Methodological Issues in Measuring Health-Related Quality of Life
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-

Study in Taiwan - 7% Rich and Colorful Culture - 15% in Taiwan, Ancient Chinese Culture Is Uniquely Interwoven No.7 in the Fabric of Modern Society
Le ar ni ng pl us a d v e n t u r e Study in Foundation for International Cooperation in Higher Education of Taiwan (FICHET) Address: Room 202, No.5, Lane 199, Kinghua Street, Taipei City, Taiwan 10650, R.O.C. Taiwan Website: www.fichet.org.tw Tel: +886-2-23222280 Fax: +886-2-23222528 Ministry of Education, R.O.C. Address: No.5, ZhongShan South Road, Taipei, Taiwan 10051, R.O.C. Website: www.edu.tw www.studyintaiwan.org S t u d y n i T a i w a n FICHET: Your all – inclusive information source for studying in Taiwan FICHET (The Foundation for International Cooperation in Higher Education of Taiwan) is a Non-Profit Organization founded in 2005. It currently has 114 member universities. Tel: +886-2-23222280 Fax: +886-2-23222528 E-mail: [email protected] www.fichet.org.tw 加工:封面全面上霧P 局部上亮光 Why Taiwan? International Students’ Perspectives / Reasons Why Taiwan?1 Why Taiwan? Taiwan has an outstanding higher education system that provides opportunities for international students to study a wide variety of subjects, ranging from Chinese language and history to tropical agriculture and forestry, genetic engineering, business, semi-conductors and more. Chinese culture holds education and scholarship in high regard, and nowhere is this truer than in Taiwan. In Taiwan you will experience a vibrant, modern society rooted in one of world’s most venerable cultures, and populated by some of the most friendly and hospitable people on the planet. A great education can lead to a great future. What are you waiting for? Come to Taiwan and fulfill your dreams. -

Supplementary Information
SUPPLEMENTARY INFORMATION Astragalus polysaccharides (PG2) enhances the M1 polarization of macrophages, functional maturation of dendritic cells, and T cell-mediated anticancer immune responses in patients with lung cancer Oluwaseun Adebayo Bamodu a,b# , Kuang-Tai Kuo c,d# , Chun-Hua Wang e,f , Wen-Chien Huang g,h , Alexander T.H. Wu i, Jo-Ting Tsai j,k , Kang-Yun Lee l, Chi-Tai Yeh c,d,m* and Liang-Shun Wang a,b * a Division of Hematology & Oncology, Department of Medicine, Shuang Ho Hospital, Taipei Medical University, New Taipei City, Taiwan. b Department of Medical Research and Education, Shuang Ho Hospital, Taipei Medical University, New Taipei City, Taiwan. c Division of Thoracic Surgery, Department of Surgery, Shuang Ho Hospital, Taipei Medical University, New Taipei City, Taiwan. d Division of Thoracic Surgery, Department of Surgery, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan. e Department of Dermatology, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan. f School of Medicine, Buddhist Tzu Chi University, Hualien, Taiwan g MacKay Medical College, Taipei, Taiwan. h Division of Thoracic Surgery, Department of Surgery, MacKay Memorial Hospital, Taipei, Taiwan. i The Ph.D. Program for Translational Medicine, College of Medical Science and Technology, Taipei Medical University, Taipei, Taiwan j Department of Radiation Oncology, Shuang Ho Hospital, Taipei Medical University, New Taipei City, Taiwan. k Department of Radiology, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan. l Division of Pulmonary Medicine, Department of Internal Medicine, Shuang Ho Hospital, Taipei Medical University, Taiwan. m Department of Biotechnology and Pharmaceutical Technology, Yuanpei University of Medical Technology, Hsinchu City 30015, Taiwan # These authors contributed equally to this work. -

Tuition Fees Waiver
Tzu Chi University TCU_GPS 3.0 G P S Globalocalization People Centric Sustainability 全球在 地 以人為本 永續發展 1986 Tzu Chi General Hospital 2002 Tzu Chi Medical Center 1989 Tzu Chi College of Nursing 1999 Tzu Chi College of Technology Founder 1994 Tzu Chi College of Medicine 2000 Tzu Chi University Dharma Master Cheng Yen School Mottos Kindness, Compassion, Joy, Unselfish Giving Tzu Chi's Comprehensive Education System In early 2000, a comprehensive education from kindergarten up to the Ph.D. Kindergarten Elementary School Junior High School University Tzu Chi's Medical System Buddhist Tzu Chi Medical Foundation Hualien Tzu Chi Hospital Yuli Branch Kuanshan Branch Taipei Tzu Chi Hospital International Medical Service Center Buddhist Tzu Chi Medical Foundation Taichung Tzu Chi Hospital Buddhist Tzu Chi Medical Foundation Douliu Tzu Chi Hospital Buddhist Tzu Chi Medical Foundation Dalin Tzu Chi Hospital • President(Since 2019/08~) • Vice president(Since 2017/08~2019/07) • Provost(Since 2014/09~2017/07) • Director,Center for Faculty Development and Teaching Resources (Since 2013/08~) • Professor, Institute of Medical Sciences(Since 2014/08~) • Ph.D., University of Southern California, California, USA. • M.Sc.Indiana University, Bloomington, USA. • B.Sc.National Taiwan University, Taipei, Taiwan. Presented Lifelong Honorary President Fellowship and Outstanding Female Scientist Award by the Ingrid Y. Liu, Ph.D. Thai Neuroscience Society. 8 World Asia Taiwan Tzu Chi University is ranked 67th in the world, 10th in Asia, and tops the list in Taiwan, among 462 universities 67/462 10 1 by Times Higher University Impact Ranking in 2019. Strategies for SDGs Promotion 101- 26 200 79 201- 77 300 52 82 26 101- 201 201 200 Incorporate SDGs concepts into curriculums and education. -

Introduction Fields of Interest for Collaboration
Tzu Chi University Wenzao Ursuline University of Languages 慈濟大學 文藻外語大學 INTRODUCTION Ingrid Liu - 劉怡均 YuJane Chen - 陳玉珍 INTRODUCTION Dean Chairperson of Department Tzu Chi University was founded in 1994; we have 4 Office of Academic Affairs Department of International Affairs Wenzao Ursuline University of Languages is the first colleges that contain 18 research institutes and 17 institute of higher education in Taiwan focusing on academic departments. We emphasizes the Daily Life Tel : +886-3-8565301 ext.1100 Tel : +886-7-3426031 ext.6124/6101 the teaching of foreign languages. Wenzao has college Education, Virtue Education, Humanities Education Fax : +886-3-8562490 Fax : +886-7-3100743 programs (regular 4-year and upper 2-year), post- and Appreciation for education. Email : [email protected] Email : [email protected] graduate study, Chinese language learning programs, and extension education. Presently, the university has 203 partner institutes around the world. FIELDS OF INTEREST Anita Yang - 楊青穎 Aiden Yeh - 葉佰賢 FOR COLLABORATION Staff Manager of Cooperation and Office of International Affairs Exchange Section FIELDS OF INTEREST 1. Short-term exchange program Office of International and Cross-strait Tel : +886-3-8565301 ext.1018 FOR COLLABORATION 2. Academic exchange Cooperation Fax : +886-3-8574499 Email : [email protected] Tel : +886-7-3426031 ext.2611 1. Dual degrees Fax : +886-7-3100743 (including 2+1+1; 3+1; 2+2, or 3+2 plus etc.) Email : [email protected] 2. Distance learning courses 3. Exchange students 4. Short-term program www.tcu.edu.tw (Summer and tailor-made Mandarin course etc.) Address: No. -

The Competitiveness of Taiwan Higher Education
The Competitiveness of Taiwan Higher Education Presented By Wan-Lee Cheng, Ph.D. Chair Professor Chung Yuan Christian University At The Executive Conference on International and Cross- strait Affairs, 2013 June 26, 2013 Presentation Outlines • Taiwan Students Study Abroad (60s, 70s and 80s) • Time for Taiwan Higher Education Institutions to Make Contributions • Quality Assurance of Taiwan Higher Education • Government Investments in Research and Teaching • Uniqueness and Worthiness of Studying in Taiwan • Internationalization of Campuses • Additional Values on University Campuses in Taiwan • Conclusion 2 • The number of study abroad over the years in the 60s 70s and 80s • Overseas scholars returning homeland TAIWAN STUDENTS STUDY ABROAD 3 Taiwan Students Study Abroad Number of people approved to study abroad (A) 215,830 64,216 31,365 21,248 4,515 1950-1959 1960-1969 1970-1979 1980-1989 1990-1998 4 Taiwan Students Study Abroad Number of people return to Taiwan (B) 37,883 14,880 5,166 400 1,172 1950-59 1960-69 1970-79 **1980-1989 **1990-1998 5 Taiwan Students Study Abroad Percentage of return to Taiwan (B) / (A) * 100 23.17 17.55 16.5 8.9 5.5 1950-59 1960-69 1970-79 **1980-1989 **1990-1998 6 Taiwan Students Study Abroad Data from MOE 7 Number of Returning Study Abroad Scholars Employed in Various Sectors 1971-1998 Year Total Employment Assisted by the Youth Commission Self Employed(%) Research University Government Public Private Organizations (%) Teaching (%) Units (%) Businesses (%) Businesses (%) 1971 291 6.5 52.2 10 10.7 5.5 15.1 1972 -

APANE (Asian and Pacific Alliance for Nursing Education)
Asian and Pacific Alliance for Nursing Education Opening Ceremony and International Congress Multi-culture Collaboration in Nursing Education Friday, September 6, 2019 9:00 am Registration & Networking Opening Remarks 10:20 am CHAIR: Jing-Jy Wang 王靜枝, Chair of APANE Preparation Committee Keynote speech─ Nursing leadership: Bridging education and practice SPEAKER: 11:05 am MODERATOR: Professor Lian-Hua Huang 黃璉華 Hsiu-Hung Wang 王秀紅, President of Taiwan Nurses Association (TWNA) ICN Board Member 12:00 pm Lunch & Poster Exhibition, Networking Plenary speech ─Sustainable Development Goals and nursing education MODERATOR: SPEAKER: 1:30 pm Yu-Yun Hsu 許⽟雲, President of Taiwan Association of Nursing Education (TANE) Director Johnson Huang 黃兆聖 AdvMeds Co., Ltd., Taiwan Professor Patsy Yates Yann-Fen Chiou Chao 邱艷芬, Chair of College of Nursing, Hungkuang University Queensland University of Technology, Australia Associate Professor and Dean Yajai Sitthimongkol Shao-Yu Tsai 蔡劭瑜, Professor of School of Nursing, National Taiwan University ยาใจ สิทธิมงคล Mahidol University, Thailand 2:45 pm Refreshment Break & Poster Exhibition, Networking Partner Presentations & Exhibitions Jing-Jy Wang 王靜枝, Chair of Fan-Hao Chou 周汎澔, Vice Chair of Ying-Ju Chang 張瑩如, Director of APANE Preparation Committee Education Committee of TANE Nursing Department, NCKU Hospital 1. Asia University 12. Fu Jen Catholic University 22. National Taipei University of 2. Chang Gung University of Science 13. Hungkuang University Nursing and Health Sciences and Technology 14. Pham Ngoc Thach University of 23. National Taiwan University 3. Chang Jung Christian University Medicine 24. University of Puthisastra 3:00 pm 4. Association of Indonesian Nurse 15. Kaohsiung Medical University 25. National Yang-Ming University Education Center 16. -

NSF-NSC Summer Institute in Taiwan Program
NSF-NSC Summer Institute in Taiwan Program The National Science Foundation (NSF) has recently announced the 2009 East Asia and Pacific Summer Institutes (EAPSI) program and is accepting applications for U.S. graduate students to do research in Taiwan or Australia , China , Japan , Korea , New Zealand , or Singapore for 8 weeks in the summer of 2009. The Summer Institute in Taiwan (SIT) program is a joint program between the NSF and the National Science Council (NSC) in Taiwan . The program provides U.S. graduate students in science (including social and humanity sciences) and engineering with an opportunity to go to Taiwan in the summer for eight weeks to participate in research projects in the areas of their studies at the participating host institutions. Since the program inaugurated in 2000, NSF and NSC have supported over 100 graduate students. They participated in research works in Taiwan at the host institutions such as National Taiwan University , National Tsing-Hua University , National Central University , Academia Sinica, National Center for High Performance Computing, National Center for Research on Earthquake Engineering, etc. The experience not only has enabled the students to expand the scope of their scholarly works but also has helped them establish personal relationship with scientists in Taiwan, thus better prepare them to collaborate with foreign counterparts in the future. Awardees will receive a $5,000 stipend, a round trip air ticket from NSF, while the NSC in Taiwan will provide additional support to cover living expenses during the period of the summer program. I would highly recommend that you encourage your graduate students to take advantage of this opportunity. -
Building up Students' Overall Competitiveness
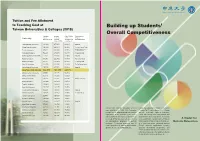
Tuition and Fee Allotment to Teaching Cost at Building up Students’ Taiwan Universities & Colleges (2018) Overall Competitiveness Standard Average Ratio (Tuition Businesses or University Tuition Teaching and Fees/ Religious andFees (NT$) Cost per Average Cost Group Sponsors Student (NT$) per Student) Taipei Medical University 110,914 477,951 23.21% Hospital Chang Gung University 100,884 408,819 24.68% Formosa Plastics Group Tzu Chi University 90,817 330,959 27.00% Fo Guang University 74,246 215,989 34.37% Fo Guang Shan Kaohsiung Medical University 113,625 273,208 42.00% Hospital Huafan University 97,250 222,862 44.00% Religious Group Nanhua University 91,116 191,562 47.56% Fo Guang Shan Yuan Ze University 112,080 231,538 48.41% The Far Eastern Group China Medical University 107,145 217,531 49.26% Hospital Chung Yuan Christian University 102,534 163,875 62.57% Chinese Culture University 99,093 151,274 65.51% Chung Hua University 96,578 139,963 69.00% Tatung University 104,815 151,611 69.13% Tatung Company Dayeh University 100,042 143,934 69.51% Tunghai University 109,000 153,000 71.20% Feng Chia University 104,720 138,175 76.00% Fu Jen Catholic University 98,229 123,812 79.00% Hospital I-SHOU University 109,687 138,852 79.00% E United Group Tamkang University 98,456 124,259 79.23% Soochow University 102,834 129,458 79.43% Asia University 104,894 129,817 80.80% Hospital Ming Chuan University 97,863 120,723 81.06% Providence University 95,262 111,994 85.06% Chung Yuan Christian University (CYCU) Under the leadership of Chair of the Board Shih Chien University 94,716 110,069 86.05% was established in 1955. -

Differences in the Microbial Composition of Hemodialysis Patients Treated with and Without Β-Blockers
Journal of Personalized Medicine Article Differences in the Microbial Composition of Hemodialysis Patients Treated with and without β-Blockers Yi-Ting Lin 1,2,3 , Ting-Yun Lin 4,5 , Szu-Chun Hung 4,5, Po-Yu Liu 6 , Wei-Chun Hung 7, Wei-Chung Tsai 8 , Yi-Chun Tsai 2,9,10 , Rachel Ann Delicano 11, Yun-Shiuan Chuang 1 , Mei-Chuan Kuo 2,10,12, Yi-Wen Chiu 2,10,12 and Ping-Hsun Wu 2,3,12,* 1 Department of Family Medicine, Kaohsiung Medical University Hospital, Kaohsiung 80708, Taiwan; [email protected] (Y.-T.L.); [email protected] (Y.-S.C.) 2 Faculty of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung 80708, Taiwan; [email protected] (Y.-C.T.); [email protected] (M.-C.K.); [email protected] (Y.-W.C.) 3 Graduate Institute of Clinical Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung 80708, Taiwan 4 Division of Nephrology, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City 23142, Taiwan; [email protected] (T.-Y.L.); [email protected] (S.-C.H.) 5 School of Medicine, Tzu Chi University, Hualien 97071, Taiwan 6 Department of Internal Medicine, College of Medicine, National Taiwan University, Taipei 100225, Taiwan; [email protected] 7 Department of Microbiology and Immunology, Kaohsiung Medical University, Kaohsiung 80708, Taiwan; [email protected] 8 Division of Cardiology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung 80708, Taiwan; [email protected] 9 Division of General Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Citation: Lin, Y.-T.; Lin, T.-Y.; Hung, Kaohsiung 80708, Taiwan S.-C.; Liu, P.-Y.; Hung, W.-C.; Tsai, 10 Faculty of Renal Care, College of Medicine, Kaohsiung Medical University, Kaohsiung 80708, Taiwan W.-C.; Tsai, Y.-C.; Delicano, R.A.; 11 Institute of Surgical Sciences, Uppsala University, 752 36 Uppsala, Sweden; [email protected] Chuang, Y.-S.; Kuo, M.-C.; et al. -

Yi-Rung Lin [email protected]
Lin 1 Yi-Rung Lin [email protected] Personal Information. Nationality: Taiwan Education. Ph. D. in English. August, 2007. Claremont Graduate University of The Claremont Colleges, California, U. S. A. Doctoral dissertation: The Politics of Advice: Counsel for Women in Eighteenth-Century British Fiction . Director: Marc Redfield. M. A. in English. January, 2002. Tamkang University, Tamsui, Taipei. Master thesis: The Holy Idiot Archetype: Madness as a Metaphor for Sanity in Twentieth-Century Drama and Film. B. A. in English. June, 1996. Tamkang University. B. A. in Spanish. June, 1996. Tamkang University. Academic Appointments. August, 2016 to date Full-time Associate Professor. Department of English Language and Literature, Tzu Chi University, Hualien. August, 2008 – July, 2016 Full-time Assistant Professor. Department of English Language and Literature, Tzu Chi University, Hualien. February, 2008 – July, 2008 Full-time Assistant Professor. Department of Applied English, Ming Chuan University, Taipei City. August, 2007 – July, 2008 Adjunct Lecturer. Division of Continuing Education, Chinese Culture University, Taipei City. August, 2002 – July, 2003 Adjunct Lecturer. Division of Continuing Education, Chinese Culture University. August, 2002 – July, 2003 Adjunct Lecturer. English Department, Shih Hsin University, Taipei City. August, 2002 – July, 2003 Adjunct Lecturer. Department of Applied Foreign Languages, Kwang Wu Technical College, Taipei City. Lin 2 August, 2002 – July, 2003 Adjunct Lecturer. English Program, Mackay Junior -

10Reasons for Learning Chinese in Taiwan
到 Tuition INTERNATIONAL 41 Chinese Language Centers in Taiwan provide various types of courses, tuition fee also varies from every center. 臺 The following is a brief summary of tuition fees: 灣 Total hrs Tuition fee (USD1 NTD30) STUDENTS IN TAIWAN General Course 180 hours or more NTD18,300–43,500 (about USD 610–1,450) Intensive Summer Course 80–240 hours NTD12,000–65,000 (about USD 400–2,200) Language Center 1 Mandarin Learning Center, Chinese Culture University Now it is my second time here, and I still enjoy to Scholarship the most the opportunities that studying in Taiwan Huayu (Mandarin) Enrichment Scholarship offers me. Taiwan is a really beautiful island, with nice beaches and natural sites. Taipei is a perfect sized The Ministry of Education (MOE) of Taiwan provides the Huayu Enrichment Scholarship (HES) to encourage city, not too big not too small, extremely convenient international students and individuals to undertake Chinese language study in Taiwan. Ruiz Varela Pedro and with lots of leisure activities available. Sports, Fernando exhibitions, cultural events, gastronomy, nightlife, etc Application date Duration Amount (USD1 NTD30) from Spain and everything at a very reasonable cost. February 1 to March 31 summer classes (2 months), 3,6, or 9 months, or 1 year monthly stipend: NTD 25,000 (USD 834) LEARNING CHINESE IN TAIWAN For more information, please visit the Taiwan Scholarship and Huayu Enrichment Scholarship website at taiwanscholarship.moe.gov.tw or contact a Taiwan representative office directly Language Center (english.moe.gov.tw About MOE Overseas Offices) Chinese Language Center, Some Chinese learning centers offer scholarships. -

CCT327 Enhances TRAIL-Induced Apoptosis Through the Induction of Death Receptors and Downregulation of Cell Survival Proteins in TRAIL-Resistant Human Leukemia Cells
ONCOLOGY REPORTS 32: 1257-1264, 2014 CCT327 enhances TRAIL-induced apoptosis through the induction of death receptors and downregulation of cell survival proteins in TRAIL-resistant human leukemia cells YAN-JIN LIU1, YING-CHAO LIN2,3, JANG-CHANG LEE4, SHENG-CHU KUO1, CHI-TANG HO5, LI-JIAU HUANG1, DAIH-HUANG KUO6 and TZONG-DER WAY7-9 1Graduate Institute of Pharmaceutical Chemistry, College of Pharmacy, China Medical University, Taichung; 2Division of Neurosurgery, Buddhist Tzu Chi General Hospital, Taichung Branch, Taichung; 3School of Medicine, Tzu Chi University, Hualien; 4Department of Pharmacy, China Medical University, Taichung, Taiwan, R.O.C.; 5Department of Food Science, Rutgers University, New Brunswick, NJ, USA; 6Graduate Institute of Pharmaceutical Technology, College of Pharmacy and Health Care, Tajen University, Pingtung; 7Department of Biological Science and Technology, College of Life Sciences, China Medical University, Taichung; 8Institute of Biochemistry, College of Life Science, National Chung Hsing University, Taichung; 9Department of Health and Nutrition Biotechnology, College of Health Science, Asia University, Taichung, Taiwan, R.O.C. Received March 7, 2014; Accepted May 20, 2014 DOI: 10.3892/or.2014.3317 Abstract. Tumor necrosis factor-related apoptosis-inducing the induction of DRs by CCT327. Taken together, these results ligand (TRAIL) has potential application in cancer therapy showed that CCT327 combined with TRAIL treatment may and it has the ability to selectively kill cancer cells without provide an effective therapeutic strategy for cancer. affecting normal cells. However, the development of resistance to TRAIL in cancer cells cannot be avoided. Introduction This study investigated the effects of 2-(5-methylseleno- phen-2-yl)-6,7-methylenedioxyquinolin-4-one (CCT327), The tumor necrosis factor (TNF)-related apoptosis-inducing an analogue of quinolin-4-one, on the sensitization of ligand (TRAIL) is a member of the TNF superfamily, and is an cancer cells to TRAIL and on TRAIL-induced apoptosis in attractive anticancer agent.