SMALLPOX Nm:Lllpox in in Unv[Ic(.In;It .(L (Hii(L
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Vaccinia Belongs to a Family of Viruses That Is Closely Related to the Smallpox Virus
VACCINIA INFECTION What is it? Vaccinia belongs to a family of viruses that is closely related to the smallpox virus. Because of the similarities between the smallpox and vaccinia viruses, the vaccinia virus is used in the smallpox vaccine. When this virus is used as a vaccine, it allows our immune systems to develop immunity against smallpox. The smallpox vaccine does not actually contain smallpox virus and cannot cause smallpox. Vaccination usually prevents smallpox infection for at least ten years. The vaccinia vaccine against smallpox was used to successfully eradicate smallpox from the human population. More recently, this virus has also become of interest due to concerns about smallpox being used as an agent of bioterrorism. How is the virus spread? Vaccinia can be spread by touching the vaccination site before it has fully healed or by touching clothing or bandages that have been contaminated with the live virus during vaccination. In this manner, vaccinia can spread to other parts of the body and to other individuals. It cannot be spread through the air. What are the symptoms of vaccinia? Vaccinia virus symptoms are similar to smallpox, but milder. Vaccinia may cause rash, fever, headache and body aches. In certain individuals, such as those with weak immune systems, the symptoms can be more severe. What are the potential side effects of the vaccinia vaccine for smallpox? Normal reactions are mild and go away without any treatment.These include: Soreness and redness in the arm where the vaccine was given Slightly swollen, sore glands in the armpits Low grade fever One in approximately three people will feel badly enough to miss school, work or recreational activities Trouble sleeping Serious reactions are not very common but can occur in about 1,000 in every 1 million people who are vaccinated for the first time. -
Guidelines for Case-Based Reporting
澳門特別行政區 傳染病強制申報機制 Macao SAR Notifiable Communicable Diseases Guidelines for Case-based Reporting (FIRST DRAFT) 2008 澳門特別行局區政府衛生局 Health Bureau, Government of Macao Special Administrative Region ii iii Contents Contents ............................................................................................................................................................ iii Signs and abbreviations .................................................................................................................................... 5 Acquired immunodeficiency syndrome (AIDS) ............................................................................................... 6 Acute gastroenteropathy due to Norwalk agent (ICD-9 : 008.6, ICD-10 : A08.1 ) ...................................... 11 Acute haemorrhagic conjunctivitis (ICD-9 : 077, ICD-10 : B30.3 ) ............................................................. 12 Acute poliomyelitis ICD-9 045 ICD-10 A80 ................................................................................... 13 Amoebiasis ICD-9 006 ICD-10 A06 ............................................................................................... 14 Anogenital herpesviral (herpes simplex) infection ICD-9 054 ICD-10 A60 ............................... 16 Anthrax ICD-9 022 ICD-10 A22 .................................................................................................. 17 Chickenpox (Varicella) ICD-9 052 ICD-10 B01 ............................................................................ 19 Cholera ICD-9 -

12 Approved Literature List by Title Title Author Gr
K- 12 Approved Literature List by Title Title Author Gr 1984 Orwell, George 9 10 for Dinner Bogart, Jo Ellen 3 100 Book Race: Hog Wild in the Reading Room, The Giff, Patricia Reilly 1 1000 Acres, A Knoph, Alfred A. 12 101 Success Secrets for Gifted Kids, The Ultimate Fonseca, Christina 6 Handbook (BOE approved April 2014) 11 Birthdays Mass, Wendy 4 12 Ways to Get to 11 Merriam, Eve 2 2001: A Space Odyssey Clarke, Arthur 6 2002: A Space Odyssey Clarke, Arthur 6 2061: Odyssey Three Clarke, Arthur 6 26 Fairmount Avenue dePaola, Tomie 2 4 Valentines In A Rainstorm Bond, Felicia 1 5th of March Rinaldi, Ann 5 6 Titles: Eagles, Bees and Wasps, Alligators and Crocodiles, Morgan, Sally 1 Giraffes, Sharks, Tortoises and Turtles 79-Squares Bosse, Malcolm 6 A Likely Place Fox, Paula 4 A Night to Remember Lord, Waler 6 A Nightmare in History: The Holocaust 1933-1945 Chaikin, Miriam 5 A, My Name Is Alice Bayer, Jane 2 Abandoned Puppy Costello, Emily 3 Abby My Love Irwin, Hadley 6 ABC Bunny, The Gag, Wanda 1 Abe Lincoln Goes to Washington Harness, Cheryl 2 Abe Lincoln Grows Up Sandburg, Carl 6 Updated November 11, 2016 *previously approved at higher grade level 1 K- 12 Approved Literature List by Title Title Author Gr Abe Lincoln's Hat Brenner, Martha 2 Abel's Island Steig, William 3 Abigail Adams, Girl of Colonial Days Wagoner, Jean Brown 2 Abraham Lincoln Cashore, Kristen 2 Abraham Lincoln, Lawyer, Leader, Legend Fontes, Justine & Ron 2 Abraham Lincoln: Great Man, Great Words Cashore, Kristen 5 Abraham Lincoln: Our 16th President Luciano, Barbara L. -

Cidofovir Activity Against Poxvirus Infections
Viruses 2010 , 2, 2803-2830; doi:10.3390/v2122803 OPEN ACCESS viruses ISSN 1999-4915 www.mdpi.com/journal/viruses Review Cidofovir Activity against Poxvirus Infections Graciela Andrei * and Robert Snoeck Laboratory of Virology and Chemotherapy, Rega Institute for Medical Research, KULeuven, Minderboredersstraat 10, B-3000 Leuven, Belgium; E-Mail: [email protected] * Author to whom correspondence should be addressed; E-Mail: [email protected]; Tel.: +32-16-337372; Fax: +32-16-337340. Received: 10 November 2010; in revised form: 9 December 2010 / Accepted: 10 December 2010 / Published: 22 December 2010 Abstract: Cidofovir [(S)-1-(3-hydroxy-2-phosphonylmethoxypropyl)cytosine, HPMPC] is an acyclic nucleoside analog approved since 1996 for clinical use in the treatment of cytomegalovirus (CMV) retinitis in AIDS patients. Cidofovir (CDV) has broad-spectrum activity against DNA viruses, including herpes-, adeno-, polyoma-, papilloma- and poxviruses. Among poxviruses, cidofovir has shown in vitro activity against orthopox [vaccinia, variola (smallpox), cowpox, monkeypox, camelpox, ectromelia], molluscipox [molluscum contagiosum] and parapox [orf] viruses. The anti-poxvirus activity of cidofovir in vivo has been shown in different models of infection when the compound was administered either intraperitoneal, intranasal (aerosolized) or topically. In humans, cidofovir has been successfully used for the treatment of recalcitrant molluscum contagiosum virus and orf virus in immunocompromised patients. CDV remains a reference compound against poxviruses and holds potential for the therapy and short-term prophylaxis of not only orthopox- but also parapox- and molluscipoxvirus infections. Keywords: cidofovir; poxviruses; acyclic nucleoside analog 1. Introduction The antiviral activity of (S)-1-(3-hydroxy-2-phosphonylmethoxypropyl)cytosine (HPMPC, cidofovir, CDV) (Figure 1) against human cytomegalovirus (HCMV) and other DNA viruses was first Viruses 2010 , 2 2804 reported in 1986 [1]. -

The Literature of Kita Morio DISSERTATION Presented In
Insignificance Given Meaning: The Literature of Kita Morio DISSERTATION Presented in Partial Fulfillment of the Requirements for the Degree Doctor of Philosophy in the Graduate School of The Ohio State University By Masako Inamoto Graduate Program in East Asian Languages and Literatures The Ohio State University 2010 Dissertation Committee: Professor Richard Edgar Torrance Professor Naomi Fukumori Professor Shelley Fenno Quinn Copyright by Masako Inamoto 2010 Abstract Kita Morio (1927-), also known as his literary persona Dokutoru Manbô, is one of the most popular and prolific postwar writers in Japan. He is also one of the few Japanese writers who have simultaneously and successfully produced humorous, comical fiction and essays as well as serious literary works. He has worked in a variety of genres. For example, The House of Nire (Nireke no hitobito), his most prominent work, is a long family saga informed by history and Dr. Manbô at Sea (Dokutoru Manbô kôkaiki) is a humorous travelogue. He has also produced in other genres such as children‟s stories and science fiction. This study provides an introduction to Kita Morio‟s fiction and essays, in particular, his versatile writing styles. Also, through the examination of Kita‟s representative works in each genre, the study examines some overarching traits in his writing. For this reason, I have approached his large body of works by according a chapter to each genre. Chapter one provides a biographical overview of Kita Morio‟s life up to the present. The chapter also gives a brief biographical sketch of Kita‟s father, Saitô Mokichi (1882-1953), who is one of the most prominent tanka poets in modern times. -

(12) Patent Application Publication (10) Pub. No.: US 2012/0009150 A1 WEBER Et Al
US 2012O009 150A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2012/0009150 A1 WEBER et al. (43) Pub. Date: Jan. 12, 2012 (54) DIARYLUREAS FORTREATINGVIRUS Publication Classification INFECTIONS (51) Int. Cl. (76) Inventors: Olaf WEBER, Wulfrath (DE); st 2. CR Bernd Riedl, Wuppertal (DE) ( .01) A63/675 (2006.01) (21) Appl. No.: 13/236,865 A6II 3/522 (2006.01) A6IP 29/00 (2006.01) (22) Filed: Sep. 20, 2011 A6II 3/662 (2006.01) A638/14 (2006.01) Related U.S. Application Data A63L/7056 (2006.01) A6IP3L/2 (2006.01) (63) Continuation of application No. 12/097.350. filed on A6II 3/44 (2006.01) Nov. 3, 2008, filed as application No. PCTAEPO6/ A6II 3/52 (2006.01) 11693 on Dec. 6, 2006. O O (52) U.S. Cl. .......... 424/85.6; 514/350; 514/171; 514/81; (30) Foreign Application Priority Data 514/263.38: 514/263.4: 514/120: 514/4.3: Dec. 15, 2005 (EP) .................................. 05O274513 424/85.7; 514/43 Dec. 15, 2005 (EP). ... O5O27452.1 Dec. 15, 2005 (EP). ... O5O27456.2 Dec. 15, 2005 (EP). ... O5O27458.8 The present invention relates to pharmaceutical compositions Dec. 15, 2005 (EP) O5O27.460.4 for treating virus infections and/or diseases caused by virus Dec. 15, 2005 (EP) O5O27462.O infections comprising at least a diary1 urea compound option Dec. 15, 2005 (EP). ... O5O27465.3 ally combined with at least one additional therapeutic agent. Dec. 15, 2005 (EP). ... O5O274.67.9 Useful combinations include e.g. BAY 43-9006 as a diaryl Dec. -
The Secret Language of Books (A Guide to Appeal)
The Secret Language of Books 2nd edition A Guide to Appeal now with character appeal © 2015 Appeal —the “chemistry” of readers’ involve intimate knowledge of the advisory—is a way of determining why characters, or are they appealing but not people enjoy the books they read. Some especially complex? Snarky and quirky, or readers already have a good vocabulary brooding and introspective? If you don’t for talking about the books they love, mind spoilers, you can even search for while some do better talking about books unreliable narrators! they never want to read again. Framing these conversations in appeal is the This edition also reflects the regular foundation for helping people find what to and ongoing changes that we make to read next. our appeal vocabulary—we sometimes broaden or narrow the reading levels of When we added appeal terms to NoveList given terms (there really are some darkly in 2010 (building on the groundwork humorous books for preschoolers!). laid by people like Joyce Saricks, Nancy Welcome Pearl, and Neal Wyatt), we envisioned a We spend a lot of time evaluating our vocabulary that would grow and change appeal cataloging, and we welcome in response to readers, librarians, and the feedback from all librarians and readers world of books. With this “second edition,” who are willing to share with us. Seriously! we are excited to introduce a few fun My email address is vcaplinger@ebsco. changes, including character appeal! com—bring on your suggestions & questions! Our character appeal vocabulary is not intended to be an exhaustive list of Happy reading—there’s a whole character types or character names—we multiverse out there! have subject headings for that. -
The Peace Corps' Contributions to the Global Smallpox Eradication Program
The Peace Corps’ Contributions to the Global Smallpox Eradication Program About the Office of Strategic Information, Research, and Planning (OSIRP) It is the mission of OSIRP to advance evidence-based management at the Peace Corps by guiding agency strategic planning; monitoring and evaluating agency-level performance and programs; conducting research to generate new insights in the fields of international development, cultural exchange, and Volunteer service; enhancing the stewardship and governance of agency data; and helping to shape agency engagement on high-level, governmentwide initiatives. Front Cover: Peace Corps Volunteers Robert Steinglass and Doug Arbuckle administering the smallpox vaccine in Mille, Ethiopia, in 1974. Photo: Steinglass, personal collection. ii Dedication This report is dedicated to the memory of Dr. Donald Ainslie “D. A.” Henderson (September 7, 1928—August 19, 2016), a seminal figure in the field of smallpox eradication. The Peace Corps is deeply appreciative of having had the opportunity to correspond with Dr. Henderson about the contributions of Peace Corps Volunteers and returned Volunteers within the context of the global eradication program. His charismatic leadership, tireless energy, and unflagging devotion to this program inspired countless public health workers around the world, including many of the returned Peace Corps Volunteers interviewed for this report. iii Acknowledgments In 1806, approximately 10 years after Dr. Edward Jenner conducted the first documented experiment with smallpox vaccination, laying the foundations of modern medicine, President Thomas Jefferson wrote to the English physician and scientist. Jefferson acknowledged the importance of this discovery, extending “a portion of the tribute of gratitude due to you from the whole human family. -

Izu Peninsula Geopark Promotion Council
Contents A. Identification of the Area ........................................................................................................................................................... 1 A.1 Name of the Proposed Geopark ........................................................................................................................................... 1 A.2 Location of the Proposed Geopark ....................................................................................................................................... 1 A.3 Surface Area, Physical and Human Geographical Characteristics ....................................................................................... 1 A.3.1 Physical Geographical Characteristics .......................................................................................................................... 1 A.3.2 Human Geographical Charactersitics ........................................................................................................................... 3 A.4 Organization in charge and Management Structure ............................................................................................................. 5 A.4.1 Izu Peninsula Geopark Promotion Council ................................................................................................................... 5 A.4.2 Structure of the Management Organization .................................................................................................................. 6 A.4.3 Supporting Units/ Members -

Feminism and Sexed Violence in Stephen R. Donaldson
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by The University of Arizona “Violations as Profound as any Rape”: Feminism and Sexed Violence in Stephen R. Donaldson “Long ago, she had done such things [as possession]: she knew now that they were violations as profound as any rape.” Against All Things Ending, pg. 26 Introduction Few readers of Stephen R. Donaldson have missed how thoroughly sexual violence inundates his work. Rape, or the threat of rape, appears in nearly every novel and short story— the protagonist of The Chronicles of Thomas Covenant the Unbeliever (1977–2013), for example, assaults a young woman early in Lord Foul’s Bane (1977); fantasies of sexual violence obsess Castellan Lebbick in Mordant’s Need (1986–1987), and the first novel in the five-volume Gap (1991–1996) sequence easily surpasses both series in terms of sexual violence. Moreover, as my epigraph suggests, similes involving rape abound. These ubiquitous references to sexual violence can dismay even Donaldson’s most ardent proponents—fan blogger Gavrielle Perry, for example, bluntly calls them “pretty damn disturbing.” At the same time, Perry also considers Donaldson a “scrupulously non-sexist” writer, someone in whom feminists can find much to champion. More than anything, perhaps, Donaldson’s fiction advocates for the individual’s absolute power for moral choice regardless of Extrapolation, vol. 60, no. 2 (2019) https://doi.org/10.3828/extr.2019.10 sex or gender. Although female characters such as Morn Hyland and Terisa Morgan might begin as quintessential helpless beauties, they eventually develop nearly superhuman levels of agency. -
Here, There, and Everywhere: the Wide Host Range and Geographic Distribution of Zoonotic Orthopoxviruses
viruses Review Here, There, and Everywhere: The Wide Host Range and Geographic Distribution of Zoonotic Orthopoxviruses Natalia Ingrid Oliveira Silva, Jaqueline Silva de Oliveira, Erna Geessien Kroon , Giliane de Souza Trindade and Betânia Paiva Drumond * Laboratório de Vírus, Departamento de Microbiologia, Instituto de Ciências Biológicas, Universidade Federal de Minas Gerais: Belo Horizonte, Minas Gerais 31270-901, Brazil; [email protected] (N.I.O.S.); [email protected] (J.S.d.O.); [email protected] (E.G.K.); [email protected] (G.d.S.T.) * Correspondence: [email protected] Abstract: The global emergence of zoonotic viruses, including poxviruses, poses one of the greatest threats to human and animal health. Forty years after the eradication of smallpox, emerging zoonotic orthopoxviruses, such as monkeypox, cowpox, and vaccinia viruses continue to infect humans as well as wild and domestic animals. Currently, the geographical distribution of poxviruses in a broad range of hosts worldwide raises concerns regarding the possibility of outbreaks or viral dissemination to new geographical regions. Here, we review the global host ranges and current epidemiological understanding of zoonotic orthopoxviruses while focusing on orthopoxviruses with epidemic potential, including monkeypox, cowpox, and vaccinia viruses. Keywords: Orthopoxvirus; Poxviridae; zoonosis; Monkeypox virus; Cowpox virus; Vaccinia virus; host range; wild and domestic animals; emergent viruses; outbreak Citation: Silva, N.I.O.; de Oliveira, J.S.; Kroon, E.G.; Trindade, G.d.S.; Drumond, B.P. Here, There, and Everywhere: The Wide Host Range 1. Poxvirus and Emerging Diseases and Geographic Distribution of Zoonotic diseases, defined as diseases or infections that are naturally transmissible Zoonotic Orthopoxviruses. Viruses from vertebrate animals to humans, represent a significant threat to global health [1]. -
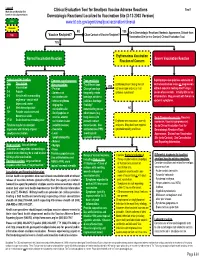
Localized to Vaccination Site (3-12-2003 Version) Low
Legend Tool 1 Morbidity and Mortality Risk Clinical Evaluation Tool for Smallpox Vaccine Adverse Reactions based on clinical presentation. Dermatologic Reactions/ Localized to Vaccination Site (3-12-2003 Version) Low www.bt.cdc.gov/agent/smallpox/vaccination/clineval Moderate NO YES Go to Dermatologic Reactions/ Nontoxic Appearance, Distant from High Close Contact of Vaccine Recipient? Vaccine Recipient? Vaccination Site (or in a Contact) Clinical Evaluation Tool. YES Erythematous Vaccination Normal Vaccination Reaction Severe Vaccination Reaction Reaction of Concern Typical reaction timeline Common signs/symptoms Tape sensitivity Rapid progressive painless extension of Day Description after vaccination Try different tape. Erythema present along lines of central vaccination lesion or progression YES 0 Vaccination - Pruritus Change bandage adhesive tape and no or mild without apparent healing after 15 days. 3-4 Papule - Soreness at frequently, rotate systemic symptoms? Lesion often necrotic. Initially little or no 5-6 Vesicle with surrounding vaccination site bandage, or take a inflammation. May present with few or no erythema - vesicle with - Intense erythema judicious bandage systemic symptoms. depressed center ringing the “holiday” 8-9 Well-formed pustule vaccination site remembering to use NO 12+ Pustule crusts over and - Small papules or other means (e.g. becomes a scab vesicles around long sleeves) to Early Progressive vaccinia (Vaccinia 17-21 Scab detaches revealing scar vaccination lesion prevent contact Erythema with induration, warmth, necrosum, Vaccinia gangrenosum) Timeline may be accelerated (satellite lesions) transmission. Use and pain. May also have regional Go to Clinical Evaluation Tool for in persons with history of prior - Headache antihistamines PRN; lymphadenopathy and fever. Dermatologic Reactions/Toxic smallpox vaccination.