, SRCS, WVI Casselload IInsuffffiiciientt Datta Partners: HADO D Parrttnerrss:: SRCS,, APD ^` District QANDALA Region: TOGDHEER Caseload 747 QANDALA Partners: HADO District: SHEIKH ZEILA BOSSASO Caseload 904 EL AFWEIN District BENDER BAYLA Partners: SRCS,HPA LUGHAYA Caseload Insufficient Data BAKI ^` BADAN Partners: HADO District BURAO AWDAL -

Epidemiological Week 28 (Week Ending 15Th July, 2018)
Epidemiological Week 28 (Week ending 15th July, 2018) Highlights Cumulative figures as of week 28 • 232 health facilities across Somalia submitted weekly • 1,576,745 consultations from week 1 reports of epidemic-prone diseases in the electronic to week 28. early warning disease surveillance (EWARN) system in • 5,880 cumulative cases of week 28. • Total number of consultations increased from 51,625 AWD/Cholera and 40 deaths since in week 27 to 54,605 in week 28. December 2017. • A total of 307 alerts were received. 35 of these alerts • 8,880 Accumulative alerts were were confirmed as true alerts in week 28. received, 499 of these, were • The highest numbers of diseases reported in week 28 confirmed as true alerts from week 1 were other acute diarrhoeas (2,306 cases), influenza to week 28, 2018. like illness (1,245 cases) and severe acute respiratory illness (1,559 cases). • 6,201 cumulative cases of suspected measles cases since the beginning of • A total of 146 new cases of suspected AWD/cholera with no death were reported in week 28 compared to 2018. Of the 6,201 measles cases, 151 AWD cases with no death in week 27. 4,112 (66%) are under 5 years while • A cumulative total of 5,880 AWD/cholera cases1, 2,089 (34%) are above 5 years. including 40 deaths have been reported since • 7,624 cumulative cases of Malaria December 2017. were reported since the beginning of • The number of reported measles cases decreased 2018, 3,302(43%) are under 5 years, from 61 in week 27 to 52 cases in week 28. -
Agulhas and Somali Currents Large Marine Ecosystems Project
Agulhas and Somali Currents Large Marine Ecosystems Project Capacity Building and Training Component National Training Plan for SOMALIA Prepared by: Mr. Hassan Mohamud Nur 1) Summary of key training requirements a) Skill training for fishers. b) To strength the scientific and management expertise c) To introduce an ecosystem approach to managing the living marine resources d) To enhance the local and international markets. e) To secure processing systems f) To upgrade environmental awareness and waste management and marine pollution control g) To create linkages between the local community and the international agencies 2) introduction: Somalia has 3,333Km of coast line of which 2,000Km is in the Indian Ocean south of Cape Guardafui and 1,333Km of north shore of Gulf of Aden. Surveys indicate high potential for fisheries development with evenly distributed fish stocks along the entire coastline, but with greater concentration in the Northeast. The fishing seasons are governed by two monsoon winds, the south west monsoon during June to September and northeast monsoon during December to March and two inter-monsoon periods during April/May and October/November. In the case of Somalia, for the last two decades the number of people engaged in fisheries has increased from both the public and private sector. Although, the marine fisheries potential is one of the main natural resources available to the Somali people, there is a great need to revive the fisheries sector and rebuild the public and private sector in order to promote the livelihood of the Somali fishermen and their families. 3) Inventory of current educational Capacity Somalia has an increasing number of elementary and intermediate schools, beside a number of secondary and a handful of universities. -

Warsheikh Situational Report (Rapid Assessment for Solar Poweredwell in Warsheikh District)
WARSHEIKH SITUATIONAL REPORT (RAPID ASSESSMENT FOR SOLAR POWEREDWELL IN WARSHEIKH DISTRICT) Assessment Team: 1. Mubashir Mohamed Ahmed ADT 2. Mohamud Jinow Afrah Water Engineer 3. Abdullahi Salad Qoslaaye Construction and Solar System Expert 28/06/2021 Brief Background Warsheikh district compose of 52 villages. Warsheikh town is the seat of district which belongs to middle Shabelle region of Hirshabelle state. The town is on the Indian ocean 40km north of Mogadishu. It is well known Islamic historical center and hosts centers of Sufi Dariqas. The twon is very known the traditional Islamic studies such Fiqihi, Arabic Grammer and Tafseer. It was one of the principal settlements of the Sultanate of Mogadishu during the Middle Ages. The town has an old mosque situated near a cape, which features an inscription noting its construction in 1278H (1861-1862 CE). Politically, it was center for the resistance of Italian colony. Warsheikh was before the civil war a popular destination for Sufi adherents who visited tombs of Sufi clerics and saints buried in the town. It was popular for beach lovers away from the mostly crowded Mogadishu beaches, recently the town away from Mogadishu only 40 km has been a boom of visitors. The population of Warsheikh is estimated 3200 HHs or 19200 people. Warsheikh district like other districts doesn’t have segregated data but they claim the population in the town is more than 3200HHs. According to the Warsheikh mayor about 8634 children under 18 years, 5778 women and 4788 men are living in Warsheikh town. The livelihood in the town is variety of small businesses, fishing, farming and animal herding. -
Pdf | 433.9 Kb
Somalia Nutrition Cluster Region: ADWAL Region: SOOL Region: SANAG Region:BARI District: BAKI District: AINABO District: EL AFWEIN Caseload 5,214 Region: W. GALBEED Caseload Insufficient Data Caseload Insufficient Data District: ISKUSHUBAN Partners: WVI Partners: SRCS Partners: SRCS Caseload Insufficient Data District: BERBERA Partners: HADO District BOROMA Caseload 8,274 District LAS ANOD District ERIGAVO District GARDO Caseload 36,498 Partners: MOH SL ,HPA, SRCS Caseload Insufficient Data Caseload Insufficient Data Caseload Insufficient Data Partners: MOH SL, SCI, SRCS Partners: MOH SL, SCODO,SRCS, Partners: SRCS, MOH SL Partners: HADO District HARGEISA Mercy USA, APD District LUGHAYA District BADAN Caseload Insufficient Data District BOSSASO Caseload Insufficient Data Partners: MOH SL , WVI, HPA, District TALEH Caseload Insufficient Data Partners: WVI i Caseload 26,791 t Mercy USA, SRCS Caseload Insufficient Data Partners: APD Partners: BHM , SCI, HADO u Partners: APD District ZEILA o District GABILEY District ALULA Caseload Insufficient Data ALULA b Caseload 4,741 District HUDUN Caseload 5,686 Partners: SRCS ji ZEILA Partners: MOH SL, SRCS, WVI Caseload Insufficient Data Partners: HADO D Partners: SRCS, APD ^` District QANDALA Region: TOGDHEER Caseload 6,417 QANDALA Partners: HADO District: SHEIKH ZEILA BOSSASO Caseload 4,630 EL AFWEIN District BENDER BAYLA Partners: SRCS,HPA LUGHAYA Caseload Insufficient Data BAKI ^` BADAN Partners: HADO District BURAO AWDAL BERBERA Caseload 44,341 BAKI SANAG ERIGAVO ISKUSHUBAN Partners: HPA BORAMA -

Somalia Weekly Update Week-26 Ending 01 July 2018 Highlight: TROCAN
Somalia Weekly Update Week-26 Ending 01 July 2018 Highlight: TROCAN • A new VDPV2 isolated from a contact (EPID SOM/GDO/DLO/18/002-C1) from Dolo district in Gedo region of South zone. It has 38 nucleotide differences from Sabin2. The VP1 sequence shows it has no close genetic link to previously sequenced cVDPV2s; it is classified as VDPV2 and represents a VDPV2 event that has not previously been identified. Dolo • The contact sample is collected from an IDP camp called KABASA • Dolo is one of the 5 fully accessible districts in south from the total 29 districts in south zone. The districts borders both Ethiopia and Kenya characterized by high population moment in all directions and is around 40 km from Mandara town in Kenya. There is immunization activity in the district and the index case took 6 doses of OPV including 2 doses from routine EPI. The last SIA was conducted in May, 2018 during NID-1. - No reporting of a new positive environmental sample for cVDPV2 or cVDPV3 last week; the date of collection of most recent positive environmental sample for cVDPV2 or cVDPV3 was on 17th May 2018 from Waberi and Hamerewoini districts in Banadir. A cVDPV3 and one co-infected (cVDPV2 & cVDPV3) cases reported from Bulloburti and Warhsakeh districts of Hiran and Middle Shabelle regions in Central zone - An index case with co-infection of cVDPV2 and cVDPV3 from Bulloburti district in Hiran region had date of onset on 11 May. In addition, cVDPV3 was isolated from three contacts of this case. - cVDPV3 case isolated from an AFP with dates of onset on 23 May is from Warsheikh district of Middle Shabelle region.