Examining Geographical Accessibility to Multi-Tier Hospital Care Services for the Elderly: a Focus on Spatial Equity
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-
SGS-Safeguards 04910- Minimum Wages Increased in Jiangsu -EN-10
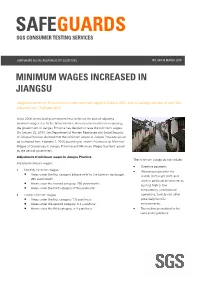
SAFEGUARDS SGS CONSUMER TESTING SERVICES CORPORATE SOCIAL RESPONSIILITY SOLUTIONS NO. 049/10 MARCH 2010 MINIMUM WAGES INCREASED IN JIANGSU Jiangsu becomes the first province to raise minimum wages in China in 2010, with an average increase of over 12% effective from 1 February 2010. Since 2008, many local governments have deferred the plan of adjusting minimum wages due to the financial crisis. As economic results are improving, the government of Jiangsu Province has decided to raise the minimum wages. On January 23, 2010, the Department of Human Resources and Social Security of Jiangsu Province declared that the minimum wages in Jiangsu Province would be increased from February 1, 2010 according to Interim Provisions on Minimum Wages of Enterprises in Jiangsu Province and Minimum Wages Standard issued by the central government. Adjustment of minimum wages in Jiangsu Province The minimum wages do not include: Adjusted minimum wages: • Overtime payment; • Monthly minimum wages: • Allowances given for the Areas under the first category (please refer to the table on next page): middle shift, night shift, and 960 yuan/month; work in particular environments Areas under the second category: 790 yuan/month; such as high or low Areas under the third category: 670 yuan/month temperature, underground • Hourly minimum wages: operations, toxicity and other Areas under the first category: 7.8 yuan/hour; potentially harmful Areas under the second category: 6.4 yuan/hour; environments; Areas under the third category: 5.4 yuan/hour. • The welfare prescribed in the laws and regulations. CORPORATE SOCIAL RESPONSIILITY SOLUTIONS NO. 049/10 MARCH 2010 P.2 Hourly minimum wages are calculated on the basis of the announced monthly minimum wages, taking into account: • The basic pension insurance premiums and the basic medical insurance premiums that shall be paid by the employers. -

Mobile Monitoring of Urban Air Quality at High Spatial Resolution by Low
Mobile monitoring of urban air quality at high spatial resolution by low-cost sensors: Impacts of COVID-19 pandemic lockdown Shibao Wang1, Yun Ma1, Zhongrui Wang1, Lei Wang1, Xuguang Chi1, Aijun Ding1, Mingzhi Yao2, Yunpeng Li2, Qilin Li2, Mengxian Wu3, Ling Zhang3, Yongle Xiao3, Yanxu Zhang1 5 1School of Atmospheric Sciences, Nanjing University, Nanjing, China 2Beijing SPC Environment Protection Tech Company Ltd., Beijing, China 3Hebei Saihero Environmental Protection Hi-tech. Company Ltd., Shijiazhuang, China Correspondence: Yanxu Zhang ([email protected]) Abstract. The development of low-cost sensors and novel calibration algorithms provides new hints to complement 10 conventional ground-based observation sites to evaluate the spatial and temporal distribution of pollutants on hyperlocal scales (tens of meters). Here we use sensors deployed on a taxi fleet to explore the air quality in the road network of Nanjing over the course of a year (Oct. 2019–Sep. 2020). Based on GIS technology, we develop a grid analysis method to obtain 50 m resolution maps of major air pollutants (CO, NO2, and O3). Through hotspots identification analysis, we find three main sources of air pollutants including traffic, industrial emissions, and cooking fumes. We find that CO and NO2 concentrations show a pattern: 15 highways > arterial roads > secondary roads > branch roads > residential streets, reflecting traffic volume. While the O3 concentrations in these five road types are in opposite order due to the titration effect of NOx. Combined the mobile measurements and the stationary stations data, we diagnose that the contribution of traffic-related emissions to CO and NO2 are 42.6 % and 26.3 %, respectively. -

Table of Codes for Each Court of Each Level
Table of Codes for Each Court of Each Level Corresponding Type Chinese Court Region Court Name Administrative Name Code Code Area Supreme People’s Court 最高人民法院 最高法 Higher People's Court of 北京市高级人民 Beijing 京 110000 1 Beijing Municipality 法院 Municipality No. 1 Intermediate People's 北京市第一中级 京 01 2 Court of Beijing Municipality 人民法院 Shijingshan Shijingshan District People’s 北京市石景山区 京 0107 110107 District of Beijing 1 Court of Beijing Municipality 人民法院 Municipality Haidian District of Haidian District People’s 北京市海淀区人 京 0108 110108 Beijing 1 Court of Beijing Municipality 民法院 Municipality Mentougou Mentougou District People’s 北京市门头沟区 京 0109 110109 District of Beijing 1 Court of Beijing Municipality 人民法院 Municipality Changping Changping District People’s 北京市昌平区人 京 0114 110114 District of Beijing 1 Court of Beijing Municipality 民法院 Municipality Yanqing County People’s 延庆县人民法院 京 0229 110229 Yanqing County 1 Court No. 2 Intermediate People's 北京市第二中级 京 02 2 Court of Beijing Municipality 人民法院 Dongcheng Dongcheng District People’s 北京市东城区人 京 0101 110101 District of Beijing 1 Court of Beijing Municipality 民法院 Municipality Xicheng District Xicheng District People’s 北京市西城区人 京 0102 110102 of Beijing 1 Court of Beijing Municipality 民法院 Municipality Fengtai District of Fengtai District People’s 北京市丰台区人 京 0106 110106 Beijing 1 Court of Beijing Municipality 民法院 Municipality 1 Fangshan District Fangshan District People’s 北京市房山区人 京 0111 110111 of Beijing 1 Court of Beijing Municipality 民法院 Municipality Daxing District of Daxing District People’s 北京市大兴区人 京 0115 -

Annual Report 2013 Contents
AMITY A member of Annual Report 2013 Contents 01 A Message from the General Secretary 03 Project Reports 03 Church and Social Services 07 Community Development, Disaster Management, Environmental Protection, HIV/AIDS Prevention and Public Health 11 Education and Orphan Fostering 15 Education and International Exchange 20 Social Welfare 24 NGO Development 28 Urban Community Services 31 Resource Development 34 Amity Foundation, Hong Kong 43 Amity Printing Co., Ltd. 45 Who We Are 45 Organizational Chart 46 Amity Staff 47 Statistics 47 Where the funds come from 47 Where the funds go 48 List of Institutional Partners 55 Auditors Reports 2013 AMITY 01 A Message from the General Secretary In mid-January 2014, the Center for Civil Society Studies of Peking University announced Top Ten Events in Social Sectors in China 2013, among which were direct registration of four types of NGOs as a result of reforming the dual management system, population policy shift from quantity control to structure optimization remarked by the adoption of two-child fertility policy for couples where either the husband or the wife is from a single child family, citizens’ actions urging the government to share the responsibility to address the haze-highlighted environmental problems, Rule of Law in China as a resolution of the 3rd Plenary Session of 18th CPC Central Committee accompanied by a nationwide debate on political and legal basis for China Dream, and smoother cooperation between NGOs and the government occurring during Ya'an earthquake where the emergency response mechanism for disaster relief was challenged. Reading through the Top Ten Events, we find that more and more public voices were heard and taken seriously and eventually became driving forces to social development. -

Transmissibility of Hand, Foot, and Mouth Disease in 97 Counties of Jiangsu Province, China, 2015- 2020
Transmissibility of Hand, Foot, and Mouth Disease in 97 Counties of Jiangsu Province, China, 2015- 2020 Wei Zhang Xiamen University Jia Rui Xiamen University Xiaoqing Cheng Jiangsu Provincial Center for Disease Control and Prevention Bin Deng Xiamen University Hesong Zhang Xiamen University Lijing Huang Xiamen University Lexin Zhang Xiamen University Simiao Zuo Xiamen University Junru Li Xiamen University XingCheng Huang Xiamen University Yanhua Su Xiamen University Benhua Zhao Xiamen University Yan Niu Chinese Center for Disease Control and Prevention, Beijing City, People’s Republic of China Hongwei Li Xiamen University Jian-li Hu Jiangsu Provincial Center for Disease Control and Prevention Tianmu Chen ( [email protected] ) Page 1/30 Xiamen University Research Article Keywords: Hand foot mouth disease, Jiangsu Province, model, transmissibility, effective reproduction number Posted Date: July 30th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-752604/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 2/30 Abstract Background: Hand, foot, and mouth disease (HFMD) has been a serious disease burden in the Asia Pacic region represented by China, and the transmission characteristics of HFMD in regions haven’t been clear. This study calculated the transmissibility of HFMD at county levels in Jiangsu Province, China, analyzed the differences of transmissibility and explored the reasons. Methods: We built susceptible-exposed-infectious-asymptomatic-removed (SEIAR) model for seasonal characteristics of HFMD, estimated effective reproduction number (Reff) by tting the incidence of HFMD in 97 counties of Jiangsu Province from 2015 to 2020, compared incidence rate and transmissibility in different counties by non -parametric test, rapid cluster analysis and rank-sum ratio. -

Risk Assessment of Urban Rainstorm Disaster Based on Multi-Layer Weighted Principal Component Analysis: a Case Study of Nanjing, China
International Journal of Environmental Research and Public Health Article Risk Assessment of Urban Rainstorm Disaster Based on Multi-Layer Weighted Principal Component Analysis: A Case Study of Nanjing, China Junfei Chen 1,2,3,* , Juan Ji 1, Huimin Wang 1,4, Menghua Deng 1 and Cong Yu 1 1 Business School, Hohai University, Nanjing 211100, China; [email protected] (J.J.); [email protected] (H.W.); [email protected] (M.D.); [email protected] (C.Y.) 2 Yangtze Institute for Conservation and Development, Hohai University, Nanjing 210098, China 3 Research Institute of Jiangsu Yangtze River Conservation and High-Quality Development, Nanjing 210098, China 4 State Key Laboratory of Hydrology-Water Resources and Hydraulic Engineering, Hohai University, Nanjing 210098, China * Correspondence: [email protected]; Tel.: +86-25-6851-4613 Received: 26 June 2020; Accepted: 29 July 2020; Published: 30 July 2020 Abstract: Nanjing city is taken as a case in this urban rainstorm disaster risk research. Using the data of meteorology and social-economy statistics of Nanjing area, the paper selected ten indicators to establish the risk assessment system of urban rainstorm disaster from the aspects of the vulnerability of hazard-affected body, the fragility of disaster-pregnant environment, and the danger of hazard factors. Multi-layer weighted principal component analysis (MLWPCA) is an extension of the principal component analysis (PCA). The MLWPCA is based on factor analysis for the division subsystem. Then the PCA is used to analyze the indicators in each subsystem and weighted to synthesize. ArcGIS is used to describe regional differences in the urban rainstorm disaster risk. -

View’, Procedia-Social and Growth of That Area
Avestia Publishing International Journal of Civil Infrastructure (IJCI) Volume 3, Year 2020 ISSN: 2563-8084 DOI: 10.11159/ijci.2020.004 Spatial Differentiation and Influencing Factors of Attended Collection and Delivery Points in Nanjing City, China Muhammad Sajid Mehmood1,2, Gang Li1,2*, Shuyan Xue1,2, Qifan Nie3, Xueyao Ma1,2, Zeeshan Zafar1,2, Adnan Rayit4 1College of Urban and Environmental Sciences, Northwest University Xi’an 710127, China 2Shaanxi Key Laboratory of Earth Surface System and Environmental Carrying Capacity, Northwest University Xi’an 710127, China *[email protected] 3Department of Civil, Construction and Environmental Engineering, University of Alabama System, Tuscaloosa 35401, USA 4Agricultural Information Institute, Graduate School Chinese Academy of Agricultural Sciences, Haidian District, Beijing 100093, China Keywords: Attended collection and delivery points, China Abstract - E-commerce and online shopping have become more Post stations, Cainiao stations, spatial pattern, convenient due to the rapid growth of the internet logistic influencing factors, Nanjing City. industry in many developed countries and is particularly popular and suitable in China. The method is primarily based on © Copyright 2020 Authors - This is an Open Access article logistic points like attended collection and delivery points published under the Creative Commons Attribution (ACDPs), an emerging industry for economic development. This License terms (http://creativecommons.org/licenses/by/3.0). article includes text analysis, descriptive statistics, and spatial Unrestricted use, distribution, and reproduction in any medium analysis to analyze the operation types, service objects, location are permitted, provided the original work is properly cited. distribution, and influencing factors of ACDPs in Nanjing City using point of interest data (POI) of Cainiao stations and China Post stations. -

H2 AN201203050005010565 1.Pdf
Wuxi Little Swan Company Limited Annual Report 2011 Contents Important Notes-------------------------------------------------------------------------------------------------0 I. Company Profile-----------------------------------------------------------------------1 II. Summary of Accounting Highlights and business Highlights-------------------------------------- 3 III. Changes in Share Capital and Particulars about Shareholders------------------5 IV. Directors, Supervisors, Senior Management Staff and Employees-------------11 V. Corporate Governance--------------------------------------------------------------------15 VI. Particulars about Establishment and Accomplishment of Internal Control------------------19 VII. Brief Introduction to Shareholders’ General Meetings-------------------------------23 VIII. Report of the Board of Directors-----------------------------------------------------24 IX. Report of the Board of Supervisors-------------------------------------------------35 X. Significant Events-------------------------------------------------------------------------37 XI. Financial Report----------------------------------------------------------------------------46 XII. Documents Available for Reference-----------------------------------------------------------------131 Wuxi Little Swan Company Limited Annual Report 2011 Important Notes The Board of Directors, the Board of Supervisors as well as all directors, supervisors and senior management staffs of Wuxi Little Swan Company Limited (hereinafter referred to as “the Company”) -

HCP REPORT NO. 1: the URBAN FOOD SYSTEM of NANJING, CHINA Si, Zhenzhong;Crush, Jonathan;Scott, Stephanie;Zhong, Tiyang; ;
HCP REPORT NO. 1: THE URBAN FOOD SYSTEM OF NANJING, CHINA Si, Zhenzhong;Crush, Jonathan;Scott, Stephanie;Zhong, Tiyang; ; © 2018, HUNGRY CITIES PARTNERSHIP This work is licensed under the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/legalcode), which permits unrestricted use, distribution, and reproduction, provided the original work is properly credited. Cette œuvre est mise à disposition selon les termes de la licence Creative Commons Attribution (https://creativecommons.org/licenses/by/4.0/legalcode), qui permet l’utilisation, la distribution et la reproduction sans restriction, pourvu que le mérite de la création originale soit adéquatement reconnu. IDRC Grant/ Subvention du CRDI: 107775-001-Hungry Cities Initiative: Informality, Inclusive Growth, and Food Security in Cities of the Global South HUNGRY CITIES PARTNERSHIP T!" U#$%& F''( S)*+", '- N%&./&0, C!/&% HUNGRY CITIES REPORT NO. 1 HUNGRY CITIES PARTNERSHIP THE URBAN FOOD SYSTEM OF NANJING, CHINA ZHENZHONG SI WITH JONATHAN CRUSH, STEFFANIE SCOTT AND TAIYANG ZHONG SERIES EDITOR: PROF. JONATHAN CRUSH HUNGRY CITIES REPORT NO. 1 ACKNOWLEDGEMENTS The research and publication of this report was funded by the Social Sciences and Humanities Research Council (SSHRC) and the Interna- tional Development Research Centre (IDRC) under the International Partnerships for Sustainable Societies (IPaSS) Program. © HUNGRY CITIES PARTNERSHIP 2016 Published by the Hungry Cities Partnership African Centre for Cities, University of Cape Town, South Africa, and Wilfrid Laurier University/Balsillie School of International Affairs, Waterloo, Canada First published 2016 ISBN 978-1-920597-16-0 Cover photo: Zhenzhong Si Production by Bronwen Dachs Muller, Cape Town All rights reserved. No part of this publication may be reproduced or transmitted, in any form or by any means, without prior permission from the publishers. -

List of the Recommended Hotels for Nanjing 2017 World Roller Games 0331
List of the Recommended Hotels for Nanjing 2017 World Roller Games 0331 Number of Number of Single Hotel Name Star Price (RMB) Price (RMB)Contact Official Website Booking Email Address Note Twin Rooms Rooms The other Hilton named ' Hilton River Side' 800 (including breakfast 800 (Breakfast was the venue of the last FIRS Congress, it is 1 Hilton Nanjing 5 75 75 MIAO Tingting 18805140811 nangjing.hilton.com [email protected] No.100 Jiangdong Middle Road, Nanjing for two) included) not included in the list due it is the appointed headquarter hotel for the WRG. 700 (including breakfast 768 (Breakfast 2 Han Yue Lou Hotel 5 43 155 SUN Chao 13913019399 [email protected] No.235 Jiangdong Middle Road, Nanjing for two) included) Nanjing Jinling 658 (including breakfast 658 (Breakfast No.8 Wanjingyuan Road, Yangzijiang 3 Riverside Conference Quasi-5 50 80 ZHANG Yu 15195847019 www.jinlinghotels.com [email protected] for two) included) Avenue, Nanjing Hotel 376 (including breakfast 550 (Breakfast 4 New Town Hotel Quasi-4 88 40 LUO Yanlong 18626411163 www.newtown-hotel.com [email protected] No.67 Aoti Avenue, Jianye District, Nanjing for two) included) 400 (including breakfast 428 (Breakfast No.188 Jiangdong Middle Road, Jianye 5 Zhenbao Holiday Hotel Quasi-5 90 40 SUN Zijun 13913920469 www.zbhhotel.cn [email protected] for two) included) District, Nanjing Jiangsu Trade 400 (including breakfast 550 (Breakfast No.289 Jiangdong Middle Road, Jianye 6 Quasi-5 100 40 Jiang Jie 13913901683 [email protected]. International Hotel for two) -

Types of Community Health Services Selected by Urban and Suburban Residents in Nanjing and Influencing Factors
Fam Med Com Health: first published as 10.15212/FMCH.2014.0105 on 1 March 2014. Downloaded from Family Medicine and Community Health ORIGINAL ORIGINAL RESEARCH ORIGINAL RESEARCH Types of community health services selected by urban and suburban residents in Nanjing and influencing factors Hong Fan, Qianyuan Wang, Yinyan Wu Abstract Social and Health Education Objective: The purpose of the current study was to determine the types of community health Department, School of Public services selected by urban and suburban residents in Nanjing and the influencing factors in an ef- Health, Nanjing Medical Uni- fort to improve the community health services to better meet the residents’ demands. versity, Nanjing City, Jiangsu Methods: Between 15 May 2013 and 15 June 2013, eight community health service centers Province 210029 from four districts in Nanjing (Gulou District and Baixia District in urban areas and Jiangning CORRESPONDING AUTHOR: District and Pukou District in suburban areas; two centers from each district) were selected using Hong Fan a stratified random sampling method of investigation sites. After an intercept interview with 487 Social and Health Education community residents, univariate and multivariate analyses were performed by means of logistic Department, School of Public regression. Health, Nanjing Medical Results: Among the 487 users of community health services, there were 241 residents from University, Nanjing City, Jiangsu urban areas (49.5%) and 246 residents from suburban areas (50.5%). Among the respondents, Province 210029 there were 191 (39.2%) who usually received medical treatment from community health service E-mail: [email protected] institutions, including 74 (38.7%) from urban areas and 117 (61.3%) from suburban areas. -
Sanctioned Entities Name of Firm & Address Date of Imposition of Sanction Sanction Imposed Grounds China Railway Constructio
Sanctioned Entities Name of Firm & Address Date of Imposition of Sanction Sanction Imposed Grounds China Railway Construction Corporation Limited Procurement Guidelines, (中国铁建股份有限公司)*38 March 4, 2020 - March 3, 2022 Conditional Non-debarment 1.16(a)(ii) No. 40, Fuxing Road, Beijing 100855, China China Railway 23rd Bureau Group Co., Ltd. Procurement Guidelines, (中铁二十三局集团有限公司)*38 March 4, 2020 - March 3, 2022 Conditional Non-debarment 1.16(a)(ii) No. 40, Fuxing Road, Beijing 100855, China China Railway Construction Corporation (International) Limited Procurement Guidelines, March 4, 2020 - March 3, 2022 Conditional Non-debarment (中国铁建国际集团有限公司)*38 1.16(a)(ii) No. 40, Fuxing Road, Beijing 100855, China *38 This sanction is the result of a Settlement Agreement. China Railway Construction Corporation Ltd. (“CRCC”) and its wholly-owned subsidiaries, China Railway 23rd Bureau Group Co., Ltd. (“CR23”) and China Railway Construction Corporation (International) Limited (“CRCC International”), are debarred for 9 months, to be followed by a 24- month period of conditional non-debarment. This period of sanction extends to all affiliates that CRCC, CR23, and/or CRCC International directly or indirectly control, with the exception of China Railway 20th Bureau Group Co. and its controlled affiliates, which are exempted. If, at the end of the period of sanction, CRCC, CR23, CRCC International, and their affiliates have (a) met the corporate compliance conditions to the satisfaction of the Bank’s Integrity Compliance Officer (ICO); (b) fully cooperated with the Bank; and (c) otherwise complied fully with the terms and conditions of the Settlement Agreement, then they will be released from conditional non-debarment. If they do not meet these obligations by the end of the period of sanction, their conditional non-debarment will automatically convert to debarment with conditional release until the obligations are met.