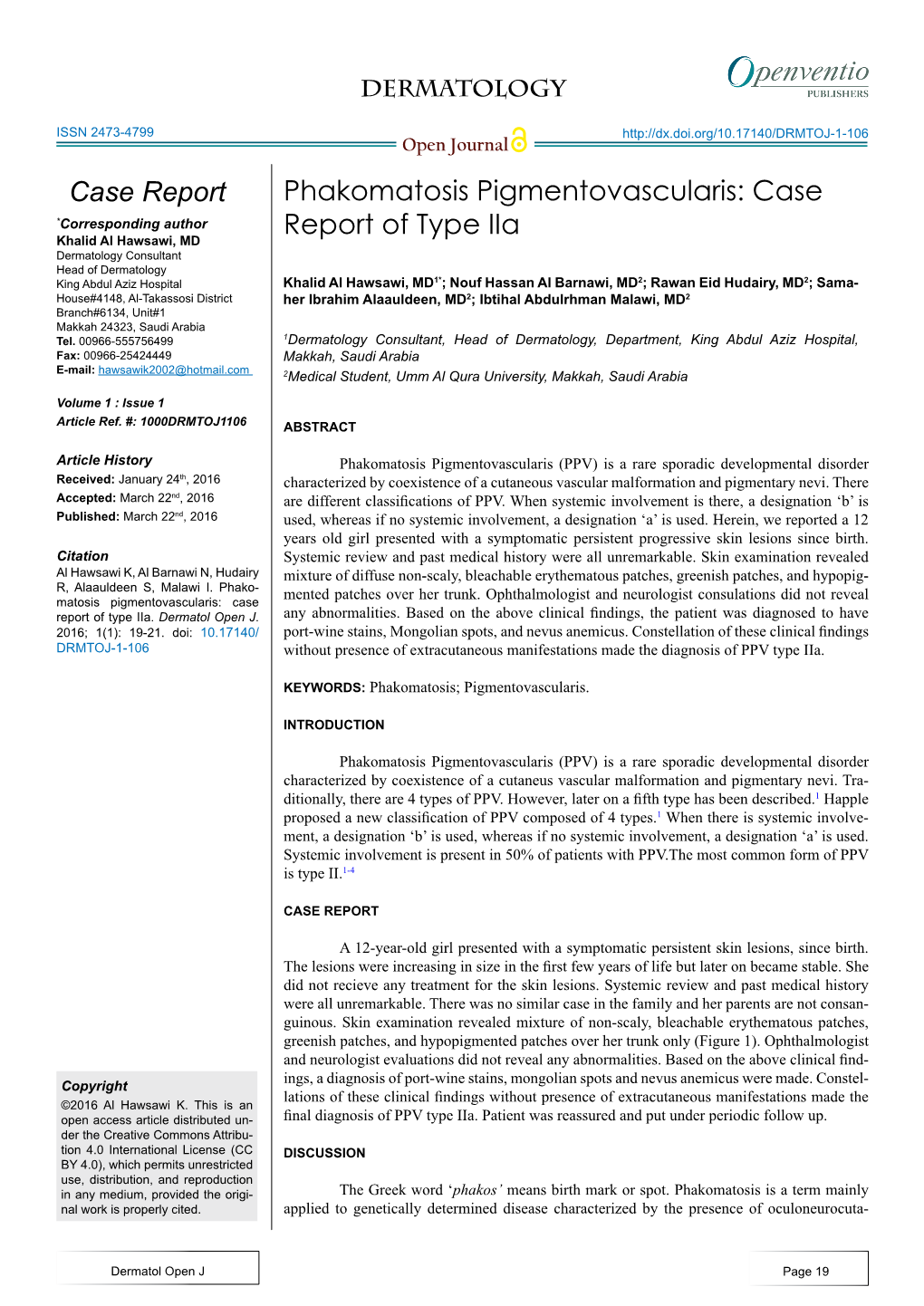
Phakomatosis Pigmentovascularis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Multiple, Primary Brain Tumors with Diverse Origins
Published online: 2019-09-02 Case Series Multiple, Primary Brain Tumors with Diverse Origins and Different Localizations: Case Series and Review of the Literature Thara Tunthanathip, Kanet Kanjanapradit1, Sanguansin Ratanalert, Nakornchai Phuenpathom, Thakul Oearsakul, Anukoon Kaewborisutsakul Department of Surgery, Background: Multiple, primary brain tumors with different histological types Neurosurgical Unit, Faculty occurring in the same patient are extremely rare. Several hypotheses have been of Medicine, Prince of Songkla University, proposed, and the pathophysiology of coexisting tumors has long been debated; 1Department of Pathology, however, due to low incidence, standard practices for this scenario are still Abstract Faculty of Medicine, Prince inconclusive. Case Description: The authors describe 6 cases of coexisting of Songkla University, tumors. By conducting a literature research focused on the computed tomography Hat Yai, Songkhla, 90110, (CT) era and patients without prior radiation or phakomatosis. Sixty‑five such Thailand reported cases were identified. In addition, the authors summarize their experience in 6 patients including histopathological features, chronological presentations, outcomes, mortality, and management from their series as well as from previous cases from the reported literature. Conclusion: The coexistence of multiple, primary brain tumors is an interesting condition. Surgical management remains the major treatment; malignant histology has a poor prognostic factor. Keywords: Coexistence of brain tumor, diffuse astrocytoma, glioblastoma, meningioma, multiple primary brain tumor Introduction gender‑specific distribution, the incidence rate of tumor he association of multiple, primary brain tumors of the meninges is higher in females (10.51/100,000) T with different histology occurring simultaneously rather than in males (4.85/100,000), while the in the same patient is an extremely rare condition. -

Tuberous Sclerosis Epilepsy and Psychosis by Adults
Journal of Neurology & Stroke Short Communication Open Access Tuberous sclerosis epilepsy and psychosis by adults Introduction Volume 8 Issue 6 - 2018 The tuberous sclerosis (TS) or tuberous sclerosis complex (TSC) is a multisystem, autosomal dominant disorder by children and adults, Andrej N Ilanković,1 NikolaN Ilanković2 results from mutations in one of two genes, TSC1 (encoding hamartin) 1Universitz Psychiatric Clinic, Dep. of Neuropszchiatrz, Serbia or TSC2 (encoding tuberin). First described in depth by Bourneville in 2General hospital “MEDIGROUP”, Serbia 1880 (Morbus Bourneville, Epiloa).1 TS and TSC often causes disabling neuropsychiatric disorders, Correspondence: Andrej N. Ilanković, MD, PhD, Ass Prof, including epilepsy, mental retardation, autism and psychosis. Universitz Psychiatric Clinic, Dep. of Neuropszchiatrz, Belgrade, Serbia, Pasterova 2, Email Additional major features of the disease include dermatologic manifestations such as facial angiofibromas, renal angiomyolipomas, Received: October 09, 2018 | Published: December 26, 2018 and pulmonary lymphangiomyomatosis. TSC has a wide clinical spectrum of disease, and many patients have minimal signs and symptoms with or without neurologic and psychiatric disability.2 TS is one of “phakomatosis” a group of congenital hereditary developmental anomalies having selective involvement of tissues of ectodermal origin, which develop disseminated glial hamartomas. Examples of phakomatosis are neurofibromatosis, tuberous sclerosis, DERMATOLOGICAL LESIONS Sturge-Weber syndrome, and von Hippel-Lindau disease.”3 Shagrin patch Papula Hypomelanic macula Angiofibroma Figure 2 Typical endocranial (cortical, subcortical and subependymal) lesions by Tuberous sclerosis. The molecular genetics analysis in multigenerational families and positional cloning were used to map both the TSC1 and TSC2 genes 32- 34 . The TSC2 gene, which is located on chromosome 16p13, encodes Figure 1 Typical skin lesion for Tuberous sclerosis. -

Neurocutaneous Syndromes (Covers Schwannoma, Hemangioblastoma, ...) Andrea Rossi, MD Neuroradiology Unit G
06/04/19 The Neurocutaneous Syndromes, also called Phakomatoses, are a heterogeneous group of congenital disorders involving structures primarily derived from: - NEUROECTODERM: CNS, PNS, skin, eye - MESODERM: blood vessels, bone, cartilage - ENDODERM: epithelial lining the GI tract NEURAL CREST Neurocutaneous syndromes (covers schwannoma, hemangioblastoma, ...) Andrea Rossi, MD Neuroradiology Unit G. Gaslini Children’s Hospital - Genoa, Italy [email protected] Sarnat H J Child Neurol 2005 OTHER RARE PHAKOMATOSES Basal Cell Nevus Syndrome phakomatosis [fak′ōmətō′sis] pl. phakomatoses Organoid Nevus Syndrome Cowden-Lhermitte-Duclos (COLD) Epidermal nevus Syndrome Etymology: Gk, φακός phako: spot, lens, oma: tumor, osis: condition Encephalocraniocutaneous Lipomatosis Xeroderma pigmentosum This term was introduced by Jan van der Hoeve, a Dutch ophthalmologist, MELANO in 1920, to indicate the benign tumor-like nodules of the eye in VASCULAR PHAKOMATOSES PHAKOMATOSES - Neurofibromatosis (Recklinghausen's disease) PHACE Syndrome Hypomelanosis of Ito Ataxia Telangiectasia Incontinentia Pigmenti - Tuberous sclerosis (Bourneville's disease) Wyburn-Mason Waardenburg Syndrome Neurocutaneous Melanosis HHT Nevus of Ota - Encephalotrigeminal angiomatosis (Sturge-Weber syndrome) Blue Rubber Bleb Nevus Meningioangiomatosis McCune-Albright - Cerebroretinal angiomatosis (Von Hippel-Lindau disease) Nelson Syndrome MAIN RETINAL HAMARTOMAS PHAKOMATOSES The original “Phakoma” of van der Hoeve in a TSC patient Neurofibromatosis 1 Neurofibromatosis 2 Tuberous -

Ocular Manifestations in Neurocutaneous Syndromes with Emphasis on Neurofibromatosis – a Descriptive Observational Study
Jebmh.com Original Research Article Ocular Manifestations in Neurocutaneous Syndromes with Emphasis on Neurofibromatosis – A Descriptive Observational Study Sija Sudha1, Deepa Molathe Gopalan2 1 Department of Ophthalmology, Government T.D. Medical College, Alappuzha, Kerala, India. 2 Department of Ophthalmology, Government Medical College, Ernakulam, Kerala, India. ABSTRACT BACKGROUND Neurocutaneous syndromes (NCS) are a group of genetic disorders that produce Corresponding Author: a variety of developmental abnormalities of the eye. Ophthalmic manifestations Dr. Sija Sudha, Pranamam CSM Nagar, Edapazhinji, usually appear early in life and progress with time. The study was conducted to Thiruvananthapuram – 695010, know the prevalence of ocular manifestations in neurocutaneous syndromes with Kerala, India. emphasis on neurofibromatosis. E-mail: [email protected] METHODS DOI: 10.18410/jebmh/2021/100 This study was conducted in ophthalmology department at a tertiary care hospital during a period of 2 years among 30 patients. All phakomatoses referred from How to Cite This Article: other specialty departments for ophthalmological evaluation and cases diagnosed Sudha S, Gopalan DM. Ocular Manifestations in neurocutaneous in ophthalmology department during routine evaluation were included in the study. syndromes with emphasis on neurofibromatosis – a descriptive RESULTS observational study. J Evid Based Med Neurofibromatosis type 1 (NF-1) accounted for most of (66.67 %) the cases Healthc 2021;8(09):512-516. DOI: followed by Sturge Weber syndrome (SWS) (20 %). Majority (55 %) of NF-1 and 10.18410/jebmh/2021/100 83.33 % of SWS and all patients of other phakomatoses were in the age group < 30 yrs. 55 % of NF-1 patients were males. 65 % of NF-1 patients gave positive Submission 11-09-2020, family history. -
Revista4vol88ingles001 Layout 1
507 CONTINUING MEDICAL EDUCATION ▲ Cutaneous mosaicisms: concepts, patterns and classifications* Mosaicismos cutâneos: conceitos, padrões e classificações Samara Silva Kouzak1 Marcela Sena Teixeira Mendes2 Izelda Maria Carvalho Costa3 DOI: http://dx.doi.org/10.1590/abd1806-4841.20132015 Abstract: A mosaic is an organism composed of two or more genetically distinct cell populations derived from a genetically homogeneous zygote. Cutaneous mosaicisms are the clinical expressions of these disorders. The main event which allows the existence of mosaicism is a genetic mutation, either structural or functional. Cutaneous mosaicisms usually manifest by specific patterns on the skin and the archetypic pattern is the system of Blaschko lines, but others include checkerboard, phylloid, large patches without midline separation and lateralization. Since 1901, when Blaschko lines were first described, the study of mosasicism has helped to elucidate the behavi- or of numerous genetic diseases, generating therapeutic perspectives for these pathologies, including the promi- sing gene therapy. Keywords: Focal dermal hypoplasia; Incontinentia pigmenti; Loss of heterozygosity; Mosaicism; Nevus Resumo: Um mosaico é um organismo formado por duas ou mais populações de células geneticamente distintas originadas a partir de um mesmo zigoto geneticamente homogêneo. Os mosaicismos são as expressões clínicas dessa desordem, e a mutação gênica seu evento determinante, que pode ser tanto estrutural quanto funcional. Os mosaicismos cutâneos costumam se expressar em padrões específicos, dentre os quais podem ser mencionados as prevalentes linhas de Blaschko, o padrão "checkerboard", o padrão filóide, o padrão em placa sem separação na linha média e o padrão de lateralização, que serão abordados neste artigo. Desde 1901, momento da primeira des- crição das linhas de Blaschko, o estudo dos mosaicismos tem contribuído para a elucidação do comportamento de numerosas desordens genéticas, de forma a criar perspectivas terapêuticas para essas doenças, incluindo a pro- missora terapia gênica. -
Sturge Weber Syndrome, Phakomatosis Pigmentovascu- Laris and Down Syndrome in a Newborn Infant
SWISS SOCIETY OF NEONATOLOGY Sturge Weber syndrome, phakomatosis pigmentovascu- laris and Down syndrome in a newborn infant January 2014 2 Völker S, Voelcker T, Neonatal Intensive Care Unit, Children’s Hospital of Aarau, Aarau, Switzerland © Swiss Society of Neonatology, Thomas M Berger, Webmaster 3 Sturge Weber syndrome (SWS) is a neurocutaneous INTRODUCTION disorder affecting skin, central nervous system and eyes. Phakomatosis pigmentovascularis (PPV) is ano- ther neurocutaneous disorder with an association of cutaneous and extracutaneous (visceral, muscular, neurologic or ocular) abnormalities. We present a newborn African boy with SWS with port wine stains and leptomeningeal involvement. Additio- nally, he had multiple Mongolian spots and was also diagnosed with Down syndrome. This boy was born to a 30-year old mother by spontane- CASE REPORT ous vaginal delivery at 41 3/7 weeks of gestation follo- wing premature and prolonged rupture of membranes (10 days). The prenatal ultrasound examinations had been unremarkable. Both parents were from Nigeria and there was no consanguinity. In the delivery room, the infant was intubated because of poor respiratory effort. Apgar scores were 4, 6 and 7 at 1, 5 and 10 minutes, respectively. The arterial umbilical cord pH value was 7.21. He was transferred to our neonatal intensive care unit. Birth weight was 3640 g (P 25-50), body length 50 cm (P 5-10) and head circumference 35 cm (P 10-25). On physical examina- tion, there were facial port wine stains on the left side in the distribution of the first and second branches of the trigeminal nerve (Fig. 1). Furthermore, he showed 4 the port wine stains and numerous Mongolian spots, some of them of huge size, all over his body (Fig. -

Phakomatoses and Their Tumors: Genetics and New Treatment Options Treatment Options
Provisional chapter Chapter 5 Phakomatoses and Their Tumors: Genetics and New Phakomatoses and Their Tumors: Genetics and New Treatment Options Treatment Options Muhammad Taimur Malik, Mohammed MuhammadFaraz Majeed Taimur and Scott Malik, G. Turner Mohammed Faraz Majeed and Scott G. Turner Additional information is available at the end of the chapter Additional information is available at the end of the chapter http://dx.doi.org/10.5772/66207 Abstract In addition to sporadic primary neoplasms of the central nervous system, several genetic syndromes associated with CNS tumors have been identified. Tuberous sclerosis, neu- rofibromatosis-1 and -2, and von Hippel–Lindau syndrome belong to a collection of disorders called phakomatoses, which include both CNS tumors and cutaneous manifes- tations. The underlying genetics of these disorders are being elucidated and offer novel therapies for intervention. Keywords: genetic, phakomatosis, tuberous sclerosis, neurofibromatosis, von Hippel–Lindau 1. Introduction Phakomatoses are disorders which, in addition to skin manifestations, can lead to the devel- opment of tumors within the central and peripheral nervous systems. Due to extensive organ involvement and the complex genetics pathways involved, treatment options are limited. Some of these genetic disorders involve abnormal neural crest migration or terminal differen- tiation, and tumor suppressor gene dysfunction. These may exhibit autosomal dominant or X-linked recessive inheritance. Central nervous system manifestations include seizure, stroke, hearing loss secondary to tumor growth, visual loss secondary to optic gliomas, hydrocephalus, and cognitive deficits, while peripheral manifestations include sensory loss or motor weakness from neurofibromas. The cutaneous manifestations of these disorders are usually ectodermal in origin and can and range from small lesions to involvement of entire dermatomes. -

Neurofibromatosis Imaging Manifestations
Neurofibromatosis Review for Board Examination Study. Matt Covington, MD ListenListen toto theassociated associated Podcast Radiology episodes: Review ABR PCoreodcast Exam, episodes Multisystemic on neurofibromatosis Diseases Parts, available1-3, atavailable theradiologyreview.com at theradiologyreview.com or on your or favorite on your podcastFavorite directory.podcast direcry. NeuroFibromatosis: • A phakomatosis (phakomatoses=neurocutaneous disorders involving the ectoderm involving CNS and other tissues like skin). Other phakomatoses: o Tuberous sclerosis o Von Hippel-Lindau o Sturge-Weber Syndrome o NF1/NF2 o All of these are very commonly tested! o All of these are relatively common diseases NeuroFibromatosis type 1 (NF1) o The most common phakomatosis § Hence possibly the most commonly tested o Autosomal dominant inheritance in many but not all cases (otherwise de novo) § NF1 gene on chromosome 17q11.2 § Tumor suppressor oF Ras/MAPK pathway doesn’t work correctly o Random Fact: NF1 aka von Recklinghausen disease and “von Recklighausen” has 17 letters—this can help you remember this is 17q § In reality are you really going to count letters on your board exam? o Need 2 or more oF § At least two neuroFibromas or one plexiForm neuroFibroma • PlexiForm neuroFibroma is a benign peripheral nerve tumor o Benign but carries risk oF malignant transformation unlike cutaneous neuroFibromas o PlexiForm neuroFibromas involve nerves and a nerve plexus but it is overall challenging to distinguish these form other neurofibromas o Larger lesions may be excised due to malignancy risk o If particularly large FusiForm lesion with rapid growth think malignant peripheral nerve sheath tumor § Optic nerve glioma § >6 caFé au lait spots in one year § Axillary and inguinal (intertriginous) freckles § Osseous involvement • Sphenoid wing dysplasia • Pseudoarthrosis § 2+ iris hamartoma (Lisch nodules) § First degree relative with NF1 § CAFÉ SPOT • CaFé au lait spots • Axillary/inguinal Freckling 1 Neurofibromatosis Review for Board Examination Study. -
“Study on Linear Dermatoses”
“STUDY ON LINEAR DERMATOSES” Dissertation Submitted in Partial fulfillment of the University regulations for MD DEGREE IN DERMATOLOGY, VENEREOLOGY AND LEPROSY (BRANCH XX) MADRAS MEDICAL COLLEGE THE TAMILNADU DR. M.G.R. MEDICALUNIVERSITY CHENNAI, INDIA. APRIL 2015 CERTIFICATE Certified that this dissertation titled “STUDY ON LINEAR DERMATOSES ” is a bonafide work done by Dr. P.SARASWATHY, Post-graduate student of the Department of Dermatology, Venereology and Leprosy, Madras Medical College, Chennai – 3, during the academic year 2012 – 2015. This work has not previously formed the basis for the award of any degree. Prof.K.MANOHARANMD.,D.D., Professor and Head, Department of Dermatology, Madras Medical College& Rajiv Gandhi Govt.General Hospital, Chennai-3. Prof Dr.R.Vimala M.D., Dean Madras Medical College Chennai - 3 DECLARATION I, Dr.P.SARASWATHY solemnly declare that this dissertation titled “STUDY ON LINEAR DERMATOSES” is a bonafide work done by me at Madras Medical College during 2012-2015 under the guidance and supervision of Prof. K.MANOHARAN, M.D., D.D., Professor and head department of Dermatology, Madras Medical College, Chennai-600003. This dissertation is submitted to The Tamil Nadu Dr. M.G.R. Medical University, Chennai towards partial fulfillment of the rules and regulations for the award of M.D Degree in Dermatology Venereology and Leprosy (BRANCH – XX) PLACE : DATE : (DR. P.SARASWATHY) DECLARATION The dissertation entitled “STUDY ON LINEAR DERMATOSES” is a bonafide work done by Dr. P.SARASWATHY at Department of Dermatology, Venereology and Leprosy, Madras Medical College, Chennai – 3, during the academic year 2012 – 2015 under the guidance of Professor Dr.U.R.DHANALAKSHMI M.D.,D.D,DNB., Professor, Department of Dermatology, Madras Medical College, Chennai -3. -
The Evolution of Deep Gray and White Matter MR Abnormalities
Neurofibromatosis Type 1: The Evolution of Deep Gray and White Matter MR Abnormalities Takashi ltoh, Silvia Magnaldi, Robert M. White, Martha Bridge Denckla, Karen Hofman, Sakkubai Naidu, and R. Nick Bryan PURPOSE: To investigate the evolution of deeply located high-signal-intensity abnormalities of the brain on T2-weighted MR images of patients with neurofibromatosis type 1 (NF-1 ). METHODS: The study consists of two patient groups: 1) retrospective evaluation of MR scans of 24 sympto matic NF-1 patients, 10 of whom were sequentially studied, and 2) prospective MR evaluations of 20 asymptomatic NF-1 subjects from 14 families; 2 of these families were sequentially studied. RESULTS: Deeply located, high-signal-intensity abnormalities on T2-weighted images were noted in 34 of 44 NF-1 subjects (77%). If NF-1 patients are grouped according to age, 28 of 30 subjects (93%) younger than 15 years had the lesions, whereas 4 of 7 subjects (57%) between 16 and 30 years, and 2 of 7 subjects (29%) older than 31 years had les ions. High-signal lesions in basal ganglia and brain stem were demonstrated in all decades with relatively high frequency. Lesions in the cerebellar white matter and dentate nuclei were mainly found in the patients younger than 10 years, and never found after the third decade. In 13 sequential studies (mean interval, 24 months), lesions appeared to increase in size in 3, remain unchanged in size in 2, and decrease in size in 7. One subject showed a mixed pattern of lesion size change. CONCLUSIONS: Deeply located high signal-intensity lesions on T2-weighted MR images are more evident in young NF-1 patients. -
Sturge–Weber Syndrome and Port-Wine Stains Caused by Somatic Mutation in GNAQ
T h e new england journal o f medicine original article Sturge–Weber Syndrome and Port-Wine Stains Caused by Somatic Mutation in GNAQ Matthew D. Shirley, Ph.D., Hao Tang, Ph.D., Carol J. Gallione, B.A., Joseph D. Baugher, Ph.D., Laurence P. Frelin, M.S., Bernard Cohen, M.D., Paula E. North, M.D., Ph.D., Douglas A. Marchuk, Ph.D., Anne M. Comi, M.D., and Jonathan Pevsner, Ph.D. Abstr act Background The Sturge–Weber syndrome is a sporadic congenital neurocutaneous disorder From the Biochemistry, Cellular and Mo- characterized by a port-wine stain affecting the skin in the distribution of the oph- lecular Biology Program (M.D.S., J.D.B., J.P.) and the Departments of Dermatolo- thalmic branch of the trigeminal nerve, abnormal capillary venous vessels in the gy (B.C.), Neurology (A.M.C.), Pediatrics leptomeninges of the brain and choroid, glaucoma, seizures, stroke, and intellectual (A.M.C.), and Psychiatry and Behavioral disability. It has been hypothesized that somatic mosaic mutations disrupting vas- Sciences (J.P.), Johns Hopkins School of Medicine, and the Department of Neurol- cular development cause both the Sturge–Weber syndrome and port-wine stains, ogy and Developmental Medicine, Hugo and the severity and extent of presentation are determined by the developmental time W. Moser Research Institute at Kennedy point at which the mutations occurred. To date, no such mutation has been identified. Krieger (M.D.S., J.D.B., L.P.F., A.M.C., J.P.) — all in Baltimore; the Department of Molecular Genetics and Microbiology, Methods Duke University Medical Center, Dur- We performed whole-genome sequencing of DNA from paired samples of visibly ham, NC (H.T., C.J.G., D.A.M.); and the Department of Pathology, Division of Pe- affected and normal tissue from 3 persons with the Sturge–Weber syndrome. -

Von Hippel-Lindaus Disease
VON HIPPEL-LINDAUS DISEASE REPORT OF THREE CASES AND REVIEW OF THE LITERATURE LUIZ F. BLEGGI-TORRES***, LÚCIA DE NORANHA *, J. FILLUS NETO**, JOSÉ E. QUEIROZ TELLES* *, LUIZ E. MADALOZZO* * * SUMMARY - The authors present the autopsy findings of two related patients and the biopsy findings of a thrid member of the family. The oldest member was 34 years old at death and on postmortem examination he had haemangioblastomas in the retina, cerebellum, medulla and spinal cord. Other findings were renal cell carcinoma, phaechromocytoma, cysts of kidney and pancreas, hydromyelia and atypical meningiomas. His brother died when 30 years old. The autopsy revealed haemangioblastomas of cerebellum, renal cell carcinoma and a clear cell cystadenoma of epididymus. The third patient was the daughter of the first and presented with headache and dizziness. CT-scan showed a cerebellar haemangioblastoma. Epidemiological considerations on the commonest visceral and CNS lesions and a review of current diagnostic criteria are discussed. KEY WORDS: von Hippel-Lindau's disease, angiomatosis, phakomatosis. Doença de von Hippel-Lindau: relato de três casos e revisão da literatura RESUMO - Os autores relatam os achados de autópsia de dois pacientes de uma mesma família e o diagnóstico por biópsia de hemangioblastoma de um terceiro membro desta mesma família. O primeiro paciente tinha 34 anos por ocasião do óbito e os achados de necrópsia mostraram hemangioblastoma de retina, cerebelo, bulbo e medula espinhal, além de carcinoma renal, feocromocitoma, lesões císticas de rim e pâncreas, hidromielia e meningiomas atípicos. Seu irmão morreu com 30 anos de idade e a autópsia revelou hemangioblastomas de cerebelo, carcinoma renal e cistoadenoma de células claras de epididimo.