Ultra-Processed Foods, Diet Quality and Human Health
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Find Moths with Moth Traps
3.5 Sugaring Moth traps will attract the greatest variety of moths, but not all moths are equally attracted to light. Some can be observed using sugary bait instead. Moths come to “sugar” because they feed on nectar, sap and honeydew, all of which are unrefined sources of sugar (however, some moths do not feed as adults, and therefore will never be seen at sugar sources). The success of the technique is variable - warm humid nights with a light wind are best for sugaring (as they are for most forms of mothing), but the technique will also work on far from ideal nights, and not work on nights that seem good for no apparent reason. Ingredients 454g Tin of Black Treacle 1Kg Brown Sugar (the darker the better) 500ml Brown Ale or Bitter (fizzy drink like cola will do as an alternative) Paint brush. Slowly heat the ale (or cola) in a large pan and simmer for five minutes. Stir in and dissolve the sugar, followed by the treacle and then simmer for two more minutes. Allow to cool before decanting into a container. A drop of rum stirred in just before use is recommended but not essential. Paint the mixture about eye level onto 10- 20 tree trunks or fence posts just before dusk and check for moths by torch-light for the first two hours of darkness. A variation of this technique is “ wine roping ”. This works on a similar principle to the above. Ingredients Bottle of cheap red wine 1kg sugar 1m lengths of thick cord or light rope made from absorbent material. -
Access Pdf of Geoffrey Cannon's Column Here
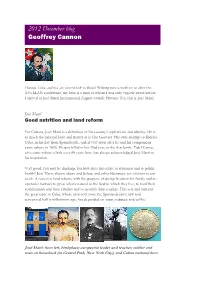
2012 December blog Geoffrey Cannon Havana, Cuba, and now just arrived back in Brazil. Writing now a week or so after the XVI SLAN conference, my hero is a man of whom I was only vaguely aware before I arrived at José Martí International Airport outside Havana. Yes, this is José Martí. José Martí Good nutrition and land reform For Cubans, José Martí is a definition of his country’s aspirations and identity. He is as much the national hero and martyr as is Che Guevara. His own attempt to liberate Cuba, in his day from Spanish rule, ended very soon after he and his companions came ashore in 1895. He was killed in his 43rd year, in the first battle. Fidel Castro, who came ashore a little over 60 years later, has always acknowledged José Martí as his inspiration. Very good, you may be thinking, but how does this relate to nutrition and to public health? José Marti, shown above and below, and other liberators, are relevant to our work. A reason is land reform, with the purpose of giving freedom for family and co- operative farmers to grow what’s natural in the land in which they live, to feed their communities and their families and to nourish their country. This was and remains the great issue in Cuba, whose economy since the Spaniards came saw and conquered half a millennium ago, has depended on sugar, tobacco and coffee. José Martí: from left, birthplace; campesino leader and teacher; soldier and man on horseback (in Central Park, New York City); and Cuban national hero The first three pictures show José Martí’s birthplace, and then him as a campesino and an educator committed to land reform. -

Minimum Dietary Diversity for Women a Guide to Measurement
FANTA III FOOD AND NUTRITION TECHNICAL A SSISTANCE Minimum Dietary Diversity for Women A Guide to Measurement Minimum Dietary Diversity for Women A Guide to Measurement Published by the Food and Agriculture Organization of the United Nations and USAID’s Food and Nutrition Technical Assistance III Project (FANTA), managed by FHI 360 Rome, 2016 Recommended citation: FAO and FHI 360. 2016. Minimum Dietary Diversity for Women: A Guide for Measurement. Rome: FAO. The designations employed and the presentation of material in this information product do not imply the expression of any opinion whatsoever on the part of the Food and Agriculture Organization of the United Nations (FAO), or of FANTA/FHI 360 concerning the legal or development status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. The mention of specific companies or products of manufacturers, whether or not these have been patented, does not imply that these have been endorsed or recommended by FAO, or FHI 360 in preference to others of a similar nature that are not mentioned. Additional funding for this publication was made possible by the generous support of the American people through the support of the Office of Health, Infectious Diseases, and Nutrition, Bureau for Global Health, U.S. Agency for International Development (USAID), under terms of Cooperative Agreement AID-OAA-A-12-00005 through the Food and Nutrition Technical Assistance III Project (FANTA), managed by FHI 360. The views expressed in this information product are those of the author(s) and do not necessarily reflect the views or policies of FAO, FHI 360, UC Davis, USAID or the U.S. -

Eat Less Meat’ Campaign
Compassion in World Farming Trust THE GLOBAL BENEFITS OF EATING LESS MEAT A report by Compassion in World Farming Trust 2004 THE GLOBAL BENEFITS OF EATING LESS MEAT Compassion in World Farming Trust is an educational charity working internationally to advance the welfare of farm animals. We carry out detailed research using academic literature and publish educational resources for use by schools, universities and the general public on farm animal welfare and associated environmental, social and ethical issues. Our publications include reports, books, videos, factsheets and teaching materials. CIWF Trust cooperates with organisations and individuals in many countries. Our current key issues include animal sentience and an assessment of the impact of the World Trade Organisation on farm animal welfare globally. The Trustees are grateful to several grant-making Charitable Trusts and members of the public who have made work in these areas possible. A complete list of our available materials and downloadable versions can be found at www.ciwf.org. THE GLOBAL BENEFITS OF EATING LESS MEAT THE GLOBAL BENEFITS OF EATING LESS MEAT A REPORT FOR COMPASSION IN WORLD FARMING TRUST Report compiled and written by Mark Gold Foreword by Jonathon Porritt 2004 © Compassion in World Farming Trust, 2004 ISBN 1 900156 29 6 Compassion in World Farming Trust, 5a Charles Street, Petersfield, Hampshire, GU32 3EH, UK T. +44 (0)1730 268070 F. +44 (0)1730 260791 E. [email protected] W. www.ciwf.org Compassion in World Farming Trust is an educational charity dedicated to advancing farm animal welfare. Registered Charity number, 1095050, a company limited by guarantee, Registered Number 4590804. -

Cabot Creamery Cooperative Receives U.S. Dairy Sustainability
June 24, 2016 • Vol. 80, Num ber 6 Published monthly by the Vermont Agency of Agriculture • www.vermontagriculture.com Cabot Creamery Cooperative Receives U.S. Dairy Sustainability Award for Real Farm Power™ Program Effort to Reduce Food Waste and Energy Use Has Cows Providing Cream and Electricity for Cabot Butter By Laura Hardie, New England Dairy U .S . Dairy®, established under Promotion Board the leadership of dairy farmers, announced its fifth annual U .S . abot Creamery Cooperative Dairy Sustainability Awards during has been recognized with a a ceremony May 11 in Chicago . C2016 U .S . Dairy Sustainability The program recognizes dairy farms, Award for Outstanding Dairy businesses and partnerships whose Processing & Manufacturing sustainable practices positively Sustainability . The cooperative impact the health and well-being of was selected for its Real Farm consumers, communities, animals Power™ program which is the and the environment . latest in a series of sustainability Real Farm Power™ reduces projects pioneered by the 1,200 greenhouse gas emissions by 5,680 dairy-farm families of Agri-Mark tons annually while generating 2,200 dairy cooperative, owner of Cabot megawatt hours (MWh) of clean, Members of Cabot Creamery Cooperative accept the 2016 U.S. Dairy Creamery Cooperative . The program renewable energy per year to offset Sustainability Award for Outstanding Dairy Processing & Manufacturing takes a closed-loop approach, the power needed to make Cabot™ Sustainability in Chicago, Illinois on May 11, 2016. From Left to right: Amanda recycling cow manure, food scraps butter . The $2 .8 million project is Freund of Freund’s Farm Market and Bakery, Ann Hoogenboom of Cabot and food processing by-products expected to have a six-year payback, Creamery Cooperative, Steven Barstow II of Barstow’s Longview Farm, Phil to produce renewable energy on a and it offers a blueprint for scaling Lempert journalist and the Supermarket Guru, Caroline Barstow of Barstow’s Massachusetts dairy farm . -

Tribute to Three Giants Figures of the Sixties' Pop
TRIBUTE TO THREE GIANTS FIGURES OF THE SIXTIES’ POP MUSIC IN THE 50th ANNIVERSAIRE OF THEIR DEATH. ALAN WILSON, JIMI HENDRIX AND JANIS JOPLIN: ASTROLOGICAL REVIEW OF THREE 27’ CLUB MEMBERS. We were at the end of the “sixties”, a remarkable decade of 20th century for popular music, revolutionary movements, technological achievements and radical changes in human relationships. It was also the time of “hippie liberation”, the spread of drugs through young people. Everything was fine when, just in the span of thirty days, three outstanding members of musical background suddenly died. 1970, September the 3th: Alan Wilson, “Canned Heat” guitar, harmonica and vocal, commit suicide at home of another member group, Bob Hite, in Topanga Canyon, California. An overdose was the cause of his death. He was 27 years old. 1970, September the 18th: Jimi Hendrix, one of the bests guitarrist of all times, share his last night with Monica Dannemann in Samarkand Hotel, London. When she woke up Jimi was inconscious, yet breathe. He was moved at St. Mary Abbot Hospital, but he was not alive. The cause of his death: asphyxia per vomit. His partner declared that Jimi had had seven tablets of Vesparax, a barbituric, say, 18 times the recommended dose. He was 27 years old. 1970, October the 4th: Janis Joplin, a singer and contraculture icon of the sixties was found dead in her hotel room, at Los Angeles, just when she was going to record the vocal part of Buried Alive in the Blues next morning. A portent, maybe a synchronicity. The official cause of her death was an heroine overdose, probably combined with alcohol effects. -

Subethnic Variation in the Diets of Moslem, Sikh and Hindu Pregnant Women at Sorrento Maternity Hospital, Birmingham
Downloaded from https://doi.org/10.1079/BJN19840114 British Journal of Nutrition (1984), 52, 469-476 469 https://www.cambridge.org/core Subethnic variation in the diets of Moslem, Sikh and Hindu pregnant women at Sorrento Maternity Hospital, Birmingham BY P. A. WHARTON, P. M. EATON* AND B. A. WHARTONT Sorrento Maternity Hospital, Birmingham B13 9HE . IP address: (Received 25 January 1984 - Accepted 1 June 1984) 1. The previous paper (Eaton et al. 1984) described the nutrient intake of pregnant Asian women attending 170.106.202.226 Sorrento Maternity Hospital, Birmingham using the weighed and recall methods. The present paper describes the subethnic variation in nutrient intake by comparing the results from Pakistanis, Sikhs, Hindus and Bangladeshis and also describes food eaten by the pregnant women. 2. Generally. Sikhs had the highest intake of most nutrients (mean energy 7.5 MJ (1800 kcal)/d) and the greatest variety of foods; they ate chapatti and paratha but few ate meat. Hindus had a very similar diet but more ate , on meat, chicken and rice. Pakistanis had an energy intake about 10% below that of the Sikhs and Hindus; meat was eaten, and intake of fruit, and therefore vitamin C, was quite large. Bangladeshis were the smallest women; 29 Sep 2021 at 14:11:24 they had the lowest intake of energy (mean energy 6.5 MJ (1555 kcal)/d) and most nutrients, except for protein, so that 15% of energy was provided by protein. Fish, rice and a low-fat intake were other features of their diet. 3. From a nutritional standpoint, peoples coming from the Asian subcontinent should be divided into subethnic groups; the collective term ‘Asian’ is insufficient. -

When the Sun Dies, It Will Make
When the Sun dies, it will make: 1. A red giant 2. A planetary nebula 3. A white dwarf 4. A supernova 5. 1, 2, and 3 When the Sun dies, it will make: 1. A red giant 2. A planetary nebula 3. A white dwarf 4. A supernova 5. 1, 2, and 3 A white dwarf star: 1. Is the core of the star from which it formed, and contains most of the mass 2. Is about the size of the earth 3. Is supported by electron degeneracy 4. Is so dense that one teaspoonful would weigh about as much as an elephant 5. All of the above A white dwarf star: 1. Is the core of the star from which it formed, and contains most of the mass 2. Is about the size of the earth 3. Is supported by electron degeneracy 4. Is so dense that one teaspoonful would weigh about as much as an elephant 5. All of the above What keeps a white dwarf from collapsing further? 1. It is solid 2. Electrical forces 3. Chemical forces 4. Nuclear forces 5. Degeneracy pressure What keeps a white dwarf from collapsing further? 1. It is solid 2. Electrical forces 3. Chemical forces 4. Nuclear forces 5. Degeneracy pressure If a white dwarf in a binary has a companion close enough that some material begins to spill onto it, the white dwarf can: 1. Be smothered and cool off 2. Disappear behind the material 3. Have new nuclear reactions and become a nova 4. Become much larger 5. -

Upfield Plant-Based Spreads and Margarine Vs. Dairy Butter
Upfield plant-based spreads and margarine vs. dairy butter Life Cycle Assessment Technical Summary March 2020 Version 1 PLANT-BASED SPREADS AND MARGARINE VS. DAIRY BUTTER. LCA TECHNICAL SUMMARY 1 LIFE CYCLE ASSESMENT …….…….…….…….…….…….…….…….…….…….…….…….…….…….…….…….. 3 METHOD …….…….…….…….…….…….…….…….…….…….…….…….…….…….…….…….…….…….…….…... 3 CRITICAL REVIEW …….…….…….…….…….…….…….…….…….…….…….…….…….…….…….…….…….…….3 FUNCTIONAL UNIT ………….…….…….…….…….…….…….…….…….…….…….…….…….…….…….……….. 3 ENVIRONMENTAL IMPACT INDICATORS CONSIDERED ……….…….…….…….…….…….…….…..….. 3 FROM FARM-TO-PLATE ……..…….…….…….…….…….…….…….…….…….…….…….…….…….…….…….. 4 DATA COLLECTION AND MODELLING………….…….…….…….…….…….…….…….…….…….…….……... 4 RESULTS AND DISCUSSION …….…….…….…….…….…….…….…….…….…….…….…….…….…….……….. 5 CLIMATE CHANGE IMPACTS ………….…….…….…….…….…….…….…….…….…….…….…….…….……... 5 FRESHWATER CONSUMPTION ……….…….…….…….…….…….…….…….…….…….…….…….………..….. 6 LAND OCCUPATION ………….…….…….…….…….…….…….…….…….…….…….…….…….…….…….…….... 6 LCA CONCLUSIONS AND OUTLOOK ………….…….…….…….…….…….…….…….…….…….…….………... 7 CALCULATION OF EQUIVALENCIES ………….…….…….…….…….…….…….…….…….…….…….………... 8 ABOUT QUANTIS ………….…….…….…….…….…….…….…….…….…….…….…….…….…….…….…….…….. 9 REFERENCES ……….…….…….…….…….…….…….…….…….…….…….…….…….…….…….…….…….……….. 9 PLANT-BASED SPREADS AND MARGARINE VS. DAIRY BUTTER. LCA TECHNICAL SUMMARY 2 In 2018 Quantis conducted a Life Cycle Assessment (LCA) of Upfield’s plant-based spreads and margarines in 21 European and North American markets. These products were compared to dairy butter sold in the same -

Performance Nutrition System WARNINGS & DISCLAIMERS
SSP FUEL Performance Nutrition System WARNINGS & DISCLAIMERS This book is intended as a reference only, not as a medical manual. The information provided here is designed to help you make informed decisions about fueling your body for performance during sport, exercise and physical activity. It is not intended as a substitute for any treatment that may have been prescribed by your doctor. You should consult a medical professional before undertaking any fitness regimen, exercise program or diet, including anything contained or set forth in this booklet, either in print, electronic media or on screen (materials). Nutrition information represents the opinions of the respective authors and is protected under the laws of copyright and trademark. SPECTRUM SPORTS PERFORMANCE, INC. AND ITS DIRECTORS, OFFICERS, EMPLOYEES AND AGENTS MAKE NO WARRANTIES OF ANY KIND OF NATURE RELATING TO THE MATERIALS, EITHER EXPRESS OR IMPLIED, AND EXPRESSLY DISCLAIMS ALL SUCH WARRANTIES AND REPRESENTATION, INCLUDING, BUT NOT LIMITED TO, THE WARRANTY OF MERCHANTABILITY AND THE WARRANTY OF FITNESS FOR A PARTICULAR PURPOSE. KNOWLEDGE REGARDING THE HUMAN BODY AND ITS NUTRITIONAL NEEDS CHANGES, THEREFORE, YOU SHOULD PERIODICALLY CHECK THE FOLLOWING WEBSITE FOR UPDATES AND CHANGES TO THESE MATERIALS – SPECTRUMSP.COM. HOWEVER, SPECTRUM SPORTS Notice PERFORMANCE, INC. HAS NO OBLIGATION TO PROVIDE UPDATES AND NEWS. ©2013 By Spectrum Sports Performance, Inc. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, scanning, or any other information storage and retrieval system, without the written permission of Spectrum Sports Performance, Inc. You spend hours training, practicing, preparing and competing.! You are drenched with sweat, pushing yourself to the limit to get a little better each day.! You prepare day in and day out to be at your best on game day.! Don’t leave out one of the most important pieces….FUEL. -

Introduction to Astronomy from Darkness to Blazing Glory
Introduction to Astronomy From Darkness to Blazing Glory Published by JAS Educational Publications Copyright Pending 2010 JAS Educational Publications All rights reserved. Including the right of reproduction in whole or in part in any form. Second Edition Author: Jeffrey Wright Scott Photographs and Diagrams: Credit NASA, Jet Propulsion Laboratory, USGS, NOAA, Aames Research Center JAS Educational Publications 2601 Oakdale Road, H2 P.O. Box 197 Modesto California 95355 1-888-586-6252 Website: http://.Introastro.com Printing by Minuteman Press, Berkley, California ISBN 978-0-9827200-0-4 1 Introduction to Astronomy From Darkness to Blazing Glory The moon Titan is in the forefront with the moon Tethys behind it. These are two of many of Saturn’s moons Credit: Cassini Imaging Team, ISS, JPL, ESA, NASA 2 Introduction to Astronomy Contents in Brief Chapter 1: Astronomy Basics: Pages 1 – 6 Workbook Pages 1 - 2 Chapter 2: Time: Pages 7 - 10 Workbook Pages 3 - 4 Chapter 3: Solar System Overview: Pages 11 - 14 Workbook Pages 5 - 8 Chapter 4: Our Sun: Pages 15 - 20 Workbook Pages 9 - 16 Chapter 5: The Terrestrial Planets: Page 21 - 39 Workbook Pages 17 - 36 Mercury: Pages 22 - 23 Venus: Pages 24 - 25 Earth: Pages 25 - 34 Mars: Pages 34 - 39 Chapter 6: Outer, Dwarf and Exoplanets Pages: 41-54 Workbook Pages 37 - 48 Jupiter: Pages 41 - 42 Saturn: Pages 42 - 44 Uranus: Pages 44 - 45 Neptune: Pages 45 - 46 Dwarf Planets, Plutoids and Exoplanets: Pages 47 -54 3 Chapter 7: The Moons: Pages: 55 - 66 Workbook Pages 49 - 56 Chapter 8: Rocks and Ice: -

Aspartame Studies by Dr. Mercola
Aspartame Studies Health Problem: Brain damage/Cognitive skills disruption/Retardation/Neurochemical changes in the brain/Behavioral and Mood Changes/Problems Reference: http://aspartame.mercola.com/sites/aspartame/studies.aspx 1. Year Published: 1970 Full Reference: Brain Damage in Infant Mice Following Oral Intake of Glutamate, Aspartate, or Cysteine; Nature 1970;227-609-610 Funded By: Washington University Conclusion/Findings: Irreversible degenerative changes and acute neuronal necrosis Hyperlink to Study http://www.nature.com/nature/journal/v227/n5258/pdf/227609b0.pdf 2. Year Published: 2008 Full Reference: Direct and Indirect Cellular Effects of Aspartame on the Brain. European Journal of Clinical Nutrition (2008) 62, 451-462; P. Humphries, E. Pretorius, and H. Naude Funded By: Not known Conclusion/Findings: Excessive aspartame ingestion might cause certain mental disorders, as well as compromised learning and emotional functioning Hyperlink to Study: http://www.newmediaexplorer.org/sepp/aspartamebrain.pdf 3. Year Published: 2007 Full Reference: Life-Span Exposure to Low Doses of Aspartame Beginning During Prenatal Life Increases Cancer Effects in Rats, Morando Soffritti, Fiorella Belpoggi, Eva Tibaldi, Davide Degli Esposti, Michelina Lauriola; Environmental Health Perspectives, 115(9) Sep 2007; 115:1293-1297. doi:10.1289/ehp.10271. Funded By: Not known Conclusion/Findings: Carcinogenicity proven a second time; with effects increased when exposure to aspartame begins during fetal life. Hyperlink to Study: http://ehp03.niehs.nih.gov/article/fetchArticle.action?articleURI=info:doi/10.1289/ehp.10271 4. Year Published: 1984 Full Reference: Effects of Aspartame and Glucose on Rat Brain Amino Acids and Serotonin. Yokogoshi H, Roberst CH, Caballero B, Wurtman RJ. American Journal of clinical Nutrition.