Community Health Improvement Plan 2019-2021
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Health Care Strategic Planning
HEALTH Introducing CARE STRATEGIC . PLANNING ACCORD LIMITED HEALTH CARE STRATEGIC PLANNING 1 ACCORD LIMITED HEALTH CARE STRATEGIC PLANNING TABLE OF CONTENTS Introduction to ACCORD LIMITED ......................................................... 3 StrategicSTRATEGIC Planning PLANNING ................................ .................................................................................................................... 4 ACCORD’s’s Approach APPROACH ................................ ................................................................................................................... 6 WhatWHAT Differentiates DIFFERENTIATES ACCORD ................................ACCORD ............................................................................... 13 A PromisePROMISE to TOour ClientsOUR CLIENTS ................................ .............................................................................................. 14 ACCORD’s’s Other OTHER Services SERVICES ................................ ................................................................................................. 15 ACCORD’s’s Health HEALTH Care CARE Clients CLIENTS ................................ ........................................................................... 16 ACCORD’s’s Consulting CONSULTING Team ................................TEAM ...................................................................................... 2220 2 ACCORD LIMITED HEALTH CARE STRATEGIC PLANNING GENERAL INFORMATION ACCORD LIMITED (ACCORD) is -

2005 Most Wired Survey and Benchmarking Study
2012 Most Wired Survey Winners by State Alabama Cullman Regional Medical Center: Innovator Award winner Evergreen Medical Center: Most Wired–Small and Rural St. Vincent’s Hospital–Birmingham: Most Wired University of Alabama at Birmingham (UAB) Hospital: Most Wired Washington County Hospital, Chatom: Most Wired–Small and Rural Arizona Banner Health, Phoenix: Most Wired Tucson Medical Center: Most Wired Arkansas Stone County Medical Center, Mountain View: Most Wired–Small and Rural California Eisenhower Medical Center, Rancho Mirage: Most Wired Kaiser Permanente, Oakland: Most Improved Naval Hospital Lemoore: Most Wired–Small and Rural Rady Children's Hospital–San Diego: Most Wired San Francisco VA Medical Center: Most Wired Sharp HealthCare, San Diego: Most Wired Stanford Hospital and Clinics: Most Wired University of California Davis Health System, Sacramento: Most Wired University of California, San Diego Health System: Most Wired VA Palo Alto Health Care System: Most Wired VA Sierra Pacific Network, Mare Island: Most Wired Colorado Denver Health and Hospital Authority: Most Wired Poudre Valley Health System, Fort Collins: Most Wired Connecticut Hartford Hospital: Most Wired Middlesex Health System, Middletown: Most Wired MidState Medical Center, Meriden: Most Wired Saint Francis Care, Hartford: Most Wired William W. Backus Hospital, Norwich: Most Wired Yale New Haven Health System: Most Wired Delaware Alfred I. duPont Hospital for Children, Wilmington: Most Wired District of Columbia Washington, D.C. VA Medical Center: Most Wired Florida -
Participants List Through January 2020
REGIONAL GROUP NAME CITY STATE CENTER HEALTH SYSTEM(s) CANADIAN VASCULAR QUALITY INITIATIVE Montreal, QC Canada CHUM CANADIAN VASCULAR QUALITY INITIATIVE Gatineau Canada CISSSO CANADIAN VASCULAR QUALITY INITIATIVE Edmonton, AB Canada Covenant Health - Grey Nuns Hospital CANADIAN VASCULAR QUALITY INITIATIVE Kentville, Nova Scotia Canada Nova Scotia Health Authority CANADIAN VASCULAR QUALITY INITIATIVE Toronto, Ontario Canada Sunnybrook Health Sciences Centre CANADIAN VASCULAR QUALITY INITIATIVE Thunder Bay Canada Thunder Bay ReGional Health Sciences Centre CANADIAN VASCULAR QUALITY INITIATIVE Toronto Canada Toronto General Hospital CAROLINAS VASCULAR QUALITY GROUP (CVQG) BurlinGton NC Alamance ReGional Medical Center Cone Health System; Carolinas Healthcare CAROLINAS VASCULAR QUALITY GROUP (CVQG) Anderson SC AnMed Health Medical Center (AnMed Health) CAROLINAS VASCULAR QUALITY GROUP (CVQG) Concord NC Atrium Health Carrabus The Charlotte-MecklenburG Hospital Authority d/b/a Atrium Health CAROLINAS VASCULAR QUALITY GROUP (CVQG) Charlotte NC Atrium Health Pineville The Charlotte-MecklenburG Hospital Authority d/b/a Atrium Health CAROLINAS VASCULAR QUALITY GROUP (CVQG) Monroe NC Atrium Health Union The Charlotte-MecklenburG Hospital Authority d/b/a Atrium Health CAROLINAS VASCULAR QUALITY GROUP (CVQG) louidiana SC Beaufort Memorial Hospital CAROLINAS VASCULAR QUALITY GROUP (CVQG) Hickory NC Catawba Valley Medical Center CAROLINAS VASCULAR QUALITY GROUP (CVQG) Greensboro NC Cone Health Heart & Vascular Center Cone Health System; Carolinas Healthcare -

Notice of Privacy Practices Introduction Research
NOTICE OF PRIVACY PRACTICES INTRODUCTION RESEARCH. Under certain circumstances, we may use or disclose your health information for research, THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND subject to certain safeguards. We may disclose health information about you to people preparing to conduct DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT a research project, but the information will stay on site. APPENDIX A: APPENDIX C: CAREFULLY. THREATS TO HEALTH OR SAFETY. Under certain circumstances, we may use or disclose your health We are required by law to maintain the privacy of your health information and to give you our Notice of Privacy information to prevent a serious and imminent threat to health and safety. In addition to the privacy protections afforded to all medical records Individuals Involved in Your Care. Depending on your age and UnityPoint Health participates in one or more Organized UnityPoint Health-Meriter, Iowa Physicians Clinic Medical under HIPAA, the confidentiality of substance use disorder records mental capacity and the location of your services, we may be permitted Health Care Arrangements (“OHCAs”). OHCAs can take one Foundation (UPC), UnityPoint at Home participate in an Practices (this “Notice”) that describes our privacy practices, legal duties and your rights concerning your SPECIALIZED GOVERNMENT FUNCTIONS. We may use and disclose your health information for are protected by another federal law referred to as Part 2. Certain to make certain disclosures of your information to your guardian, for of two forms. First, an OHCA can be a clinically integrated OHCA with University of Wisconsin Hospitals and Clinics health information. -

Opportunities Directory 2018-2019 W Family Medicine a Emergency Medicine IOWA Opportunities Directory
I Opportunities Directory 2018-2019 W Family Medicine A Emergency Medicine IOWA Opportunities Directory Family Medicine Emergency Medicine 2018-2019 Office of Statewide Clinical Education Programs The University of Iowa Roy J. and Lucille A. Carver College of Medicine 2133 ML Iowa City, Iowa 52242 Phone: (319) 335-8618 Fax: (319) 335-8034 E-mail: [email protected] Website: http://www.medicine.uiowa.edu/oscep/opportunities/ Table of Contents Data Collection Methods ................................................................. i Physician Consultation Services ...................................................... i How to Use the Directory ............................................................... ii Family Medicine Opportunities................................................................................. 1 Statewide Summary .................................................................... 23 List of Communities by Opportunity Type ..................... 24 Map of Communities ...................................................... 25 List of Communities by Geographic Region .................. 26 Summary of Practice Opportunities ................................ 27 Emergency Medicine Opportunities............................................................................... 28 Statewide Summary .................................................................... 37 List of Communities ....................................................... 38 Map of Communities ...................................................... 38 -
System Profile &
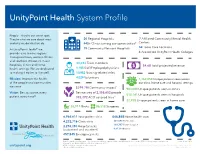
UnityPoint Health System Profile People — they’re our sweet spot. They’re what we care about most 20 Regional Hospitals 7 Affiliated Community Mental Health and why we do what we do. 440+ Clinics serving our communities# Centers 14 Home Care Locations At UnityPoint Health® we 19 Community Network Hospitals provide care in nine regions 4 Accredited UnityPoint Health Colleges throughout Iowa, western Illinois and southern Wisconsin in our 33,034 Team members hospitals, clinics and home $4.6B Total projected revenue health settings. We are dedicated 1,185 Staff/Employed physicians to making it easier to live well. 10,982 Nursing-related roles 4,029 Volunteers Mission: Improve the health 1,162,058 Unique patients seen across of the people and communities our clinic, home care and hospital settings we serve * $299.7M Community impact 983,088 Unique patients seen in clinics Vision: Best outcome, every Service area of 2,358,652 people 510,141 Unique patients seen in hospitals patient, every time® 392,372 ACO covered lives+* 22,928 Unique patients seen in home care 20,911 Births 86,518 Surgeries 6,966,611 Total patient visits 446,848 Home health visits 4,232,716 Clinic visits 301,498 Home care 138,737 Home hospice 2,276,350 Hospital visits (outpatient and inpatient) 6,613 Pediatrics 457,545 Emergency visits Statistics, outside of facility counts and team members which are updated at time of publishing, are based on the 2020 calendar year unless noted below. Updated June 2021 + Doesn’t include Medicaid MCOs or Medicare Advantage ACOs unitypoint.org # Clinic is defined as a physical address and suite. -

Physical Medicine and Rehabilitation Annual Report 2012
Physical Medicine and Rehabilitation Annual Report 2012 Genesis Health System exists to provide compassionate, quality health service to all those in need. Table of Contents Introduction 3 Inpatients Served 4 Inpatient Program Discharge Data 5 Day Rehabilitation 6 Brain Injury Program-Inpatient 7 Earning Recognition for Brain Injury Programs 8 Brain Injury Program-Outpatient 9 Constraint Induced Movement Therapy 10 Spinal Cord System of Care - Inpatient 11 Spinal Cord System of Care - Outpatient 12 Professional Development Program 13 GOPEDS-Pediatric Program 14 Outpatient Service Locations 15 Power Sports Performance 16 Medical Services 17 New Program - Concussion Management 18 New Program - Wheelchair Clinic 19 Awards/Certifications 20 2 Introduction The Genesis Physical Medicine and Rehabilitation Service Line continues to offer the largest and most complete inpatient rehabilitation program in the State of Iowa. The only CARF accredited Outpatient Brain Injury Program and Spinal Cord System of Care Program is offered at Genesis. In addition, the Inpatient Brain Injury Program is one of only two CARF accredited programs in the State to offer services to adult, adolescent and pediatric patients who have experienced a brain injury. During FY 2012, referrals to the inpatient program increased by nearly seven percent with the majority of the increase coming from outside referral sources such as the University of Iowa. Our Outpatient Pediatric Program, “Go Peds”, saw a 32% increase as compared to the previous year. These continued increases year after year, attest to the fact that the Genesis physical medicine and rehabilitation programs are highly valued. Reflecting back on FY 2012 we see many improvements to our programs. -

Mqii Stakeholders and Collaborators
MQii Stakeholders and Collaborators The Malnutrition Quality Improvement Initiative (MQii) is a project of the Academy of Nutrition and Dietetics, Avalere Health, and other stakeholders who provided guidance and expertise through a collaborative partnership. Support for the MQii is provided by Abbott. Special thanks to the members of the MQii Advisory Committee for their guidance in designing and informing the content of the Toolkit; to the members of the Technical Expert Panel for their guidance in specifying and testing the malnutrition electronic clinical quality measures (eCQMs); and to the members of the MQii Learning Collaborative for their work to implement the MQii Toolkit and eCQMs, and provide feedback to inform revisions and future iterations to MQii tools. MQii Advisory Committee Members Al Barrocas, MD, FACS, FASPEN Bob Blancato, MPA Owner of Alma, LLC President Fellow and Co-Chair of ASPEN’s Value Project Matz, Blancato and Associates (Former Chief Medical Officer of WellStar Atlanta (Former Chair of American Society on Aging, Director of Medical Center, Clinical Professor in the Surgery National Association of Nutrition and Aging Services Departments of LSU and Tulane Schools of Medicine) Programs, and board member for AARP) Member: 2020–Present Member: 2020–Present Charley John, PharmD Leslie Kelly-Hall Director of U.S. Public Policy Founder of Engaging Patient Strategy, Senior Vice Walgreens President of Policy Member of Government Affairs Committee at National Healthwise Association of Specialty Pharmacy Member: 2014–Present -

SOC Telemed Expands Partnership with Unitypoint Health to Scale Telemedicine Solution and Increase Access to Behavioral Health S
SOC Telemed Expands Partnership with UnityPoint Health to Scale Telemedicine Solution and Increase Access to Behavioral Health Specialists Multi-site expansion of Telemed IQ acute telemedicine platform and clinical services Reston, VA – August 3, 2021 – SOC Telemed (NASDAQ: TLMD), the largest national provider of acute care telemedicine, today announced an expansion of its partnership with UnityPoint Health from three hospitals to an additional four hospitals across two markets. Based on the success over the past three years working with SOC Telemed, UnityPoint Health is expanding its telePsychiatry services, adding the Telemed IQ telemedicine platform and SOC- provided psychiatrists to four additional hospitals. In Des Moines, Iowa, additional hospitals include Iowa Methodist Medical, Iowa Lutheran Hospital and Methodist West Hospital. In Cedar Rapids, Iowa, it includes St. Luke’s Hospital. SOC Telemed will go live with telePsychiatry services for UnityPoint Health in the second half of 2021 in both markets. SOC Telemed’s relationship with UnityPoint Health began in 2018 at Allen Hospital, a not-for- profit community hospital located in Waterloo, Iowa. The facility used Telemed IQ, SOC Telemed’s telemedicine platform, to drive their enterprise telePsychiatry solution, resulting in improved psychiatric care, including reduced length of stay, improved throughput in the emergency department and a substantial ROI for the hospital. “Our successful partnership with SOC Telemed at Allen Hospital showed that we could help alleviate the stress placed on our other facilities,” said Calvin Heller, Director, Telehealth, UnityPoint Health. “SOC Telemed is a helpful morale booster to our doctors and nurses while also providing best-in-class care for our patients.” Prior to implementing SOC Telemed’s enterprise solution, Allen Hospital had one full-time psychiatrist staffing its 21-bed behavioral health unit. -

Genesis Health System 2014 Audit Report
Genesis Health System and Related Organizations Consolidated Financial Report June 30, 2014 Contents Independent Auditor's Report 1 – 2 Financial Statements Consolidated balance sheets 3 – 4 Consolidated statements of operations 5 Consolidated statements of changes in net assets 6 Consolidated statements of cash flows 7 – 8 Notes to consolidated financial statements 9 – 41 Independent Auditor’s Report To the Audit and Compliance Committee Genesis Health System Davenport, Iowa Report on the Financial Statements We have audited the accompanying consolidated financial statements of Genesis Health System and related organizations (System) which comprise the consolidated balance sheets as of June 30, 2014 and 2013, and the related consolidated statements of operations, changes in net assets and cash flows for the years then ended and the related notes to the consolidated financial statements. Management’s Responsibility for the Financial Statements Management is responsible for the preparation and fair presentation of these consolidated financial statements in accordance with accounting principles generally accepted in the United States of America; this includes the design, implementation, and maintenance of internal control relevant to the preparation and fair presentation of consolidated financial statements that are free from material misstatement, whether due to fraud or error. Auditor’s Responsibility Our responsibility is to express an opinion on these consolidated financial statements based on our audits. We did not audit the financial statements of Misericordia Assurance Company, Ltd., a consolidated subsidiary, which statements reflect total assets constituting approximately 3% and 4%, respectively, of the related consolidated total assets as of June 30, 2014 and 2013, and total revenue constituting approximately 1% of consolidated total revenue for each of the years then ended. -

The Valued Voice, September 10, 2019
37 , Issue THE VALUED VOICE 3 Vol 6 Vol September 10, 2019 IN THIS ISSUE Grassroots Spotlight Grassroots Spotlight: WHA Talks WHA Talks Surprise Billing with Congressman Surprise Billing with Congressman Steil at Mercyhealth - Walworth .............. 1 Steil at Mercyhealth - Walworth The Wisconsin Hospital Association met with DHS Announces Second Round of APC, Congressman Bryan Steil of Wisconsin’s 1st Allied Health Grants ......................... 1 Congressional District for a health care roundtable Grant Funds will Enhance Perinatal discussion September 6. Care .................................................. 2 The event was hosted at Mercyhealth Hospital and Medical Center-Walworth in Lake Geneva. WHA Director of Federal and State Relations Jon Hoelter kicked Wisconsin Hospitals State PAC & off the discussion with some background on issues important to WHA and its Conduit 2019 Campaign Update ...... 2 members. Hoelter stressed the importance of adequate reimbursement under September is Prostate Cancer Medicare, noting that while Wisconsin hospitals are known for delivering some Awareness Month ............................ 2 of the best health care in the country, they receive on average only 75 cents on the dollar for treating Medicare patients. This is particularly challenging in Wisconsin, where hospitals receive significantly lower Medicare reimbursement than most states. The group also discussed concerns about recent issues making it more difficult for hospitals to serve their communities, such as site-neutral payments. Hospitals -

Unitypoint Health® – Des Moines Overview
UnityPoint Health® – Des Moines Overview UnityPoint Health – Des Moines is committed to surrounding you with care — at your doctor’s office, in the hospital or at home. Our family includes four hospitals: Iowa Methodist Medical Center, Iowa Lutheran Hospital, Methodist West Hospital and Blank Children’s Hospital; our John Stoddard Cancer Center; more than 50 UnityPoint Clinic® locations; UnityPoint at HomeSM; and UnityPoint HospiceSM. Our team of health care professionals work together to coordinate high-quality, compassionate health care services right here in Central Iowa. And we are proud to be part of UnityPoint Health, which provides care throughout Iowa, Illinois and Wisconsin through more than 280 clinics, 29 hospitals in metropolitan and rural communities and home care services throughout its regions. UnityPoint Health – Des Moines at a Glance 887 5,010 22,425 101,980 918 BIRTHS SURGERIES EMERGENCY VISITS PHYSICIANS VOLUNTEERS 7,797 LICENSED BEDS 33,225 1.3 million EMPLOYEES 801 ADMISSIONS OUTPATIENT VISITS UnityPoint Health – Des Moines Iowa Methodist Medical Center Iowa Methodist Medical Center was established in 1901 and is known as an important regional medical center, teaching hospital and Level 1 Trauma Center. Iowa Methodist specializes in emergency and trauma treatment, cancer treatment, cardiovascular care, kidney transplant, surgery, maternity and women’s services, YounkerPHYSICIANS Rehabilitation Center, and orthopaedics. Iowa Lutheran Hospital Since 1914 Lutheran Hospital has a history of serving the Des Moines community and Central Iowa with a patient-centered, caring atmosphere. The hospital specializes in maternity services, emergency care, chemical dependency treatment, behavioral health, general surgery, critical care, cardiovascular care, and transitional care services.