Nichols College Incomer's Checklist
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
FINAL August 15 2017-18 D2-3 All Academic Team.Xlsx
Name Year Position School Hometown Commonwealth Coast Conference Becker Ryan Clifford Freshman Goaltender Becker College Coventry, Rhode Island MacGregor Howey Senior Forward Becker College Grosse Ile, Michigan Connor Jones Junior Forward Becker College Lake Placid, New York Nikolas Nasby Senior Defenseman Becker College Newberg, Oregon Corey Schafer Junior Forward Becker College Johnstown, Pennsylvania James Wallace Senior Forward Becker College Levittown, Pennsylvania Curry Frank Cundiff Freshman Goaltender Curry College Oceanside, New York Joe DiBenedetto Sophomore Forward Curry College Anchorage, Alaska Zoltan Eross Freshman Forward Curry College Budapest, Hungary Ryan Fitzgerald Senior Forward Curry College Cary, North Carolina Mack Heisinger Junior Defenseman Curry College Winnipeg, Manitoba Viktor Jansson Freshman Forward Curry College Stockholm, Sweden Phil Kiss Senior Defenseman Curry College Burlington, Ontario Kasper Kjellkvist Freshman Forward Curry College Vaxjo, Sweden Jarret Kup Senior Defenseman Curry College Rosseau, Ontario Tyler Lindstrom Freshman Defenseman Curry College Brooklyn Park, Minnesota Lio Mauron Junior Forward Curry College Lausanne, Switzerland Alec Mono Sophomore Defenseman Curry College Las Vegas, Nevada Tristan Morin Freshman Forward Curry College Unionville, Connecticut Shane Tracy Senior Forward Curry College Bow, New Hampshire Anthony Trujillo Sophomore Forward Curry College Toronto, Ontario Jordan Williamson Sophomore Forward/DefeCurry College Okotoks, Alberta Endicott Josh Bowes Junior Forward Endicott -

UNH CF American College Dublin American International College
UNH CF American College Dublin American International College American University Anna Maria College Assumption College Bay Path University Becker College Bennington College Bishop's University Bridgewater State University Bryant University Castleton University Central Maine Community College Champlain College Clarkson University Colby-Sawyer College Colorado State University Curry College Dean College Dickinson College Drew University Eastern Maine Community & Technical College Eckerd College Elizabethtown College Elmira College Elms College Emmanuel College Endicott College Fitchburg State University Florida Atlantic University Florida Institute of Technology Florida Southern College Franklin Pierce University George Mason University Goddard College Goucher College Hampshire College Hartwick College Hobart and William Smith Colleges Hofstra University Husson University Ithaca College Johnson & Wales University Juniata College Keene State College Lakes Region Community College Lasell College Lesley University Liberty University Lynn University Maine College of Health Professions Manchester Community College Manhattan College Manhattanville College Marist College Marymount Manhattan College McGill University Messiah College Montserrat College of Art Mount Allison University Mount Holyoke College Mount Ida College N.H. National Guard N.H. National Guard Nashua Community College New England College New England Institute of Technology New England School of Photography New Hampshire Institute of Art Newbury College Nichols College Northern -

Member Colleges
SAGE Scholars, Inc. 21 South 12th St., 9th Floor Philadelphia, PA 19107 voice 215-564-9930 fax 215-564-9934 [email protected] Member Colleges Alabama Illinois Kentucky (continued) Missouri (continued) Birmingham Southern College Benedictine University Georgetown College Lindenwood University Faulkner Univeristy Bradley University Lindsey Wilson College Missouri Baptist University Huntingdon College Concordia University Chicago University of the Cumberlands Missouri Valley College Spring Hill College DePaul University Louisiana William Jewell College Arizona Dominican University Loyola University New Orleans Montana Benedictine University at Mesa Elmhurst College Maine Carroll College Embry-Riddle Aeronautical Univ. Greenville College College of the Atlantic Rocky Mountain College Prescott College Illinois Institute of Technology Thomas College Nebraska Arkansas Judson University Unity College Creighton University Harding University Lake Forest College Maryland Hastings College John Brown University Lewis University Hood College Midland Lutheran College Lyon College Lincoln College Lancaster Bible College (Lanham) Nebraska Wesleyan University Ouachita Baptist University McKendree University Maryland Institute College of Art York College University of the Ozarks Millikin University Mount St. Mary’s University Nevada North Central College California Massachusetts Sierra Nevada College Olivet Nazarene University Alliant International University Anna Maria College New Hampshire Quincy University California College of the Arts Clark University -

Course Catalog | Nichols College
2015–2017 CATALOG This publication provides information concerning the programs at Nichols College and does not constitute a contract with the student. The policies and procedures contained in the 2015-2017 Nichols College Catalog will remain in effect until June 30, 2017. Nichols College reserves the right to change at any time the rules governing admission, tuition, fees, courses, the granting of degrees, or any other regulations affecting the campus community. Such changes are to take effect whenever College officials deem necessary. NICHOLS COLLEGE Center Road P.O. Box 5000 Dudley, Massachusetts 01571-5000 Catalog of Nichols College July 2015 Volume XLVII President’s Message Dear Student, Within a supportive community, Nichols College transforms today’s students into tomorrow’s leaders through a dynamic, career-focused business and professional education. This mission guides all of our efforts and ensures that our students benefit from a range of curricular and co-curricular opportunities that give them a distinct advantage in the workplace. Our faculty, many of whom are former business leaders, executives and owners, bring a unique perspective to the classroom and continually work to develop teaching methods that promote a meaningful educational experience. Programs such as the Professional Development Seminar, a four-year series of one-credit courses designed to enhance the professional and personal development of students beyond academics, 1 have become the cornerstone of a Nichols education. Nichols is steadily defining leadership education for the next generation of students. Every day, we dedicate ourselves to their professional development and they amaze us with their capacity to discover their own leadership potential. -

Nautilus, Vol. 35 No. 6 (May 1982)
Salve Regina University Digital Commons @ Salve Regina Student Newspapers Archives and Special Collections 4-1-1982 Nautilus, Vol. 35 No. 6 (May 1982) Salve Regina College Follow this and additional works at: https://digitalcommons.salve.edu/student-newspapers Recommended Citation Salve Regina College, "Nautilus, Vol. 35 No. 6 (May 1982)" (1982). Student Newspapers. 67. https://digitalcommons.salve.edu/student-newspapers/67 This Book is brought to you for free and open access by the Archives and Special Collections at Digital Commons @ Salve Regina. It has been accepted for inclusion in Student Newspapers by an authorized administrator of Digital Commons @ Salve Regina. For more information, please contact [email protected]. ~ ·· Vol. XXXV, No. 6 SALVE REGINA - THE NEWPORT COLLEGE May 1982 Governor J. J. Garrahy Addresses Salve Students Conduct Newport County Olympics Honors and Awards Convocation by KATHY LaPORTE Columbus Tootsie Roll Drive, pro by JILL CRONIN Study - Spanish; Diane Griffin, "The committees have been ceeds of which were earmarked to "The pursuit of excellence in R.I. Chapter - International Fed working hard consistently," and help those with special needs. which you have engaged in these eration of Catholic Alumni. according to Cindy McVeigh, Stu The Food Committee, led by past years does not end now. Outstanding Scholastic dent Director of the Newport Chyleene Flynn, arranged for Rather it continues throughout Achievement Awards County Olympics, " ... we couldn't Domino's Pizza to provide all the your lifetime." Governor J. Joseph Valedictorian: Mary Beth Cor do without these people." food and drink for the athletes; Garrahy addressed the families, deiro, Raytheon Company Award; Those who attended the Olym· they requested the concession students, and friends at the 32nd Seniors: Jo-Ann Bettencourt, pies last Saturday were as im- truck also. -
The Following List Represents the Colleges and Universities to Which
The following list represents the colleges and universities to which Suffield High School graduates have been offered admission in the last two years: University of Alabama Emory University Mercy College Salve Regina University American International College Endicott College Merrimack College School of the Art Institute of Chicago American University Fairfield University University of Miami The University of Scranton Anna Maria College Fitchburg State University Michigan State University Seton Hall University Arcadia University Flagler College University of Missouri Columbia Siena College University of Arizona Florida Atlantic University Mitchell College Simmons College Arizona State University Florida Gulf Coast University Molloy College Skidmore College Asnuntuck Community College Florida Institute of Technology Monmouth University University of Southern California Assumption College Florida International University Montana State University Southern CT State University College of the Atlantic Florida Southern College Monterey Peninsula College University of Southern Maine Auburn University Florida State University Mount Holyoke College Southern New Hampshire University Austin Community College University of Florida College of Mount Saint Vincent Southern Vermont College Babson College Fordham University New England College Southern Virginia University Bard College Framingham State University University of New England Spartan College of Aeronautics & Barry University Franciscan University of Steubenville New England Institute of Technology -

Member Colleges & Universities
Bringing Colleges & Students Together SAGESholars® Member Colleges & Universities It Is Our Privilege To Partner With 427 Private Colleges & Universities April 2nd, 2021 Alabama Emmanuel College Huntington University Maryland Institute College of Art Faulkner University Morris Brown Indiana Institute of Technology Mount St. Mary’s University Stillman College Oglethorpe University Indiana Wesleyan University Stevenson University Arizona Point University Manchester University Washington Adventist University Benedictine University at Mesa Reinhardt University Marian University Massachusetts Embry-Riddle Aeronautical Savannah College of Art & Design Oakland City University Anna Maria College University - AZ Shorter University Saint Mary’s College Bentley University Grand Canyon University Toccoa Falls College Saint Mary-of-the-Woods College Clark University Prescott College Wesleyan College Taylor University Dean College Arkansas Young Harris College Trine University Eastern Nazarene College Harding University Hawaii University of Evansville Endicott College Lyon College Chaminade University of Honolulu University of Indianapolis Gordon College Ouachita Baptist University Idaho Valparaiso University Lasell University University of the Ozarks Northwest Nazarene University Wabash College Nichols College California Illinois Iowa Northeast Maritime Institute Alliant International University Benedictine University Briar Cliff University Springfield College Azusa Pacific University Blackburn College Buena Vista University Suffolk University California -

Newton North High School 2020-2021 School Profile
Newton North High School 2020-2021 School Profile “Learning sustains the human spirit.” 457 Walnut Street CEEB Code = 221-555 Counseling Office Phone: 617-559-6230 Newtonville, Massachusetts 02460 www.newton.k12.ma.us Counseling Office Fax: 617-559-6249 NNHS Distance Learning Grading Policy David Fleishman, Ed.D. Superintendent of Schools Newton North High School transitioned from traditional in-person learning to a fully Henry Turner, Ed.D. remote distance education model on March 13, 2020. During the Spring of 2020, Principal instruction was mostly asynchronous and all courses were graded on a pass/no grade basis for an extended third marking period that spanned the remainder of the year. Beth Swederskas 6230 Final year grades were issued as letter grades whenever possible and reflected the Counseling Department Chair average of all work completed between September 2019 and the close of school in March 2020. Sara Foley 6230 Counseling Administrative Asst. For the 2020-2021 school year, Newton North continues to operate primarily College Counselors Extension remotely, except for a cohort of high needs students who are being supported in Jennifer Geraghty 6348 the building and accessing instruction remotely from the school building. Only Jillian Hall 6349 substantially-separate special education classes are being taught in-person in the Melissa Hanenberger 6347 building. All other courses are being taught synchronously, online, with three class School Counselors meetings per week. Some elective offerings that previously met twice weekly for the Brendan Amedio 6242 full year or for half of the year now meet three times weekly for half the year or one Nancy Decoteau 6275 quarter of the year, respectively. -

2021 - 2022 CATALOG This Publication Provides Information Concerning the Programs at Nichols College and Does Not Constitute a Contract with the Student
2021 - 2022 CATALOG This publication provides information concerning the programs at Nichols College and does not constitute a contract with the student. The policies and procedures contained in the 2021-2022 Nichols College Catalog will remain in effect until June 30, 2022. Nichols College reserves the right to change at any time the rules governing admission, tuition, fees, courses, the granting of degrees, or any other regulations affecting the campus community. Such changes are to take effect whenever College officials deem necessary and will be communicated via written notice whenever possible or other means as appropriate. NICHOLS COLLEGE Center Road P.O. Box 5000 Dudley, Massachusetts 01571-5000 Catalog of Nichols College July 2021 Volume LIII Table of Contents Minors & Certificates . 81 Minors in Business................................................................................. 81 Minors in Liberal Arts ............................................................................ 83 Business Administration Minor ........................................................... 83 Civic Leadership and Politics Minor .................................................... 84 President’s Message . .2 Gender and Diversity Studies Minor................................................... 84 Nichols College Mission . .3 Liberal Arts Minor ................................................................................. 84 General Information . .4 Certificate in Business Analytics ........................................................ -

Newsbulletin Vol. 9, No. 18
Salve Regina University Digital Commons @ Salve Regina Newsbulletin Archives and Special Collections 2-12-1981 Newsbulletin vol. 9, no. 18 Salve Regina College Follow this and additional works at: https://digitalcommons.salve.edu/newsbulletin Part of the Education Commons Recommended Citation Salve Regina College, "Newsbulletin vol. 9, no. 18" (1981). Newsbulletin. 229. https://digitalcommons.salve.edu/newsbulletin/229 This News Article is brought to you for free and open access by the Archives and Special Collections at Digital Commons @ Salve Regina. It has been accepted for inclusion in Newsbulletin by an authorized administrator of Digital Commons @ Salve Regina. For more information, please contact [email protected]. J\!ewstu/fetin The Newport College Salve Regina Newport, Rhode Island 02840 Office of College Information ( 401 ) 84 7-6650 Ext. 223 Published for the Newport College Community on a weekly basis by the Office of College Information, Extension 228. Deadline date for notices: Tuesday, NOON time. VoL 9 No. 18 February 12, 1981 SISTER MARY MCAULIFFE ACCEPTS NEW POSITION Sister Mary McAuliffe, former Trustee of Salve Regina College and former Director of Research and Planning, has accepted a position with the Massachusetts Department of Education as Principal and Director of Education and Train ing at Massachusetts Hospital School in Canton. On leave from Salve Regina College for two years, Sister will con tinue her association with the College as Adjunct Professor in the area of special needs education, Sister is completing her doctoral studies in Humanistic Education and Human Services with a concentration in admin istration at Boston University, Her doctoral dissertation is entitled "Changing Patterns of Relationships Between Sponsoring Religious Bodies and Catholic Colleges." Sister's new position brings her into a leadership role as the chief educational planner of one of the most unique schools in the country, Massachusetts Hospital School was founded in 1964 for physically handicapped children with normal intelligence. -
Iconic Nichols College Statue Damaged During Super Bowl
Free by request to residents of Webster, Dudley and the Oxfords SEND YOUR NEWS AND PICS TO [email protected] Friday, February 15, 2019 Iconic Nichols College Public hearing will statue damaged during explore DPW Super Bowl celebration project possibilities BY JASON BLEAU recommendations. This would TIMES CORRESPONDENT allow for a proper public forum for citizens to have their say DUDLEY – The Dudley Board and fully consider the advan- of Selectmen is continuing to tages and perceived setbacks ponder the possibility of a of creating a Department of Department of Public Works Public Works versus remain- including what steps would ing with separate highway and be required should the town water and sewer departments. choose to exercise the option. Selectmen then inquired The board briefly touched about how and when a decision on the long-standing subject would be made following the during a meeting late January public hearing. Would the deci- where Town Administrator sion be made at that hearing or Greg Balukonis responded to would there be time to digest inquiries from selectmen about the information and further exactly how they would go discuss the matter at subse- about initiating a new DPW. quent hearings? Balukonis said Balukonis said there are actu- the best course of action would ally two ways to do so, but one be to allow the information to is much less complicated than sink in before taking a vote. the other. “I think there’s always a good “The first (option) is to adopt opportunity to digest. I think Courtesy Photo Chapter 41 Section 69c through it’s always wise to hear what f. -
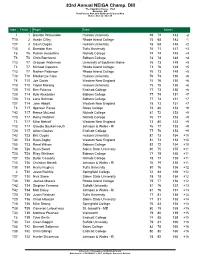
83Rd Annual NEIGA Champ. DIII the Captains Course - Port Brewster, MA Port Course Men and Starboard Course Men Dates: Oct 22 - Oct 23
83rd Annual NEIGA Champ. DIII The Captains Course - Port Brewster, MA Port Course Men and Starboard Course Men Dates: Oct 22 - Oct 23 Start Finish Player Team Scores 1 1 Daulton Wickenden Husson University 69 73 142 -2 T10 2 Austin Cilley Rhode Island College 75 68 143 -1 T27 3 Gavin Dugas Husson University 78 68 146 +2 T13 4 Brandon Karr Tufts University 76 71 147 +3 T6 T5 Patrick Hesseltine Nichols College 74 74 148 +4 T6 T5 Chris Bornhorst Babson College 74 74 148 +4 T13 T7 Grayson Waterman University of Southern Maine 76 73 149 +5 T3 T7 Michael Caparco Rhode Island College 73 76 149 +5 T13 T7 Nathan Patterson Rhode Island College 76 73 149 +5 T13 T10 Mackenzie Clow Husson University 76 74 150 +6 T6 T10 Joe Ciolek Western New England 74 76 150 +6 T10 T10 Taylor Morang Husson University 75 75 150 +6 T20 T10 Ben Palazzo Endicott College 77 73 150 +6 T20 T14 Kyle Alexander Babson College 77 74 151 +7 T20 T14 Lane Bohman Babson College 77 74 151 +7 T27 T14 John Abbott Western New England 78 73 151 +7 T3 T17 Spencer Pierce Bates College 73 80 153 +9 T42 T17 Reece McLeod Nichols College 81 72 153 +9 T13 T17 Remy Fletcher Nichols College 76 77 153 +9 T3 T17 Mike Metcalf Western New England 73 80 153 +9 T13 T17 Claudio Soukamneuth Johnson & Wales - RI 76 77 153 +9 T20 T17 Athan Goulas Endicott College 77 76 153 +9 T42 T23 Eric Dugas Husson University 81 73 154 +10 T42 T23 Ryan Zogby Western New England 81 73 154 +10 T55 T23 Reed Wilson Babson College 82 72 154 +10 T38 T26 Ryan Swart Salem State University 80 75 155 +11 T20 T26 Riley Whitham