Performance- Enhancing Drugs AI Performance Drugs INT 8/7/02 2:06 PM Page 2
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

20 Top-Ten Shot
Last Updated – 21.10.2015 EUROPEAN ALL TIME RANKINGS MEN SHOT PUT M35 – 39 (Weight 7.250 kg) DISTANCE NAME NATION BORN MEET PLACE MEET DATE 22.10 Andrei Mikhnevich BLR 12.07.1976 Minsk 11.08.2011 21.35 Aleksander Baryshnikov RUS 11.11.1948 Sochi 10.06.1984 20.91 Dragan Perić SRB 08.05.1964 Edmonton 04.08.2001 20.90 Saulius Kleiza LTU 02.04.1964 Kaunas 14.05.1999 20.84 Matti Yrjölä FIN 26.03.1938 Kobemäki 06.07.1976 20.79 Milan Haborak SVK 11.01.1973 Pacov 11.07.2008 20.78 Roman Virastyuk UKR 20.04.1968 Kiev 03.07.2003 20.70 Wladyslaw Komar POL 11.04.1940 Chemnitz 26.06.1977 20.67 Hamza Alic BIH 20.01.1979 Bistrica 30.05.2015 20.54 Jovan Lazarevic SRB 03.05.1952 Minsk 26.07.1990 INDOOR 21.04 Gheorghe Guset ROU 18.05.1968 Bucarest 18.02.2006 20.85 Mark Proctor GBR 15.01.1963 Kings Lynn 18.01.1998 20.76 Valery Voykin RUS 14.10.1945 Leningrado 29.01.1983 * * * SHOT PUT M40 – 44 (Weight 7.250 kg) DISTANCE NAME NATION BORN MEET PLACE MEET DATE 20.44 Ivan Ivancic SRB 06.12.1937 Beograd 05.07.1980 20.34 Dragan Perić SRB 08.05.1964 Zenica 02.09.2006 20.04 Mark Proctor GBR 15.01.1963 Manchester 30.08.2005 19.97 Waldyslaw Komar POL 11.04.1940 Warsaw 06.09.1980 19.77 Pierre Colnard FRA 18.02.1929 Colombes 18.07.1970 19.18 Matti Yrjölä FIN 26.03.1938 Somero 16.07.1978 19.10 Paolo Dal Soglio ITA 29.07.1970 Savona 10.06.2012 19.09 Ferdinand Schladen GER 24.05.1939 Höhr 06.09.1981 19.08 Paul Edwards GBR 16.02.1959 Luton 16.06.1999 19.07 Alessandro Andrei ITA 03.01.1959 Pescara 23.07.2000 INDOOR 19.48 Ivan Ivancic SRB 06.12.1937 Sindelfingen 02.03.1980 * * * SHOT PUT M45 – 49 (Weight 7.250 kg) DISTANCE NAME NATION BORN MEET PLACE MEET DATE 20.77 Ivan Ivancic SRB 06.12.1937 Coblenz 31.08.1983 18.22 Gudmund. -

Lance Armstrong Has Something to Get Off His Chest
Texas Monthly July 2001: Lanr^ Armstrong Has Something to . Page 1 of 17 This copy is for your personal, non-commercial use only. For public distribution to your colleagues, clients or customers, contact [email protected] for reprint information and fees. (EJiiPfflNITHIS Lance Armstrong Has Something to Get Off His Chest He doesn't use performance-enhancing drugs, he insists, no matter what his critics in the European press and elsewhere say. And yet the accusations keep coming. How much scrutiny can the two-time Tour de France winner stand? by Michael Hall In May of last year, Lance Armstrong was riding in the Pyrenees, preparing for the upcoming Tour de France. He had just completed the seven-and-a-half-mile ride up Hautacam, a treacherous mountain that rises 4,978 feet above the French countryside. It was 36 degrees and raining, and his team's director, Johan Bruyneel, was waiting with a jacket and a ride back to the training camp. But Lance wasn't ready to go. "It was one of those moments in my life I'll never forget," he told me. "Just the two of us. I said, 'You know what, I don't think I got it. I don't understand it.1 Johan said, 'What do you mean? Of course you got it. Let's go.' I said, 'No, I'm gonna ride all the way down, and I'm gonna do it again.' He was speechless. And I did it again." Lance got it; he understood Hautacam—in a way that would soon become very clear. -
LIBRARY All Rights Reserved
LIBRARY All rights reserved INFORMATION TO ALL USERS The quality of this reproduction is dependent upon the quality of the copy submitted. In the unlikely event that the author did not send a com plete manuscript and there are missing pages, these will be noted. Also, if materia! had to be removed, a note will indicate the deletion. Published by ProQuest LLC (2017). Copyright of the Dissertation is held by the Author. All rights reserved. This work is protected against unauthorized copying under Title 17, United States C ode Microform Edition © ProQuest LLC. ProQuest LLC. 789 East Eisenhower Parkway P.O. Box 1346 Ann Arbor, Ml 48106- 1346 fA NEW DAWN RISING':1 AN EMPIRICAL AND SOCIAL STUDY CONCERNING THE EMERGENCE AND DEVELOPMENT OF ENGLISH WOMEN'S ATHLETICS UNTIL 1980 Gregory Paul Moon Submitted in part fulfilment for the degree of Doctor of Philosophy at Roehampton Institute London for the University of Surrey August 1997 1Sutton and Cheam Advertiser 1979. Dawn Lucy (later Gaskin) was the first athlete I ever coached. Previously, she had made little progress for several years. In our first season together her improvement was such that the local newspaper was prompted to address her performances with this headline. ABSTRACT This study explores the history of English women's athletics, from the earliest references up to 1980. There is detailed discussion of smock racing and pedestrianism during the eighteenth- and nineteenth-centuries, but attention is focused on the period from 1921, when international and then domestic governing bodies were formed and athletics .became established as a legitimate sporting activity for women. -

Le Dopage Existe Dans Le Sport N'est Pas Un Scandale
Le point sur les récentes affaires de dopage (1997-1999) Thierry-Roland Canizares To cite this version: Thierry-Roland Canizares. Le point sur les récentes affaires de dopage (1997-1999). Sciences pharma- ceutiques. 1999. dumas-01563861 HAL Id: dumas-01563861 https://dumas.ccsd.cnrs.fr/dumas-01563861 Submitted on 18 Jul 2017 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. AVERTISSEMENT Ce document est le fruit d'un long travail approuvé par le jury de soutenance et mis à disposition de l'ensemble de la communauté universitaire élargie. Il n’a pas été réévalué depuis la date de soutenance. Il est soumis à la propriété intellectuelle de l'auteur. Ceci implique une obligation de citation et de référencement lors de l’utilisation de ce document. D’autre part, toute contrefaçon, plagiat, reproduction illicite encourt une poursuite pénale. Contact au SID de Grenoble : [email protected] LIENS LIENS Code de la Propriété Intellectuelle. articles L 122. 4 Code de la Propriété Intellectuelle. articles L 335.2- L 335.10 http://www.cfcopies.com/juridique/droit-auteur -

Peso Olímpico. Datos Mujeres
LOS LANZAMIENTOS EN LOS JJOO PROGRESIÓN RECORD OLÍMPICO JUEGOS OLÍMPICOS. PODIUM LANZAMIENTO DE PESO. MUJERES LANZAMIENTO DE PESO MUJERES • 13.14 Micheline Ostermeyer FRA London Aug 04, 1948 SEDE ORO PLATA BRONCE • 13.75 Micheline Ostermeyer FRA London Aug 04, 1948 London 1948 Micheline Ostermeyer FRA 13,75 Amelia Piccinini ITA 13,09 Ine Schäffer AUT 13,08 • 13.88 Klavdiya Tochenova URS Helsinki Jul 26, 1952 Helsinki 1952 Galina Zybina URS 15,28 Marianne Werner FRG 14,57 Klavdiya Tochenova URS 14,50 • 13.89 Marianne Werner FRG Helsinki Jul 26, 1952 Melbourne 1956 Tamara Tishkevich URS 16,59 Galina Zybina URS 16,53 Marianne Werner FRG 15,61 • 15.00 Galina Zybina URS Helsinki Jul 26, 1952 Rome 1960 Tamara Press URS 17,32 Johanna Lüttge GDR 16,61 Earlene Brown USA 16,42 • 15.28 Galina Zybina URS Helsinki Jul 26, 1952 Tokyo 1964 Tamara Press URS 18,14 Renate Garisch GDR 17,61 Galina Zybina URS 17,45 • 16.35 Galina Zybina URS Melbourne Nov 30, 1956 Mexico 1968 Margitta Gummel GDR 19,61 Marita Lange GDR 18,78 Nadezhda Chizhova URS 18,19 • 16.48 Galina Zybina URS Melbourne Nov 30, 1956 Munich 1972 Nadezhda Chizhova URS 21,03 Margitta Gummel GDR 20,22 Ivanka Khristova BUL 19,35 • 16.53 Galina Zybina URS Melbourne Nov 30, 1956 Montreal 1976 Ivanka Khristova BUL 21,16 Nadezhda Chizhova URS 20,96 Helena Fibingerova TCH 20,67 • 16.59 Tamara Tishkevich URS Melbourne Nov 30, 1956 Moscow 1980 Ilona Slupianek GDR 22,41 Esfir Krachevskaya URS 21,42 Margitta Pufe GDR 21,20 • 17.32 Tamara Press URS Rome Sep 02, 1960 Los Angeles 1984 Claudia Losch FRG 20,48 -

Downloadable Results (Pdf)
Muller British Athletics Championships Manchester Regional Arena Heptathlon From Friday 25 June to Sunday 27 June 2021 Women 's Shot Put LETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS RESULTS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS 26 June 2021 TIME TEMPERATURE Start 15:30 14°C 78 % End 15:5214°C 78 % MARK COMPETITOR NAT AGE Record Date WR22.63 Natalya LISOVSKAYA URS 24 7 Jun 1987 NR19.36 Judy OAKES GBR 30 14 Aug 1988 CR18.76 Judy OAKES GBR 30 6 Aug 1988 SR17.88 Sophie MCKINNA GBR 26 4 Sep 2020 POSSTART COMPETITOR AGE MARK POINTS 1 3 Ellen BARBER 23 13.30 747 YEOVIL 2 6 Katie STAINTON 26 12.02 662 SB BIRCHFIELD HARRIERS 3 2 Natasha SMITH 21 12.01 662 SB BIRCHFIELD HARRIERS 4 8 Ashleigh SPILIOPOULOU 22 10.88 587 ENFIELD & HARINGEY H 5 7 Ella RUSH 17 10.54 565 AMBER VALLEY 6 5 Emily TYRRELL 19 9.43 492 TEAM BATH 7 1 Emma CANNING 24 8.18 411 EDINBURGH AC 4 Amaya SCOTT-RULE 20 DNS 0 SOUTHAMPTON SERIES 1 2 3 1 Emma CANNING EDAC X 8.18 X 2 Natasha SMITH BIRCHFIELD 11.57 12.01 11.45 3 Ellen BARBER YEOVIL 13.09 13.22 13.30 4 Amaya SCOTT-RULE SOTON 5 Emily TYRRELL BATH X 8.70 9.43 6 Katie STAINTON BIRCHFIELD 12.02 11.98 X 7 Ella RUSH AMBER V 10.54 X X 8 Ashleigh SPILIOPOULOU ENFIELD 10.88 10.83 10.27 GREAT BRITAIN & N.I. -
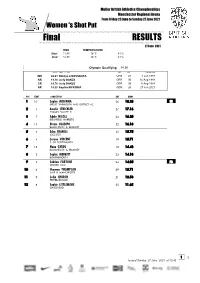
Downloadable Results (Pdf)
Muller British Athletics Championships Manchester Regional Arena From Friday 25 June to Sunday 27 June 2021 Women 's Shot Put HLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS Final RESULTS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS ATHLETICS A 27 June 2021 TIME TEMPERATURE Start 11:38 16°C 81 % End 12:3816°C 81 % Olympic Qualifying 18.50 MARK COMPETITOR NAT AGE Record Date WR22.63 Natalya LISOVSKAYA URS 24 7 Jun 1987 NR19.36 Judy OAKES GBR 30 14 Aug 1988 CR18.76 Judy OAKES GBR 30 6 Aug 1988 SR18.28 Sophie MCKINNA GBR 26 27 Jun 2021 POSSTART COMPETITOR AGE MARK 1 10 Sophie MCKINNA 26 18.28 SR GREAT YARMOUTH AND DISTRICT AC 2 5 Amelia STRICKLER 27 17.16 THAMES VALLEY H 3 7 Adele NICOLL 24 16.20 BIRCHFIELD HARRIERS 4 11 Divine OLADIPO 22 16.18 BLACKHEATH & BROMLEY 5 3 Eden FRANCIS 32 15.75 LEICESTER 6 4 Serena VINCENT 19 15.71 C OF PORTSMOUTH 7 12 Nana GYEDU 18 14.48 BLACKHEATH & BROMLEY 8 2 Sophie MERRITT 23 14.18 BOURNEMOUTH 9 1 Sabrina FORTUNE 24 14.05 PB DEESIDE AAC 10 6 Shaunna THOMPSON 29 13.71 SALE H MANCHESTER 11 9 Lydia CHURCH 21 12.53 PETERBOROUGH 12 8 Sophie LITTLEMORE 25 11.65 GATESHEAD 1 2 Issued Sunday, 27 June 2021 at 12:42 Shot Put Women - Final RESULTS SERIES 1 2 3 4 5 6 1 Sabrina FORTUNE DEESIDE 13.62 14.05 13.15 -
Spring 2010 U.S
IN THIS ISSUE SPRING 2010 School w ota La ota nes Min of y sit ver Uni the for e Magazin The Alumni fight for human rights on U.S. and global fronts. Former Justice O’Connor Visits • Justice Thomas Seminar • Legal Aid for Mille Lacs Band • Summer CLE Rights on Their Side S P R I N G 2 0 1 0 Perspectives FORMER JUSTICE O’CONNOR VISITS • JUSTICE THOMAS SEMINAR• LEGAL AID FOR MILLE LACS BAND www.law.umn.edu PAID U.S. Postage Permit No. 155 Nonprofit Org. Minneapolis, MN N225 Mondale Hall 229 19th Avenue South Minneapolis, MN 55455 Partners in Excellence Annual Fund Update Dear Friends and Fellow Alumni: As National Co-Chairs of this year’s Partners in DEAN LAW ALUMNI BOARD AND Excellence annual fund drive, we are pleased that many David Wippman BOARD OF VISITORS 2009-10 of you have chosen to benefit the Law School with Grant Aldonas (’79) your generosity through gifts to the Law School Fund. ASSISTANT DEAN AND Deborah Amberg (’90)† In this time of varied economic challenges, you have CHIEF OF STAFF Austin Anderson (’58) recognized the importance of contributing to the Law Nora Klaphake Justice Paul Anderson (’68) School, particularly in light of rapidly dwindling state Former Chief Justice support. We thank all of you who have given so far DIRECTOR OF COMMUNICATIONS Russell Anderson (’68) and wish to specially acknowledge the generosity of Cynthia Huff Albert (Andy) Andrews (’66)† this year’s Fraser Scholars and Dean’s Circle donors James J. Bender (’81) (through April 15, 2010). -

Respondents 25 Sca 001378
Questions about a Champion "If a misdeed arises in the search for truth, it is better to exhume it rather than conceal the truth." Saint Jerome. "When I wake up in the morning, I can look in the mirror and say: yes, I'm clean. It's up to you to prove that I am guilty." Lance Armstrong, Liberation, July 24,2001. "To deal with it, the teams must be clear on ethics. Someone crosses the line? He doesn't have the right to a second chance!" Lance Armstrong, L'Equipe, April 28, 2004. Between the World Road Champion encountered in a Norwegian night club, who sipped a beer, talked candidly, laughed easily and never let the conversation falter, and the cyclist with a stem, closed face, who fended off the July crowd, protected by a bodyguard or behind the smoked glass of the team bus, ten years had passed. July 1993. In the garden of an old-fashioned hotel near Grenoble, I interviewed Armstrong for three hours. It was the first professional season for this easygoing, slightly cowboyish, and very ambitious Texan. I left with a twenty-five-page interview, the chapter of a future book11 was writing about the Tour de France. I also took with me a real admiration for this young man, whom I thought had a promising future in cycling. Eight years later, in the spring of 2001, another interview. But the Tour of 1998 had changed things. Scandals and revelations were running rampant in cycling. Would my admiration stand the test? In August 1993, it was a happy, carefree, eloquent Armstrong, whom Pierre Ballester, met the evening after he won the World Championship in Oslo. -

Oy Joe T Cse on Septenber 5, Seven-Time Tour De France Champion Lance Armstron$ Made a the Story Went Off Like a Bomb
,rIer .oeattrIng. cancer I \ I rr ii \ tlq,_Uinning t?1e, .four )attlL,,W"H ffIfi$%TO5F LqIF iEig nt a[egdgtio n s qE- qqgg Fqrrbrrn- ,ncet?! -e n nanclng: cirugtrIs, ra,nce: Ssayq h.ers YiAd r"'Tr\rr,\rGLrJ }{tJ*, se*=W#:s?'--alf.q Mind-Blowinq lmages Oyef ttfe fronn Hurricane Katrlna PAGE 128 gffinF"ffgfs=ffifficrrlet'mnt. nis silaiowv Qcqsgrs ln courtqaornb #"qmfgna J.egaJ- Droceeclnps ,nd, ] - rreru#,sa#_ e# b:*flffiffi #*#ff 1r rerffiT { _ = # ud**H3ffi-ru *{trffiffit;ffiffiE &rytr#? ,; JtAcqw*u'l^t-- J-- oy Joe t cse On Septenber 5, seven-time Tour de France champion Lance Armstron$ made a The story went off like a bomb. Some observers said th= ,:-*--:s. remarkable announcement: He said that he was thinkin$ of end- was a grave one and that the case lbr Armstron$'s $ui1t \1 :: : r:. ing his retirement, at that point a mere six weeks old, and re- pelling. Others raised a flurry of criticism attacking rh- .---r joining his Discovery Channel team for a rufl at another title. and legality of leaking confidential lab results, the motn'e: -r-u Although Armstrong, 34,had previously said "only an absolute journalists and sources involved, and the aceurac), oi rhe :-: n miracle" would get him to race afain, his rationale for a return in question. As happens whenever Armstrong is accuse,l : -:- 2006, as published in theAustinAmerican-Statesman, was loud thin$, many of the reactions on both sides were characrer_.: :." and clear: "I'm thinking it's the best way to piss [the French] off." Sreater certainty than the available evidence seemed ro {-:-:r-:r. -

Winner of the 2007 Tour De France, Alberto Contador, As Well As His Astana Teammates Levi Leipheimer, Winner of the 2008 Tour Of
INSIDE THE UCI/ASO CONFLICT ABOUT ORGANIZING CYCLING AS A SPORT: THE UNIBET CASE BENOIT HANSEZ INTRODUCTION Winner of the 2007 Tour de France, Alberto Contador, as well as his Astana teammates Levi Leipheimer, winner of the 2008 Tour of California and ranked third in the 2007 Tour de France, and Andreas Klöden, ranked second in the 2004 and 2006 Tours de France, have been denied participation in the 2008 Tour de France. This results from a decision of the Tour de France organizer, Amaury Sport Organisation (ASO), not to invite the cycling team Astana to the cycling races that it organizes in 2008, including the 2008 Tour de France. ASO’s decision is based on the damage caused by this team during the 2007 Tour de France and to cycling in general, both in 2006 and 2007.1 Prior to the start of the 2006 Tour de France, Astana was excluded from the Tour de France after five of its riders were implicated in a doping scandal. In the 2007 Tour de France, Astana pulled out of the Tour de France after its team leader Alexander Vinokourov tested positive for blood doping on July 24, 2007. Astana’s doping problem is a small piece of a long history of drugs scandals that have tarnished the credit of professional cycling over the last decade. Suffice to remember the highly media covered Festina affair in the 1998 Tour de France where the Festina physician Willy Voet was caught by border officials with large quantities of doping products in his Festina team car, and several members of the team, including the 1997 World Champion Laurent Brochard, were arrested and admitted to taking erythropoietin (EPO).2 Suffice also to cite the name of the famous Spanish doping case, Operación Puerto, against Dr. -

Etn2000 12(Og)
■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■ Volume 46, No. 12 NEWSLETTERNEWSLETTER ■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■■track October 31, 2000 II(0.3)–1. Boldon 10.11; 2. Collins 10.19; 3. Surin 10.20; 4. Gardener 10.27; 5. Williams 10.30; 6. Mayola 10.35; 7. Balcerzak 10.38; 8. — Olympic Games — Lachkovics 10.44; 9. Batangdon 10.52. III(0.8)–1. Thompson 10.04; 2. Shirvington 10.13; 3. Zakari 10.22; 4. Frater 10.23; 5. de SYDNEY, Australia, September 22–25, 10.42; 4. Tommy Kafri (Isr) 10.43; 5. Christian Lima 10.28; 6. Patros 10.33; 7. Rurak 10.38; 8. 27–October 1. Nsiah (Gha) 10.44; 6. Francesco Scuderi (Ita) Bailey 11.36. Attendance: 9/22—97,432/102,485; 9/23— 10.50; 7. Idrissa Sanou (BkF) 10.60; 8. Yous- IV(0.8)–1. Chambers 10.12; 2. Drummond 92,655/104,228; 9/24—85,806/101,772; 9/ souf Simpara (Mli) 10.82;… dnf—Ronald Pro- 10.15; 3. Ito 10.25; 4. Buckland 10.26; 5. Bous- 25—92,154/112,524; 9/27—96,127/102,844; messe (StL). sombo 10.27; 6. Tilli 10.27; 7. Quinn 10.27; 8. 9/28—89,254/106,106; 9/29—94,127/99,428; VI(0.2)–1. Greene 10.31; 2. Collins 10.39; 3. Jarrett 16.40. 9/30—105,448; 10/1—(marathon finish and Joseph Batangdon (Cmr) 10.45; 4. Andrea V(0.2)–1. Campbell 10.21; 2. C. Johnson Closing Ceremonies) 114,714. Colombo (Ita) 10.52; 5. Watson Nyambek (Mal) 10.24; 3.