Services for Women Experiencing Multiple Disadvantage in England and Wales Contents
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Branches of the Bank of England
BRANCHES OF THE BANK OF ENGLAND Origin of Soon after the foundation end of the year seventy-three of the more the branches of the Bank of England in important banks in England and Wales had 1694, an anonymous writer on financial matters suspended payment. suggested that the Bank should establish In January 1826, with bank failures and branches which would be able to remit"multi commercial bankruptcies still continuing, the tudes of sums, great and small, to and from Court of Directors appointed a Committee to place to place ...without charges of carriage or consider and report "how far it may be dangers of Robberie" (Proposals for National practicable to establish branch banks ". Banks, 1696). The theme was taken up again Although the Committee were primarily con in 1721 by a pamphleteer who advocated the cerned to prevent a recurrence of the difficulties opening of branches "in the trading places of the previous year, they clearly did not over of the nation" whose managers would have look commercial considerations. Perhaps it authority "to lend a little". Such advice was because the latter issue, at least, was met with little response. Apart from introducing reasonably clear-cut that the Committee were Bank Post Bills(a) in 1724, in an attempt to able to report in only a week that they favoured reduce the risks to the mails of highway rob t e setting up of branches which, they con b ry, the Bank were little concerned during the � � SIdered, would greatly increase the Bank's own eIghteenth century with developments in the note circulation, would give the Bank greater financial system outside London and indeed control over the whole paper circulation, and were then frequently referred to as the ' Bank would protect the Bank against competition if of London '. -

The Role and Importance of the Welsh Language in Wales's Cultural Independence Within the United Kingdom
The role and importance of the Welsh language in Wales’s cultural independence within the United Kingdom Sylvain Scaglia To cite this version: Sylvain Scaglia. The role and importance of the Welsh language in Wales’s cultural independence within the United Kingdom. Linguistics. 2012. dumas-00719099 HAL Id: dumas-00719099 https://dumas.ccsd.cnrs.fr/dumas-00719099 Submitted on 19 Jul 2012 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. UNIVERSITE DU SUD TOULON-VAR FACULTE DES LETTRES ET SCIENCES HUMAINES MASTER RECHERCHE : CIVILISATIONS CONTEMPORAINES ET COMPAREES ANNÉE 2011-2012, 1ère SESSION The role and importance of the Welsh language in Wales’s cultural independence within the United Kingdom Sylvain SCAGLIA Under the direction of Professor Gilles Leydier Table of Contents INTRODUCTION ................................................................................................................................................. 1 WALES: NOT AN INDEPENDENT STATE, BUT AN INDEPENDENT NATION ........................................................ -

The Height of Its Womanhood': Women and Genderin Welsh Nationalism, 1847-1945
'The height of its womanhood': Women and genderin Welsh nationalism, 1847-1945 Item Type text; Dissertation-Reproduction (electronic) Authors Kreider, Jodie Alysa Publisher The University of Arizona. Rights Copyright © is held by the author. Digital access to this material is made possible by the University Libraries, University of Arizona. Further transmission, reproduction or presentation (such as public display or performance) of protected items is prohibited except with permission of the author. Download date 09/10/2021 04:59:55 Link to Item http://hdl.handle.net/10150/280621 'THE HEIGHT OF ITS WOMANHOOD': WOMEN AND GENDER IN WELSH NATIONALISM, 1847-1945 by Jodie Alysa Kreider Copyright © Jodie Alysa Kreider 2004 A Dissertation Submitted to the Faculty of the DEPARTMENT OF HISTORY In Partia' Fulfillment of the Requirements For the Degree of DOCTOR OF PHILOSOPHY In the Graduate College THE UNIVERSITY OF ARIZONA 2004 UMI Number: 3145085 Copyright 2004 by Kreider, Jodie Alysa All rights reserved. INFORMATION TO USERS The quality of this reproduction is dependent upon the quality of the copy submitted. Broken or indistinct print, colored or poor quality illustrations and photographs, print bleed-through, substandard margins, and improper alignment can adversely affect reproduction. In the unlikely event that the author did not send a complete manuscript and there are missing pages, these will be noted. Also, if unauthorized copyright material had to be removed, a note will indicate the deletion. UMI UMI Microform 3145085 Copyright 2004 by ProQuest Information and Learning Company. All rights reserved. This microform edition is protected against unauthorized copying under Title 17, United States Code. -

H 955 Great Britain
Great Britain H 955 BACKGROUND: The heading Great Britain is used in both descriptive and subject cataloging as the conventional form for the United Kingdom, which comprises England, Northern Ireland, Scotland, and Wales. This instruction sheet describes the usage of Great Britain, in contrast to England, as a subject heading. It also describes the usage of Great Britain, England, Northern Ireland, Scotland, and Wales as geographic subdivisions. 1. Great Britain vs. England as a subject heading. In general assign the subject heading Great Britain, with topical and/or form subdivisions, as appropriate, to works about the United Kingdom as a whole. Assign England, with appropriate subdivision(s), to works limited to that country. Exception: Do not use the subdivisions BHistory or BPolitics and government under England. For a work on the history, politics, or government of England, assign the heading Great Britain, subdivided as required for the work. References in the subject authority file reflect this practice. Use the subdivision BForeign relations under England only in the restricted sense described in the scope note under EnglandBForeign relations in the subject authority file. 2. Geographic subdivision. a. Great Britain. Assign Great Britain directly after topics for works that discuss the topic in relation to Great Britain as a whole. Example: Title: History of the British theatre. 650 #0 $a Theater $z Great Britain $x History. b. England, Scotland, Northern Ireland, and Wales. Assign England, Scotland, Northern Ireland, or Wales directly after topics for works that limit their discussion to the topic in relation to one of the four constituent countries of Great Britain. -

Health Inequalities in England, Scotland, and Wales
Edinburgh Research Explorer Health inequalities in England, Scotland and Wales: Stakeholders' accounts and policy compared Citation for published version: Harrington, B, Smith, K, Hunter, D, Marks, L, Blackman, T, McKee, L, Greene, A, Elliott, E & Williams, G 2009, 'Health inequalities in England, Scotland and Wales: Stakeholders' accounts and policy compared', Public Health, vol. 123, no. 1, pp. e24-e28. https://doi.org/10.1016/j.puhe.2008.10.010 Digital Object Identifier (DOI): 10.1016/j.puhe.2008.10.010 Link: Link to publication record in Edinburgh Research Explorer Document Version: Peer reviewed version Published In: Public Health Publisher Rights Statement: Harrington, B., Smith, K., Hunter, D., Marks, L., Blackman, T., McKee, L., Greene, A., Elliott, E., & Williams, G. (2009). Health inequalities in England, Scotland and Wales: Stakeholders' accounts and policy compared. Public Health, 123(1), e24-e28 doi: 10.1016/j.puhe.2008.10.010 General rights Copyright for the publications made accessible via the Edinburgh Research Explorer is retained by the author(s) and / or other copyright owners and it is a condition of accessing these publications that users recognise and abide by the legal requirements associated with these rights. Take down policy The University of Edinburgh has made every reasonable effort to ensure that Edinburgh Research Explorer content complies with UK legislation. If you believe that the public display of this file breaches copyright please contact [email protected] providing details, and we will remove access to the work immediately and investigate your claim. Download date: 04. Oct. 2021 Health Inequalities in England, Scotland, and Wales: stakeholders' accounts and policy compared B. -

The Bank of England and the Bank Act of 1844 Laurent Le Maux
Central banking and finance: the Bank of England and the Bank Act of 1844 Laurent Le Maux To cite this version: Laurent Le Maux. Central banking and finance: the Bank of England and the Bank Act of1844. Revue Economique, Presses de Sciences Po, 2018. hal-02854521 HAL Id: hal-02854521 https://hal.archives-ouvertes.fr/hal-02854521 Submitted on 8 Jun 2020 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Central banking and finance: the Bank of England and the Bank Act of 1844 Laurent LE MAUX* May 2020 The literature on the Bank of England Charter Act of 1844 commonly adopts the interpretation that it was a crucial step in the construction of central banking in Great Britain and the analytical framework that contrasts rules and discretion. Through examination of the monetary writings of the period and the Bank of England’s interest rate policy, and also through the systematic analysis of the financial aspect of the 1844 Act, the paper shows that such an interpretation remains fragile. Hence the present paper rests on the articulation between monetary history and the history of economic analysis and also on the institutional approach to money and banking so as to assess the consequences of the 1844 Act for the liquidity market and the relations between the central bank and finance. -

What Languages Are Spoken in England and Wales?
OCTOBER 2013 DYNAMICS OF DIVERSITY: EVIDENCE FROM THE 2011 CENSUS ESRC Centre on Dynamics of Ethnicity (CoDE) What languages are spoken in England and Wales? Summary • Languages other than English are part of the cultural – Middle Eastern and West Asian languages such as heritage of a significant and growing proportion of Arabic, Turkish, Persian, and Kurdish; the British population. – South Asian languages such as Urdu, Panjabi, • In 2011, 8% of the population reported a main language and Bengali; other than English (or Welsh in Wales) and it is likely that this is a small fraction of all people in England and Wales – East and South-East Asian languages such as who consider another language a part of their lives. Chinese, Vietnamese, and Thai; • The languages found in England and Wales are diverse: – East African languages such as Somali, Amharic, and Tigrinya; – from languages local to this region such as Welsh and Irish, to other European languages such as – Nigerian and other West African languages such as French, Portuguese, and Polish; Yoruba and Igbo. Figure 1: Twenty largest non-English main languages by number of speakers in England and Wales, 2011 Number of main language speakers 0100,000 200,000 300,000 400,000 500,000 600,000 Polish 546,174 Panjabi 273,231 Urdu 268,680 Bengali 221,403 Gujarati 213,094 Arabic 159,290 French 147,099 Chinese, Other 141,052 Portuguese 133,453 Spanish 120,222 Tamil 100,689 Turkish 99,423 Italian 92,241 Somali 85,918 Lithuanian 85,469 German 77,240 Persian/Farsi 76,391 Tagalog or Filipino 70,342 Romanian 67,586 Russian 67,366 Click here for data in Excel 1 www.ethnicity.ac.uk What languages are spoken in England and Wales? • Non-English languages are spread unevenly across Leicester, Southall Broadway in Ealing, Spinney Hills in various areas of England and Wales. -

Memorandum to the Constitutional and Legislative Affairs Committee of the National Assembly’S Inquiry Into the Establishment of a Separate Welsh Jurisdiction
MEMORANDUM TO THE CONSTITUTIONAL AND LEGISLATIVE AFFAIRS COMMITTEE OF THE NATIONAL ASSEMBLY’S INQUIRY INTO THE ESTABLISHMENT OF A SEPARATE WELSH JURISDICTION Professor Dan Wincott Blackwell Professor of Law and Society at Cardiff Law School Co-Chair of the Wales Governance Centre, Cardiff University Emyr Lewis Partner, Morgan Cole Solicitors Senior Fellow Wales Governance Centre, Cardiff University Summary 1.1 Jurisdiction relates to the question of “Who has legal authority within a particular legal framework to do what in respect of what, whom and where?” 1.2 Within the framework of the UK constitution, there already exist a distinct Welsh legislative and executive jurisdiction, and in certain limited areas, judicial jurisdiction through distinct tribunals and other fora for particular types of cases. 1.3 The concept of jurisdiction within the UK is complex. Even the currently recognised jurisdictions can only be said to be “separate” up to a point. 1.4 There already exists such a thing as a body of law which applies to Wales. The differences between this and the law which applies in England are likely to increase over time. 1.5 It is essential that Courts in Wales decide cases on the basis of distinct Welsh Law and that Lawyers can advise and represent their clients on this basis. 1.6 There is a need to plan now for the increasing divergence that appears to be an inevitable consequence of political reality. 1.7 Whatever happens, lawyers advising clients in Wales and judges hearing cases in Wales must have the necessary knowledge of Welsh law. 1.8 Jurisdiction over only devolved matters, as in a federal state, would not be in accordance with the UK model, and could create intractable problems. -
Worcestershire Has Fluctuated in Size Over the Centuries
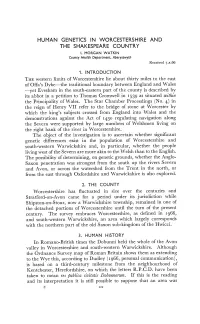
HUMAN GENETICS IN WORCESTERSHIRE AND THE SHAKESPEARE COUNTRY I. MORGAN WATKIN County Health Department, Abet ystwyth Received7.x.66 1.INTRODUCTION THEwestern limits of Worcestershire lie about thirty miles to the east of Offa's Dyke—the traditional boundary between England and Wales —yet Evesham in the south-eastern part of the county is described by its abbot in a petition to Thomas Cromwell in as situated within the Principality of Wales. The Star Chamber Proceedings (No. 4) in the reign of Henry VII refer to the bridge of stone at Worcester by which the king's subjects crossed from England into Wales and the demonstrations against the Act of 1430 regulating navigation along the Severn were supported by large numbers of Welshmen living on the right bank of the river in Worcestershire. The object of the investigation is to ascertain whether significant genetic differences exist in the population of Worcestershire and south-western Warwickshire and, in particular, whether the people living west of the Severn are more akin to the Welsh than to the English. The possibility of determining, on genetic grounds, whether the Anglo- Saxon penetration was strongest from the south up the rivers Severn and Avon, or across the watershed from the Trent in the north, or from the east through Oxfordshire and Warwickshire is also explored. 2. THECOUNTY Worcestershirehas fluctuated in size over the centuries and Stratford-on-Avon came for a period under its jurisdiction while Shipston-on-Stour, now a Warwickshire township, remained in one of the detached portions of Worcestershire until the turn of the present century. -

Nonprofit Law in England & Wales
NONPROFIT LAW IN ENGLAND & WALES Current as of August 2020 This section describes the legal framework governing nonprofit organizations (also known as non-governmental organizations or NGOs) in England & Wales, and includes translations of legislative provisions relevant for a foundation or advisor undertaking an equivalency determination of a foreign grantee under IRS Revenue Procedure 92-94. These reports have been prepared by the International Center for Not-for-Profit Law (ICNL). Please direct corrections and comments to Lily Liu. We include hyperlinks to the following information, to the extent available: • Longer country reports analyzing various aspects of local legislation; and • Texts of local laws that affect the decision whether or not to qualify a grantee (generally in translation, although ICNL and the Council cannot warrant the accuracy of any translation; in addition, legislative excerpts were selected by in-country contacts, and ICNL and the Council cannot warrant that all relevant provisions have been translated). Table of Contents I. Summary A. Types of Organizations B. Tax Laws II. Applicable Laws III. Relevant Legal Forms A. General Legal Forms B. Public Benefit Status IV. Specific Questions Regarding Local Law A. Inurement B. Proprietary Interest C. Dissolution D. Activities E. Political Activities F. Discrimination G. Control of Organization V. Tax Laws A. Tax Exemptions B. Incentives for Philanthropy C. Value Added Tax D. Property Tax E. Other Tax Benefits F. Double Tax Treaty VI. Knowledgeable Contacts I. SUMMARY This report is limited to England and Wales. Scotland and Northern Ireland, the other two components of the United Kingdom, have separate legal systems. In the past, their provisions for regulating charities have differed significantly, but Scotland and Northern Ireland both now have similar regulatory regimes. -
Crime Survey for England and Wales, 2013-2014: Teaching Dataset
UK Data Archive Study Number 7911 - Crime Survey for England and Wales, 2013-2014: Teaching Dataset Crime Survey for England and Wales 2013- 2014: Teaching Dataset User guide Author: Kun Yu, Vanessa Higgins and Jennifer Buckley Version: 2.0 Date: 03 June 2016 1 Contents Background to the Crime Survey for England and Wales (CSEW) 3 Crime Survey for England and Wales (CSEW) 2013-2014 Teaching Dataset 4 How to obtain the CSEW 2013-2014 Teaching Dataset 5 Notes for teachers 5 List of variables in the CSEW 2013-2014 Teaching Dataset 6 Frequencies 10 Code for additional variables 48 2 Background to the Crime Survey for England and Wales (CSEW) The Crime Survey for England and Wales (CSEW) is a face-to-face victimisation survey in which people resident in households in England and Wales are asked about their experiences of a range of crimes in the 12 months prior to the interview. Respondents to the survey are also asked about their perceptions of crime and attitudes towards crime related issues such as the police and criminal justice system. Previously known as the British Crime Survey (BCS), the survey was first conducted in 1982. In 2001, the then BCS, moved to an annual format with continuous sampling. The survey now only covers England and Wales with separate surveys of Scotland and Northern Ireland. However, the first and third surveys were carried out in England, Wales and Scotland (hence ‘British’ Crime Survey). The CSEW uses the Postcode Address File (PAF) to select a representative sample of households in England and Wales. -
Reforming Our Union: Shared Governance in the UK , File Type
Reforming our Union Shared Governance in the UK Securing Wales’ Future | 1 Contents 1 First Minister’s Foreword 1 2 Introduction 2 3 General Principles 4 4 Legislatures and Legislative Powers 7 5 Executive powers: Governments, Agencies and Civil Service 11 6 Finance 16 7 Justice and the Courts 19 8 Constitutional Reform 21 9 Annex 1 – The Twenty Propositions 22 © Crown copyright 2019 WG39096 Digital ISBN: 978-1-83933-324-8 2Mae’r | Reforming ddogfen ymaour Union:hefyd arShared gael yn Governance Gymraeg / in This the documentUK is also available in Welsh 1 First Minister’s Foreword In the public debate around Brexit which has engaged politicians and citizens in all parts of the UK in recent times, the main focus has been on the UK’s future international and trading relations with the European Union and the wider world. This of course is vitally important, but just as much attention needs to be paid to the other side of the coin: how is the UK itself to be governed in future years as it responds to the challenges of the new century, including the potential challenges resulting from Brexit? There is currently a vacuum in the UK Government’s thinking on this issue, at least so far as manifested in public documents. Admittedly, in a speech delivered shortly before she left office, Mrs Theresa May spoke with Mark Drakeford AM commitment about the benefits of the Union. But her speech did not provide First Minister of Wales a way forward for those of us who believe that the United Kingdom continues to have value for each of its constituent parts, that its survival is however an open question, and who wish to see it continue as an effective and mutually-beneficial partnership between people and nations.