Building the Perfect Beast Featuring 'Frank N
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MUSCLED BOSS Muscle Infusion, 1-2 Servings Cream of Rice Adding 75Lbs of Solid Muscle Is No Mean Feat
Real-life inspiration Transform INSPIRATION MOTIVATION ASPIRATION PERSPIRATION GEEK GEEK TO TO FREAK HOW RYAN DID IT FREAK RYAN ROGERSON DIET PLAN Diet plan that guided my transformation: GAINED My diet is very simple, but it works great. I always eat four to five solid meals per day, and also have one or two protein shakes (de- FROM MUSCLE pending on my goal at the time). This is a basic outline for cutting body fat. When I’m looking to bulk up I add more carbohydrates into the later meals. MEAL ONE 16oz liquid egg whites (equal to about 10 egg MOTOCROSS TO 210lb whites), 99g blueberries, 80g oatmeal MEAL TWO 6-8oz chicken, 85g broccoli, 8oz sweet potato MEAL THREE (Post workout meal) 2 Scoops Nutrex Research MUSCLED BOSS Muscle Infusion, 1-2 servings cream of rice Adding 75lbs of solid muscle is no mean feat. Dedicated MEAL FOUR 6-8oz chicken, 85g broccoli, 1 serving walnuts MEAL FIVE 6-8oz lean ground beef Ryan made it happen to go from skinny to shredded INSPIRED before he inspired others to do it too! vBY MUSIC Tunes that kept me going TRAINING REGIME HY I DECIDED TO HOW I ACCOMPLISHED MY GOALS I’m always changing up my training, but this is my TRANSFORM I’m the type of person that if I commit favorite workout routine. I like using a push/pull/legs to something it’s 100% or don’t do LOST I used to be a 135lb format going two days on and one day off. I stick to the professional it at all. -

Water Polo Cycle 4 Week 12 August 3Rd Day 1 Day 2 Day 3 Plate Warm
Water Polo Cycle 4 Week 12 August 3rd Day 1 Day 2 Day 3 Plate Warm Up x 5 Plate Warm Up x 5 Plate Warm Up x 5 Plate Squats, Standing Rotation, Wood Chops, Lateral Lunge Plate Squats, Standing Rotation, Wood Chops, Lateral Lunge Plate Squats, Standing Rotation, Wood Chops, Lateral Lunge Hurdle Warm Up x 3 each side Hurdle Warm Up x 3 each side Hurdle Warm Up x 3 each side Over/Under/Over Over/Under/Over Over/Under/Over Shoulder Warm Up 1 x 10 each way Shoulder Warm Up 1 x 10 each way Shoulder Warm Up 1 x 10 each way Standing 90/90, Standing Rear Delt Pull, External Rotation, Standing 90/90, Standing Rear Delt Pull, External Rotation, Standing 90/90, Standing Rear Delt Pull, External Rotation, Internal Rotation, 45 degree delt raise Internal Rotation, 45 degree delt raise Internal Rotation, 45 degree delt raise Band Abduction x 5 Band Abduction x 5 Band Abduction x 5 Half Moon, Monster Walk, Step Outs, Elvis, Fire Hydrant, Clam Shell Half Moon, Monster Walk, Step Outs, Elvis, Fire Hydrant, Clam Shell Half Moon, Monster Walk, Step Outs, Elvis, Fire Hydrant, Clam Shell REST REST REST Clean First Pull (Power Position) 4 x 3 90 sec. DB Push Press 3 x 3 e.a. 60 sec. Clean First Pull (Power Position) 4 x 3 90 sec. ss Bridges 3 x 10 ss S.L. Bridges 3 x 10 ss Bridges 3 x 10 ss Ankle Band Series 1 x 15 ss Ankle Band Series 1 x 15 Back Squat 70% x 4 90 sec. -
Man-Of-Iron-Workouts-Week-10.Pdf
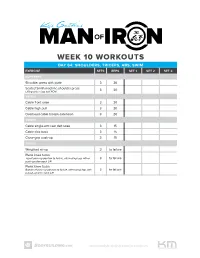
WEEK 10 WORKOUTS DAY 64: SHOULDERS, TRICEPS, ABS, SWIM EXERCISE SETS REPS SET 1 SET 2 SET 3 SUPERSET Shoulder press with plate 3 20 Seated Smith machine shoulder press 3 20 Lifting only in top-half ROM TRISET Cable front raise 3 20 Cable high pull 3 20 Overhead cable triceps extension 3 20 TRISET Cable single-arm rear delt raise 3 15 Cable kick-back 3 15 Close-grip push-up 3 15 TRISET Weighted sit-up 3 to failure Plank knee tucks Top of push-up position to failure, alternating legs with a 3 to failure push-up after each L/R Plank knee tucks Bottom of push-up position to failure, alternating legs with 3 to failure a push-up after each L/R www.bodybuilding.com/manofiron WEEK 10 WORKOUTS DAY 64: SHOULDERS, TRICEPS, ABS, SWIM (CONTINUED) SWIMMING WARM-UP 4 sets of 100 meters, 6/10 effort, rest 20 sec. between sets. Count your strokes per 25 meters; you’ll need that info later in the workout 10 Rounds: Rest as much as needed 25 meters scull drill 25 meters front catch drill 25 meters Superman drill 25 meters freestyle MAIN SET 4 rounds, rest 20 sec. after each round 150 meters, stroke count reduced by at least 1 per 25 meters to focus on strength 150 meters, strong, fast swim, normal stroke count and rhythm 100 meters kick with board, 7.5/10 effort, 25 sec. rest 3 sets of 50 meters with kickboard, escalating in intensity from 7/10 to 9.5/10, rest 25 sec. -

DB Bicep Curls
Macalester Women's tennis Cycle 1 May 25th - June 19th Week 1 May 25th Day 1 Day 2 Day 3 Med. Ball Warm-Up - 1 x 10 each way Med. Ball Warm-Up - 1 x 10 each way Med. Ball Warm-Up - 1 x 10 each way Overhead throws, Chest Pass, Hip Thrusts, Overhead throws, Chest Pass, Hip Thrusts, Overhead throws, Chest Pass, Hip Thrusts, Side Toss Side Toss Side Toss Cuff Series - 2 x 15 each way Cuff Series - 2 x 15 each way Cuff Series - 2 x 15 each way Power Clean Deadlift x 6 1 arm DB Push Press 3 x 6 each arm Power Clean Deadlift x 6 x 6 St. Bar Shoulder Press x 10 x 6 x 6 (In Front) x 10 x 6 x 6 x 10 x 6 Back Squat x 10 Half Squats x 10 Back Squat x 10 x 10 x 10 x 10 x 10 x 10 x 10 DB Bench Press x 10 3 way Delt Raises 3 x 10 each way DB Bench Press x 10 x 10 (Lat., Front, Rear) x 10 x 10 Lateral Lunges 3 x 10 each leg x 10 x 10 Lat. Pull Down 3 x 10 Lateral Step Up Cross Over 3 x 10 each leg Lunges 3 x 10 each leg Lying DB Ext. Rot. 3 x 10 1 arm Bent Over row 3 x 10 Seated Row 3 x 10 3 way Lying Tricep Ext. 2 x 10 each way Lying Delt Raise and Pull 3 x 10 DB Rear Delt Raise 3 x 10 3 way Bicep Curls 2 x 10 each way 90/90 External Rotation 3 x 10 Empty Bottle 3 x 10 Tricep Push Down 3 x 10 Forearm Series 2 x 15 Forearm series 2 x 15 DB Bicep Curls 3 x 10 Choose Ab Routine: Shoulder Stretches: Choose Ab Routine: Choose Ab Routine: Shoulder Stretches: Shoulder Stretches: Macalester Women's tennis Cycle 1 May 25th - June 19th Week 2 June 1st Day 1 Day 2 Day 3 Med. -

Bodyweight Inclined Reverse Crunch 3 to 4 10 Reps
HIT THESE LIFTS FOR HUGE RESULTS Not all fitness pursuits lead to dramatic visible changes — and that’s perfectly OK! If, on the other hand, you’re in the mood for more muscles, you may consider turning to hypertrophy training for the solution. Delts of doom, a big, round peach, and solid legs take time, work, and attention. You have to be deliberate, but you can choose where to add muscle through specific exercise selection, using a moderate to high training volume, and keeping rest times short. When you train this way, you can match the heart and soul of your workout with the addition of muscles you can’t help but snap photos of (overhead lighting, anyone?). One way you can amplify your results is paying extra attention to building your rear delts, glutes, and hamstrings. You can add in the quads and abs to round it out, too. It’s kind of like taking a vitamin for these body parts! Pop in this workout once a week if you’re already following a program, or complete it two to three times per week if you’re not. Think of this as a boost for you to get muscles that look like you must spend all day in the gym. bignessproject.com and unapologeticallystrong.com 1 VITAMIN WORKOUT For this workout, complete 3 to 4 straight sets of 10 reps of each exercise. That means you’ll finish all sets of the each exercise before moving on to the next, resting 30 to 60 seconds between each set. Click here to revisit this workout video EXERCISE SETS REPS Dumbbell Bent-Over Rear-Delt Raise 3 to 4 10 Reps Bodyweight Inclined Reverse Crunch 3 to 4 10 Reps Bodyweight Frog Pump 3 to 4 10 Reps Valslide Eccentric SHELC 3 to 4 10 Reps Bodyweight Sissy Squat 3 to 4 10 Reps bignessproject.com and unapologeticallystrong.com 2 DUMBBELL BENT-OVER REAR-DELT RAISE Muscle Focus • Stand tall and hold two dumbbells with slightly bent elbows so they hang straight down in front of you. -
Week 1 Week 2 Week 3 Week 4 DAVE's VIF
THE TOOLS YOU NEED TO BUILD THE BODY YOU WANT® Store Workouts Diet Plans Expert Guides Videos Tools DAVE’S V.I.F. MASS BUILDING PROGRAM This program tackles 3 of the 5 different types of workouts that will hopefully keep your body Main Goal: Build Muscle Time Per Workout: 45-60Mins growing in the right direction. Each phase is 4 Training Level: Intermediate Equipment: Barbell, Bodyweight, weeks. Program Duration: 12 Weeks Cables, Dumbbells, EZ Bar, Link to Workout: https://www.muscleandstrength.com/ Days Per Week: 4 Days Machines workouts/daves-vif-mass-building-program.html Author: Dave Herber PHASE 1: Volume (Weeks 1 - 4) Week 1 Exercise Sets Reps Day 1: Back & Traps Pull Ups 2 As Many As Possible Barbell Rows 2 10 Seated Cable Rows 2 10 Hyperextensions 2 10 Superset Upright Rows 2 10 Dumbbell Shrugs 2 10 Day 2: Chest & Shoulders Bench Press 2 10 Superset Incline Dumbbell Bench Press 2 10 Decline Pushups 2 As Many As Possible Dumbbell Military Press 2 10 Dumbbell Rear Laterals 2 10 Day 3: Legs Squat 2 10 Leg Press 2 10 Stiff Legged Deadlifts 2 10 Dumbbell Step Ups 2 10 Standing Calf Raise 2 10 Day 4: Arms Barbell Curls 2 10 Close Grip Bench Press 2 10 Superset Lying Tricep Extension 2 10 Standing Dumbbell Curls 2 10 Superset Preacher Curls 2 10 Tricep Kickbacks 2 10 Rest 60 Secs between sets. Week 2 Exercise Sets Reps Day 1: Back & Traps Pull Ups 3 As Many As Possible Barbell Rows 3 8 Seated Cable Rows 3 8 Hyperextensions 3 8 Superset Upright Rows 3 8 Dumbbell Shrugs 3 8 Day 2: Chest & Shoulders Bench Press 3 8 Superset Incline Dumbbell Bench Press 3 8 Decline Pushups 3 As Many As Possible Dumbbell Military Press 3 8 Dumbbell Rear Laterals 3 8 Day 3: Legs Squat 3 8 Leg Press 3 8 Stiff Legged Deadlifts 3 8 Dumbbell Step Ups 3 8 Standing Calf Raise 3 8 Day 4: Arms Barbell Curls 3 8 Close Grip Bench Press 3 8 Superset Lying Tricep Extension 3 8 Standing Dumbbell Curls 3 8 Superset Preacher Curls 3 8 Tricep Kickbacks 3 8 Increase weight. -

The Perfect Summer Shred Workouts and Cardio
THE PERFECT SUMMER SHRED WORKOUTS AND CARDIO 1 | | THE PERFECT SUMMER SHRED: WORKOUTS AND CARDIO THE RULES These rules apply to all THE PERFECT SUMMER SHRED: of the workouts. WORKOUTS AND CARDIO * The sets and reps don’t include warm-up If you’re looking to burn down the old you on a tight deadline this summer, then send sets. Perform as many those old straight-set workouts packing! To get ultra-ripped, you need to amp up your as you need, but never overall training intensity. In this program, that means supersets, dropsets, clusters, and take your warm-ups density training. near muscle failure. • After warm-ups, Stick with this program for at least 4 weeks to give it the best chance to work. Along choose a weight that with the nutrition and supplementation guidelines outlined in the Cellucor Summer allows you to approach Shred Superfeature, it should be enough to kick-start some serious progress. While this muscle failure by the target rep listed. workout will increase your conditioning, the primary goal is to to get you leaner Adjust the weight by boosting your metabolism based on the parameters outlined in the 5 Musts of The on follow-up sets as Fat-Loss Workout article. necessary. • Train past failure using However, be warned that this program is fairly advanced as written. Adjust the volume advanced intensity and intensity downward depending on your ability if you feel like you’re struggling to boosters only where recover between workouts. noted in the program. LIFTING: TWO-ON/ONE-OFF SPLIT CARDIO: FIVE-ON/TWO-OFF SPLIT • Beginning-level lifters MONDAY MONDAY should reduce the training volume by Chest, Triceps, Abs HIIT eliminating 1-2 exercises from the TUESDAY TUESDAY middle of the routine Legs Steady-State Cardio and reduce the loads lifted. -
15 Inhome Exercises.Pdf
Transform your body! Awesome In-Home 15 exercises Table of contents Welcome……………………………………………………...0 Modified Push Up……………………………………………1 Spiderman Abs……………………………………………….2 Situp Ball Press……………………………………………….3 Bicep Curl…………………………………………………….4 Glute Squeeze……………………………………………….5 Back Pull………………………………………………………6 Delt Raise……………………………………………………..7 Overhead Press………………………………………………8 Ab Tuck………………………………………………………..9 Row…………………………………………………………..10 Mid-Back Row………………………………………………11 Tricep Shoulder Press……………………………………...12 Leg Ups……………………………………………………...13 Squats………………………………………………………..14 Tick Tock……………………………………………………..15 About My Fit Gals…………………………………………..16 welcome! Are you ready to get fit? Congrats on taking the next steps towards your personal fitness journey by downloading this ebook. It is intended to be a useful resource as you experiment doing new exercises geared towards increasing your strength, making you more toned, and ultimately helping you live a more fulfilling life through fitness. My Fit Gals has presented you with 15 awesome, in-depth exercises you can do in the comfort of your own home. Compared to the gym, in-home exercise serves as more convenient and private, which should serve as an advantage in accomplishing your fitness & lifestyle goals. So go ahead, tackle these exercises and take charge towards your transformation! P.S. - Several of these exercises require resistance bands. If you need a set, I recommend these Stephanie Mountain Founder & Personal Trainer 1 Modified Push-up About Let’s be honest: push-ups are hard! Especially if you’re just getting into a fitness routine, sometimes you don’t have the strength needed to perform a full push-up and that’s okay! Modifying an exercise is a great way to build up your strength towards a particular move so you can one day perform the real thing. -
Exercises for the Traps (Trapezius) Shoulder Shrugs Major Muscle Group: Trapezius Grasp the Bar with Shoulder-Width Or Slightly Wider Overhand Grip
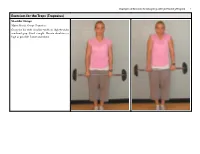
Examples of Exercises for Designing a Weight Training Program 1 Exercises for the Traps (Trapezius) Shoulder Shrugs Major Muscle Group: Trapezius Grasp the bar with shoulder-width or slightly wider overhand grip. Stand straight. Elevate shoulders as high as possible. Lower and repeat. Examples of Exercises for Designing a Weight Training Program 2 Lower Pulley Row to Neck Major Muscle Group: Trapezius Other Muscles Worked: Biceps, Middle back, Shoulders Sit at a seated row station and grab the ends of the rope using a palm-down grip. Sit with your knees slightly bent and your back straight. Do not lean back — your back should be almost completely ver- tical. Pull the rope back and up to neck height. Your elbows should be out, away from your sides. Return slowly to the starting position. Dumbbell Incline Shoulder Raise Major Muscle Group: Trapezius Sit down on an incline bench with the dumbbells resting on your lower thigh. Kick the weights to your shoulders and lean back. Position the dumbbells above your shoulders with your elbows extended. Raise your shoulders toward the dumbbells as high as possible. Lower shoulders to bench and repeat. Examples of Exercises for Designing a Weight Training Program 3 Upright Row Major Muscle Group: Trapezius Other Muscle Worked: Biceps, Shoulders Standing upright, grasp a barbell with your hands about shoulder-width apart. Let the bar hang straight down in front of you. Keep your body and wrists straight. Pull the bar straight up toward your chin, keeping it close to your body. Lower slowly to the starting position. Keep your back straight, making sure not to swing. -

Gym Workout Tracker Template
Gym workout tracker template Continue Kristin Blackburn No Gym Time? No problem! Get in great shape in your place with these five basic tools (and one easy workout). Kristin Blackburn Who says you need to cost gym fancy equipment to get in shape? Not us! For less than 50 bucks you can score enough gear to train your entire body at home without sacrificing precious space. Key: Choose parts that are not only efficient but multifunctional, says George Vafiades, co-owner of As One Gym in New York. Advertising Advertising Christine Blackburn Five tools on the Vafiades shopping list target your entire body, while increasing strength, endurance and flexibility. Put them to use with a chain developed by Vafiades. It burns 250 calories, makes you stronger for two weeks and slimmer at four, and revs up your metabolism, so you burn calories long after you've finished exercising. Do this at least three times a week by jumping rope 50 times between moves. (To keep warm, do a few minutes of squats, with your hands over your head; to cool down, try stretching). Amazon.com Resistance: Use these oversized gums that come in three resistance levels to train the upper and lower body. ($40 for a set of four; amazon.com) Dumbbells: Transform your entire body - arms, legs, back, chest - with one pair of dumbbells. ($25; amazon.com) Stability ball: This ball puts the body in an unstable position, forcing you to use (and strengthen!) your core. Pair with dumbbells or resistance bands to allow up intensity exercises like overhead presses. -

Swimming Cycle 3 July 11Th - Aug
Swimming Cycle 3 July 11th - Aug. 5th Week 9 July 11th Day 1 Day 3 Plate Warm-Up 1 x 10 each way Plate Warm-Up 1 x 10 each way Wood Chops, Standing Russian Twist, Squat w/ big circle, Wood Chops, Standing Russian Twist, Squat w/ big circle, Lateral Lunge and Press Lateral Lunge and Press Shoulder Warm Up 1 x 10 each way Shoulder Warm Up 1 x 10 each way Standing 90/90, Standing Rear Delt Pull, Inverted 45. Rear Delt Raise, Lying Ext. Rot. Standing 90/90, Standing Rear Delt Pull, Inverted 45. Rear Delt Raise, Lying Ext. Rot. Back Squat/Smith Machine x 6 Leg Press x 6 ss w/ S.L. Bridges 2 x 8 each leg x 6 ss w/ S.L. Bridges 2 x 15 each leg x 6 x 6 x 6 Bench Press x 6 Lunges 3 x 6 each leg ss w/ S.L. S.B. Hamstring Curls 3 x 8 each leg x 6 DB Incline chest Press 3 x 6 x 6 S.L. Machine Hamstring Curls 3 x 8 each leg 45 Degree Delt Raise 3 x 6 Cable Delt Pull Down 3 x 6 Seated Row 3 x 6 Front Delt Raise 3 x 6 DB Shoulder Press 3 x 6 Rev Grip Lat. Pull Down 3 x 6 Lat. Pull Down 3 x 6 Cable Glute Kicks 3 x 8 each leg Lying DB External Rotation 2 x 40 DB Alternating Shoulder Press 3 x 6 each arm Any Bicep Exercise 3 x 6 Lying DB External Rotation 2 x 40 Any Tricep Exercise 3 x 6 Any Bicep Exercise 3 x 6 Cable rear Delt Pull 3 x 6 Any Tricep Exercise 3 x 6 Front Delt Raise w/ Lateral Drop 3 x 6 Choose Ab Routine: see website Shoulder Stretches: see website Choose Ab Routine: see website Shoulder Stretches: see website Swimming Cycle 3 July 11th - Aug. -
Level I Offseason Weight Program Summer 2015
Level I Offseason Weight Program Summer 2015 Week 1 Week 2 Week 3 Day 1 Day 1 Day 1 Hang Clean Pull 5x3 Hang Clean Pull 5x3 Hang Clean Pull 5x3 Leg Sweeps 3x5 Leg Sweeps 3x5 Leg Sweeps 3x5 SL TKE 3x15 SL TKE 3x15 SL TKE 3x15 DB SL Squat 10x6 DB SL Squat 9x6 DB SL Squat 8x6 Hip Circuit 1 3x5 Hip Circuit 1 3x5 Hip Circuit 1 3x5 BB Calf Raise 3x15 BB Calf Raise 3x15 BB Calf Raise 3x15 DB Deadlifts 5x5 DB Deadlifts 5x5 DB Deadlifts 5x5 Bench Lying Neck 3x10 Bench Lying Neck 3x10 Bench Lying Neck 3x10 4 Way ABS 4 Way ABS 4 Way ABS Day 2 Day 2 Day 2 Hang Snatch Pulls 5x3 Hang Snatch Pulls 5x3 Hang Snatch Pulls 5x3 Shoulder 2 3x5 Shoulder 2 3x5 Shoulder 2 3x5 1 Arm Rear Delt Raise 3x5 1 Arm Rear Delt Raise 3x5 1 Arm Rear Delt Raise 3x5 DB Incline Combo 10x6 DB Incline Combo 9x6 DB Incline Combo 8x6 OH Tricep Ext. 4x5 OH Tricep Ext. 4x5 OH Tricep Ext. 4x5 Skydiver 4x15s Skydiver 4x15s Skydiver 4x15s Bent Over Row 10x6 Bent Over Row 9x6 Bent Over Row 8x6 DB Curl Combo 4x5 DB Curl Combo 4x5 DB Curl Combo 4x5 AB Circuit 1 3x10 AB Circuit 1 3x10 AB Circuit 1 3x10 Fast Fingers x30s each Fast Fingers x45s each Fast Fingers x60s each Day 3 Day 3 Day 3 Below Knee Cln Pull 5x3 Below Knee Cln Pull 5x3 Below Knee Cln Pull 5x3 Hip Circuit 2 2x5 Hip Circuit 2 2x5 Hip Circuit 2 2x5 Wt.